
Abstract
Background
Adolescent smoking is a major public health concern, and current treatments are only somewhat effective in promoting abstinence. One way to improve treatments is to identify psychosocial characteristics that impede cessation, allowing development of targeted treatments. This study examined the influence of 2 such characteristics, life event stressors and coping, on initiation of cessation treatment and end-of-treatment abstinence status.
Methods
One hundred five adolescent smokers were eligible to participate in a validated contingency management (CM) and cognitive-behavioral (CBT) cessation treatment; of those, 72 completed at least 1 treatment session. Data included sociodemographic characteristics, questionnaires assessing past-year life events and coping behavior use, and abstinence status at the end of the 4-week treatment. Logistic regression was used to predict treatment initiation and abstinence status, with life event stressor number, coping, or their interaction as predictors.
Results
Higher levels of cognitive and peer support coping predicted treatment initiation, whereas life events were unrelated. End-of-treatment abstinence was predicted by higher numbers of life events and greater use of avoidant coping. The interaction of helpless coping and life events also predicted abstinence, with greater increases in helpless coping as total life events rose in abstinent but not nonabstinent participants. Finally, greater use of behavioral coping predicted abstinence in participants exposed to only CM treatment, whereas lesser use of behavioral coping predicted abstinence in participants receiving combined CM/CBT treatment.
Conclusions
Exposure to life event stressors may promote cessation by forcing use of self-control resources prior to the quit attempt, which may strengthen such resources. Techniques that improve self-control resources may improve cessation outcome, and prevention programs may want to emphasize behavioral coping to improve rates of treatment initiation.
Introduction
Despite improvements, adolescent smoking remains a notable public health concern. Rates of adolescent smoking have decreased since peaks in the late 1990s, 1 but rates remain unacceptably high. In 2010, 19.2% of US high school seniors had smoked in the past month, with over half of those smoking daily. Almost 90% of adult smokers initiated smoking before the age of 18, 2 indicating the importance of prevention and efforts to promote cessation in adolescence. Adolescent tobacco use is associated with symptoms of nicotine dependence, 3 nicotine withdrawal, 4 and a host of physical health–related consequences. 2 , 5 , 6 Adolescent smoking often co-occurs with, 7 , 8 and may lead to, other addictive substance use. 9 Ultimately, conservative estimates indicate that 32% of current adolescent smokers will die from a smoking-related cause later in adulthood.10
The consequences of smoking may underlie findings that most adolescent smokers want to quit, 11 with roughly 60% having attempted past-year cessation. 12 Natural rates of adolescent smoking cessation are low, however, as no more than 10% making a quit attempt achieve longer-term cessation. 11 Abstinence rates are improved by treatment, but even with validated treatments, end-of-treatment cessation is usually achieved by less than 20% of adolescents, with continued declines at follow-up assessments. 13 , 14 Thus, there is a need for improvements in current treatments, perhaps by targeting specific characteristics that impede adolescent cessation. The first step, though, is to identify barriers to treatment initiation and cessation among adolescent smokers.
Two such characteristics could be exposure to a high level of life event stressors and coping behavior. Theoretically, life stressors increase distress, reduce self-control and motivation to undertake difficult tasks, and prompt coping. 15 , 16 Whereas more adaptive coping (e.g., behavioral strategies) may ameliorate the stressor and associated distress, maladaptive coping (e.g., anger) may have no effect or even worsen distress. Substance use, including smoking, can be seen as coping, and may become a primary strategy in entrenched users. Life stressors may indirectly entrench smoking, as adolescents become reliant on the overlearned coping response of tobacco use, 17 particularly if they are prone to other forms of ineffective coping. In adults, higher levels of past-year life stressors increase the likelihood of relapse among former smokers and prevent abstinence in current smokers. 18 , 19 The role of coping in adulthood on cessation is equivocal, with evidence indicating that use of many different coping strategies 20 and planning specific coping strategies prior to the quit attempt 21 may aid cessation; conversely, no single type of coping is most effective, 20 and real-time data point to a limited role for coping during quit attempts.22
In adolescents, higher numbers of life events and/or a greater likelihood of specific life events are found in smokers, as compared with nonsmokers, 23 , 24 and initiation and persistence of smoking is predicted by higher numbers of life events. 25 , 26 For coping, lesser use of adaptive (e.g., cognitive) and greater use of maladaptive strategies (e.g., helplessness) differentiated adolescents by smoking status. 27 Wills and colleagues 24 found parental support and behavioral strategies were associated with a decreased likelihood of smoking, whereas use of anger as a coping strategy was associated with an increased likelihood. However, searches of relevant databases revealed no studies examining the influence of life stressors or coping strategies on adolescent cessation attempts. Furthermore, no relevant studies could be found that examined adolescent coping in smokers by more specific use indicators, such as nicotine dependence status or severity of smoking. That said, sex may affect adolescent coping, as females tend to use greater social support resources and avoidance than males.28
Aims and Hypotheses
The first aim of this work was to examine whether past-year stressful life events and coping behavior use predicted entry into cessation treatment among adolescents who were eligible to enter treatment following an initial screening appointment. The second aim was to examine the effects of pretreatment life events and coping on abstinence at the end of a school-based smoking cessation research intervention. 29 , 30 Finally, there were 2 exploratory aims: (1) to evaluate the interaction of life events and coping on smoking cessation outcome and treatment initiation; and (2) to evaluate whether number of past-year life events or coping behavior interacted with treatment type (i.e., cognitive-behavioral therapy [CBT] only, contingency management [CM] only, or combined CM/CBT) to predict cessation outcome.
For the first aim, we hypothesized that fewer past-year life events, higher levels of adaptive coping (e.g., behavioral), and lower levels of less adaptive coping (e.g., anger) would predict treatment initiation. For the second aim, we anticipated a similar pattern of results, with a lower number of life events, higher levels of adaptive coping and lower levels of less adaptive coping predicting end-of-treatment abstinence. Finally, we did not posit a priori hypotheses for the exploratory aims, given the lack of any research on the examined interactions.
Methods
Participants
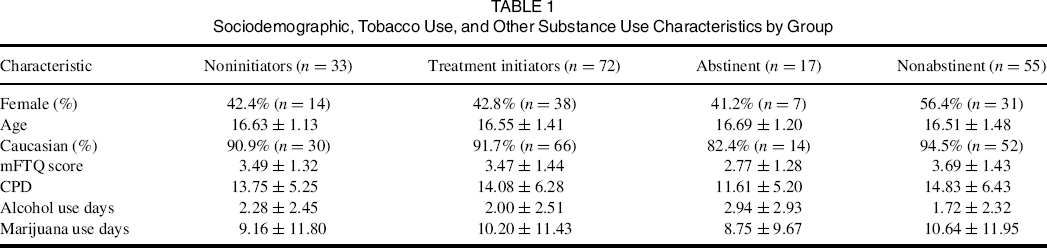
For this investigation, participants were grouped in one of two ways, with all adolescents who were eligible to participate included in one set of analyses, and participants who initiated treatment included in a separate set. One hundred fifty-seven adolescents consented to enter treatment, with 51 deemed ineligible because of below-threshold smoking or significant psychiatric illness. One individual did not have an age listed, excluding this person from analyses. Nine (8.6%) of the eligible 105 participants had 1 missing Life Events Questionnaire for Adolescents (LEQ-A) item; that item was imputed using the average of other subscale items or, for those items not in a subscale, the entire scale. Five eligible individuals (4.8%) did not complete the Response-based Coping Inventory (RBCI) and were excluded from RBCI-based analyses, and 2 other (1.9%) were missing 1 subscale and were excluded from analyses involving that subscale.
Sociodemographic, Tobacco Use, and Other Substance Use Characteristics by Group
Procedures
Data for this study came from an investigation into the efficacy of a CM- and CBT-based smoking cessation intervention for adolescent smokers. Intervention details are described in detail elsewhere. 29 – 31 Participants attended selected high schools in northeastern region of the United States, with assent/consent obtained through passive parental permission. Adolescents who appeared eligible to participate were met at their school for an initial screening session where they completed the self-report questionnaires of interest for this study in a school office with only the research assistant present. Adolescents were eligible for participation in the cessation study if they were treatment-seeking daily cigarette smokers with baseline urine cotinine levels of 350 ng/mL or greater. Eligible participants were randomized to 1 of 3 treatment groups: (1) CM-only; (2) CBT-only; or (3) combined CM/CBT. CM meetings occurred daily, whereas CBT sessions were once weekly for 30 minutes.
Measures
All measures used in this study, with the exception of 1-week point prevalence abstinence, were collected at the initial screening session (see above), prior to randomization to treatment group and treatment initiation.
One-week point prevalence abstinence at 4 weeks
Participants were abstinent if they denied past-week cigarette smoking with a qualitative urine cotinine of 100 ng/µL or lower (Graham-Massey Laboratories, Shelton, CT).
Leq-A
The Life Events Questionnaire for Adolescents 32 (LEQ-A) 67-item is a self-report measure of the presence or absence of past-year stressful life events. We combined items 33 and 34, which assess pregnancy differentially by gender. The LEQ-A provides a total score and 6 subscales, coded by discreteness of event onset (chronic or discrete), desirability (positive, negative, or ambiguous) and level of control the adolescent had (none/independent or some control/nonindependent). Across the sample, the internal consistency (Cronbach's α) of the LEQ-A was .82; Cronbach's α values for the subscales were all below .65. Because of the low internal consistencies of the original LEQ-A subscales, these were excluded from analyses. Instead, subscales were created to examine events labeled as independent, nonindependent, chronic, discrete-onset, or negative (other types had too few questions). The independent (.72) and negative events (.76) had acceptable internal consistencies and were used in analyses.
Coping
The Response-based Coping Inventory (RBCI) is a 47-item self-report 33 that uses intention-based assessment. 34 The RBCI contains 8 coping subscales: behavioral, cognitive, avoidant, angry, helpless, substance use, seeking peer support, and seeking parental support. Unpublished factor analysis by this research group in a different sample indicates that the RBCI generally fit this subscale structure. The substance use subscale was omitted here because of low internal consistency (.44). For the other subscales, Cronbach's α values ranged between .95 (parental support) and .88 (avoidant) in the entire sample.
Sociodemographic information
Participants provided information about age, sex and race/ethnicity.
Modified Fagerstrom Tolerance Questionnaire (mFTQ) 35 , 36 and Timeline Follow-back 37 measured nicotine dependence and number of days of alcohol or marijuana use in the past 28 days. These were included as covariates in regression models.
Data Analysis
Participants who were eligible to participate but did not enter treatment were compared with those who entered treatment on sociodemographic characteristics. Chi-square was used to compare sex, Mann-Whiney U was used to compare ethnicity and an independent-samples t test was used to compare age. Two sets of primary analyses were conducted, following the same plan (below): one to examine differences between those who did and did not initiate treatment and one to examine differences in end-of-treatment abstinence status among those entering treatment.
First, we examined differences in number of past-year stressful life events (i.e., LEQ-A score) based on treatment initiation or cessation outcome. If significant differences between groups were found, follow-up analyses tested for differences in LEQ-A independent or negative events. Second, we examined differences in the RBCI subscales based on treatment initiation or cessation outcome. If a significant difference was found for LEQ-A score, interaction analyses examined whether total number of stressful life events interacted with the RBCI subscales. Finally, the interaction of LEQ-A score or RCBI subscale and treatment type was examined in terms of cessation outcome at 4 weeks.
Analyses used the LOGISTIC REGRESSION command in IBM SPSS Statistics version 20 (IBM, Armonk, NY), with treatment initiation group or cessation outcome as the dependent variable and LEQ-A or RBCI score as primary predictor (independent) variable. RCBI analyses were multivariate (i.e., all subscales were included), whereas the LEQ-A analysis was univariate. All analyses controlled for sex, age, mFTQ score, and days of alcohol and marijuana use in the past 28 days; race/ethnicity was not controlled for because Caucasian participants composed over 90% of both samples. Analyses that examined cessation outcome also included treatment group (e.g., CM-only, CBT-only, or combined treatment) as a between-subject factor. Interactions between LEQ-A score and RBCI subscale entered control variables in block 1, LEQ-A score and RBCI subscale of interest in block 2, and the interaction term in block 3.
Results
Differences Based on Treatment Initiation: Sociodemographics
Of eligible participants, 72 (68.6%) initiated treatment, whereas 33 (31.4%) did not. No differences were found in any sociodemographic characteristics by treatment initiation status: sex, χ2(1, N = 105) = .97, P = .33; race/ethnicity, Mann-Whitney U = 1181.5, Z = −.09, P = .93; or age, t(103) = .38, P = .71).
Differences Based on Treatment Initiation: Stressful Life Events
Differences in Life Events and Coping Between Treatment Initiators and Noninitiators
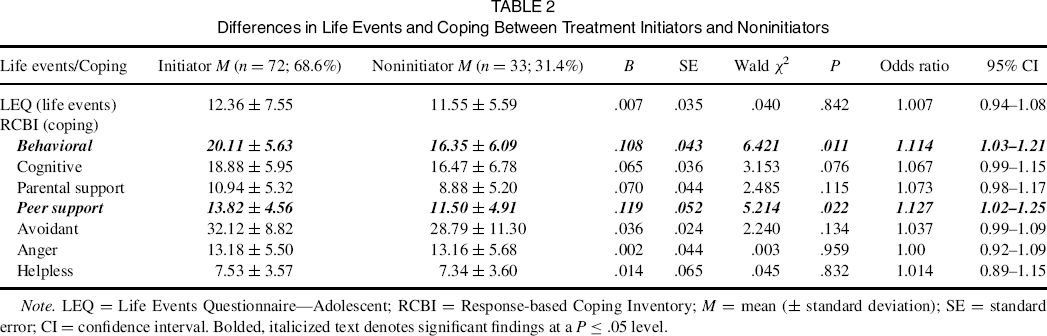
Note. LEQ = Life Events Questionnaire—Adolescent; RCBI = Response-based Coping Inventory; M = mean (± standard deviation); SE = standard error; CI = confidence interval. Bolded, italicized text denotes significant findings at a P ≤ .05 level.
Differences Based on Treatment Initiation: Coping
Two significant differences were found on RBCI subscales between treatment initiators and noninitiators. First, initiators had higher levels of behavioral coping than noninitiators, OR = 1.11, 95% CI = 1.03–1.21, with an 11% increase in odds of treatment enrollment for every point increase in behavioral coping. Also, initiators made greater use of peer support than noninitiators, OR = 1.13, 95% CI = 1.02–1.25, with a 13% increase in enrollment odds for each point increase in peer support. Also, cognitive coping displayed a trend-level difference, OR = 1.07, 95% CI = 0.99–1.15, with higher levels of cognitive coping in treatment initiators.
Differences Based on Cessation Outcome at 4 Weeks: Stressful Life Events
Differences in Life Events and Coping Based on End-of-Treatment (4-week) Cessation Status
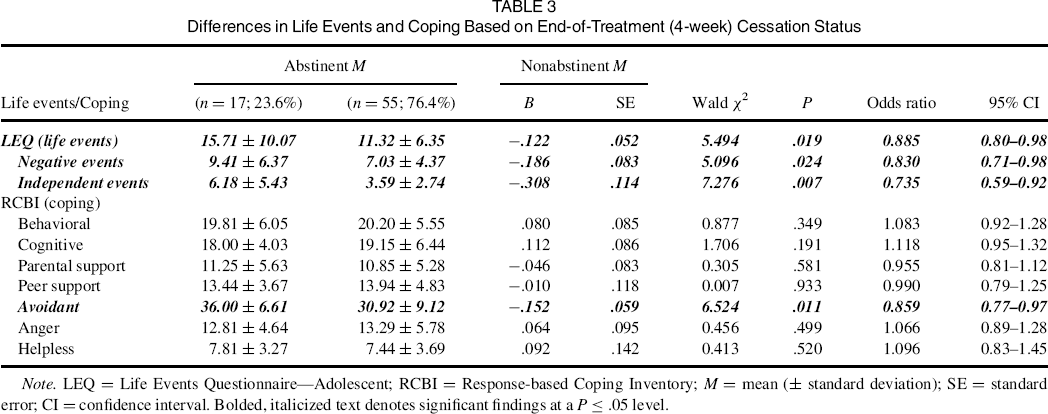
Note. LEQ = Life Events Questionnaire—Adolescent; RCBI = Response-based Coping Inventory; M = mean (± standard deviation); SE = standard error; CI = confidence interval. Bolded, italicized text denotes significant findings at a P ≤ .05 level.
Differences Based on Cessation Outcome at 4 Weeks: Coping
No significant differences (Ps < .05) were found between treatment groups in coping behavior. Analyses of coping differences on the RBCI indicated that only scores on the avoidant coping subscale differed between abstinent and nonabstinent participants, OR = 0.86, 95% CI = 0.77–0.97. Abstinent participants engaged in higher levels of avoidant coping, with a 14% increase in odds of cessation for each point on the avoidant subscale.
Interaction of Coping and Stressful Life Events on Cessation Outcome at 4 Weeks
Only one interaction between number of past-year stressful life events and RBCI subscale was found. Helpless coping interacted with LEQ score, B = −.06, SE = .03, Wald χ2 = 4.12, P = .042, such that abstinent individuals engaged in relatively little helpless coping if they had a below median number of life events (4.67 ± 1.03) and a much higher amount of helpless coping when they had an above-median number of stressful life events (9.70 ± 2.58). Nonabstinent participants had an intermediate use of helpless coping whether they experienced a below median number (7.21 ± 3.80) or an above-median number of life events (7.74 ± 3.60). This is illustrated in Figure 1.
Interaction between helpless coping and stressful life events on smoking cessation outcome.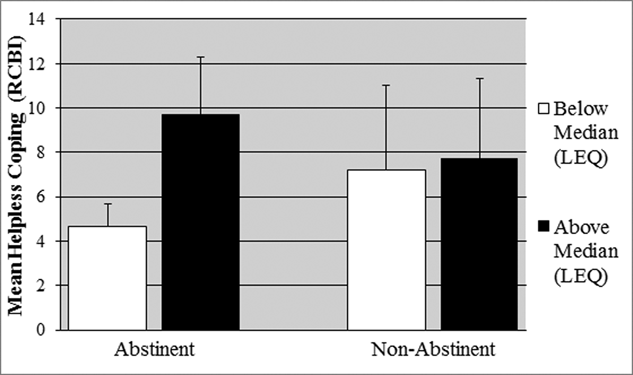
Interaction of Coping or Stressful Life Events and Treatment Group on Cessation Outcome at 4 Weeks
Since no participants in the CBT-only group achieved cessation at 4 weeks, only the CM-only and CM/CBT treatment groups were examined for the interaction of coping or stressful life events and treatment on cessation outcome. These analyses indicated that behavioral coping interacted with treatment type, B = −.352, SE = .16, Wald χ2 = 4.87, P = .027. Cessation was more likely in CM-only participants with greater behavioral coping (abstinent: 22.43 ± 6.66; nonabstinent: 18.79 ± 4.95), whereas the opposite was true in CM/CBT participants (abstinent: 17.78 ± 4.97; nonabstinent: 21.41 ± 5.85). This is illustrated in Figure 2.
Interaction between treatment type and behavioral coping on smoking cessation outcome.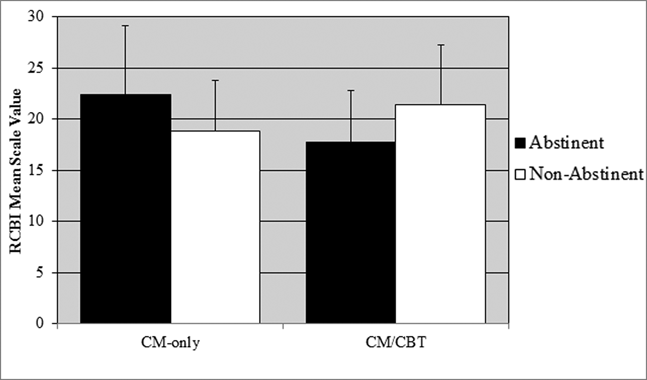
Also, peer support and cognitive coping had trend-level interactions with treatment type (peer support: B = −.408, SE = .21, Wald χ2 = 3.63, P = .057; peer support: B = −.303, SE = .17, Wald χ2 = 3.10, P = .078). Abstinent CM-only participants used greater levels of peer support than nonabstinent participants (abstinent: 14.71 ± 3.40; nonabstinent: 13.00 ± 4.72), whereas abstinent CM/CBT participants used less peer support than nonabstinent participants (abstinent: 12.44 ± 3.75; nonabstinent: 16.29 ± 3.41). For cognitive coping, CM-only participants were similar in cognitive coping use across abstinence status (abstinent: 18.00 ± 3.90; nonabstinent: 18.71 ± 6.62), whereas abstinent CM/CBT participants used greater levels than nonabstinent participants (abstinent: 17.89 ± 4.57; nonabstinent: 21.71 ± 5.00).
Discussion
In general, the hypotheses were not supported. Although initiation of cessation treatment was more likely in those who used higher levels of behavioral coping, no support was found for many of the predicted effects of life event stressors and coping on treatment initiation or cessation outcome. Unexpectedly, end-of-treatment abstinence was predicted by higher levels of past-year life events and avoidant coping. Exploratory analyses indicated that abstinence was predicted by higher levels of stressful life events combined with higher levels of baseline helpless coping or lower levels of past-year life event stressors and lower levels of helpless coping; nonabstinent adolescents had intermediate levels of helpless coping, regardless of level of past-year life events. Finally, behavioral coping interacted with treatment type for cessation at 4 weeks, with abstinent participants in the CM-only group using behavioral coping more frequently than nonabstinent participants; this pattern was reversed in CM/CBT participants.
Contrary to work in adults, 18 , 19 higher levels of life event stressors predicted abstinence at the end of a 4-week CM/CBT smoking cessation treatment. One explanation may be that adolescents with greater life stressors may value either the monetary rewards of CM or the therapeutic interaction of CBT more than other adolescents because of the likely reduction in other reinforcing events occurring in the environment of teens with greater numbers of stressful life events. CM-based reinforcers may replace some of the unavailable contingent rewards in adolescents with greater numbers of stressful life events, particularly incentivizing cessation success in order to maintain reinforcer availability. Alternatively, the work of Baumeister and Alquist 38 indicates that willpower or self-control is a dynamic resource that can be depleted, restored, and, through use of the resource, strengthened. Adolescents with higher levels of past-year life events may have had greater opportunities to exercise self-control, strengthening it. This is quite speculative, however, and further research would need to better evaluate this possibility.
Many of the coping results for treatment initiation were predicted (e.g., behavioral), but the peer support result was not necessarily anticipated. Peer support is an equivocal coping strategy vis-à-vis helping individuals resist maladaptive behaviors. Abstinent peers can promote cessation, 39 , 40 but peers who smoke discourage abstinence. 41 , 42 More unexpected was that greater use of avoidant coping encouraged cessation success. Examination of the specific avoidant coping questions indicates that many of these questions tap distraction (e.g., “I try to distract myself from the problem”), which is a relatively common adolescent cessation coping strategy. 43 Distraction may help adolescents attempting cessation avoid focusing on the adverse symptoms of nicotine withdrawal and craving, as has been posited about similar results in adult substance users. 15 Furthermore, although greater use of behavioral coping in abstinent CM-only participants was understandable given the intensity of behavioral intervention in CM, the increased use of peer support in abstinent CM-only participants was surprising. Perhaps peer support replaces the relationship between therapist and participant, supplying empathic support in the cessation attempt.
Clinical Implications
As noted previously, avoidance may serve as a proxy for distraction. Although not a perfect analogue, mindfulness strategies could help adolescents attempting cessation by increasing their ability to disengage from nicotine withdrawal sensations and craving. Indeed, mindfulness appears to help adults attempting cessation. 44 Assessing behavioral coping prior to the quit attempt may also help improve cessation rates, as CM-only treatment was most effective in those with greater behavioral coping and treatment including CBT was most effective in those with lesser levels of behavioral coping. Finally, the finding that initiation of treatment was more likely in those with higher levels of peer support coping may indicate that use of peers to encourage treatment enrollment may help teens who are considering cessation.
Limitations and Strengths
Five limitations should be noted. First, coping strategy use may have changed during treatment with CBT in some adolescents, confounding the results slightly. One of the major aims of CBT for substance use is to promote adaptive coping, 45 so coping changes are somewhat likely. Second, some data were missing for roughly 12% of individuals, potentially affecting results. Third, the sample was over 90% Caucasian, limiting generalizability to similar samples. Fourth, factors associated with entry into research-based cessation interventions may differ from those for naturalistic treatment, arguing for some caution in interpreting the treatment initiation results. Finally, post hoc power analyses indicated that the analyses of interaction effects are likely to be underpowered to detect significant results with small effect sizes. That said, this work was also strengthened by its use of a validated smoking cessation intervention, through having a wide age range of adolescents, a nearly even number of male and female participants, and its prospective design.
Conclusion
This investigation found that higher numbers of life event stressors and greater use of avoidant coping predicted smoking cessation in adolescents participating in a validated CM/CBT cessation treatment. These findings may indicate that use of distraction techniques (similar to avoidance) may help adolescents attempting cessation. Both of these hypotheses need to be evaluated in future research. More expected was that use of more adaptive coping, especially behavioral coping, promoted entry to the cessation intervention. Together, it is hoped that these results will help refine current adolescent smoking cessation treatments, reducing the significant harm and societal cost of adolescent smoking.
Footnotes
Author Contributions
This paper was derived from a parent study designed by S.K.S. and D.A.C., with conception and design of this particular investigation by T.S.S. T.S.S., D.A.C., G.K., T.L., and A.L. participated in the data collection for this study. All analyses were performed by T.S.S., and T.S.S. was also the primary author of the manuscript. All authors participated in the editing process for the manuscript, and all authors approved of its final submission.
Funding
Preparation of this paper was supported by National Institutes of Health (NIH) grant P50 DA009421. NIH (National Institute on Drug Abuse) had no further role in study design, the collection, analysis, or interpretation of data, the writing of the report, or the decision to submit the paper for publication. The authors declare that they have no conflicts of interest.