
Abstract
Background
Early onset of alcohol use has been linked to later alcohol problems in adulthood. Currently, it is not clear whether early onset of marijuana and tobacco use similarly predicts alcohol problems. Moreover, most studies examining the effect of early substance use onset on later problems only have followed youth into their early 20s. Therefore, the primary goal of this study was to examine whether early onset of alcohol, marijuana, and tobacco use predicts alcohol problems beyond the transition to adulthood.
Methods
The sample included 225 15–19-year-old youth (60% girls; 62% Caucasian) who were surveyed in three time periods: 1993–1998 (Time 1), 1998–2003 (Time 2), and 2003–2007 (Time 3). Participants reported their age of onset for regular drinking, tobacco use, and marijuana use. At each time of measurement, they also completed surveys relating to their alcohol use and abuse.
Results
Participants with an earlier age of onset of drinking regularly scored higher on the Michigan Alcoholism Screening Test (MAST) and drank more frequently to get high and drunk throughout their 20s. Tobacco use onset and marijuana use onset were not associated with later alcohol use or abuse.
Conclusions
Results from this study suggest that the relationship between the onset of substance use and later substance abuse may be substance specific. Of note, early onset of regular drinking was associated with alcohol problems during adulthood, underscoring the importance of delaying the onset of regular alcohol use among youth.
Introduction
Substance use is linked to the 3 leading causes of morbidity and mortality among youth in the United States—unintentional injury, homicide, and suicide. 1 – 3 Heavy substance use during adolescence also is associated with substance use problems during adulthood. 4 , 5 In addition, research suggests that adolescents who have an early onset of alcohol use are more likely to drink heavily and to develop alcohol problems than those who initiate alcohol use later. 6 The relationship between early substance use and later substance abuse problems may simply reflect an individual's genetic predisposition for the development of substance abuse. 7 , 8 Numerous studies have shown that individuals with a genetic predisposition for substance abuse (e.g., offspring of alcoholic parents) have an increased risk for early substance use, heavy substance use, and alcohol and drug problems. 9 , 10 Of note, this genetic predisposition may manifest differently during different developmental stages (e.g., early onset during adolescence, alcohol dependence during adulthood). Indeed, strong genetic effects have been found to contribute to both early drinking age of onset and to alcohol dependence.11,12
Other underlying mechanisms (e.g., social mechanisms such as peer selection and influence) are likely to be involved in the relationship between early substance use onset and later substance abuse as well. 13 For instance, the socially mediated hypothesis 14 suggests that the genetic relationship between early onset and later alcohol-related problems is mediated by exposure to environmental risk (e.g., through peers). Research consistently has shown that there are social mechanisms that increase the risk for substance use. 15 For example, peer use and peer support for substance use during adolescence have been found to positively predict problematic alcohol and marijuana use during early adulthood. 16 Other studies have shown that even after controlling for gender, family income, and adolescents’ baseline substance use, peer substance use predicts greater future use.17
It is important to note that to date, most research has focused on the onset of alcohol use. The onset of drug use and the interaction between the onset of alcohol and drug use on later substance use has been relatively neglected. However, some research 18 indicates that adolescents who use both alcohol and other drugs (e.g., marijuana) are at a greater risk for alcohol problems than those who use alcohol alone. Moreover, there is evidence for a common liability such that age of onset of alcohol and marijuana both may predict later alcohol use problems.19
In addition, the majority of studies focusing on the onset of substance use have used cross-sectional or short-term longitudinal designs. Although a few long-term longitudinal studies 20 , 21 have found early onset of alcohol use to be linked with later alcohol use and dependence, these studies have not followed youth beyond their early 20s.
The present study sought to extend the literature by examining age of onset of tobacco and marijuana use as well as regular drinking. In addition, youth were followed over an extensive period of time through key developmental phases associated with substance abuse risk. Research has indicated that early adulthood is a high-risk period for the development of substance use problems because it involves multiple contextual changes and changes in social roles within a brief developmental window. 22 As the individual makes the transition into early adulthood, multiple systems of the individual and the context enter a period of temporary flux. 23 Because this transition occurs within a short developmental window, marked by extensive change, 22 it may be particularly challenging for some youth. As youth negotiate these major changes, they may rely on substance use to cope. Indeed, research has shown that alcohol use accelerates during adolescence, peaks during early adulthood, and subsequently decreases. 24 Clinical substance abuse and dependence similarly peak between 18 and 23 years of age. 25 , 26 Importantly, the design of this study allowed for alcohol use and abuse to be assessed before, during, and after the transition to adulthood. The primary goal was to examine whether the onset of alcohol and drug use predicts later alcohol abuse.
Methods
Participants
All of the study participants were involved in a larger, longitudinal study (the RISK project 27 , 28 ) designed to follow offspring of alcohol- and drug-dependent fathers over time (along with a comparison group of offspring who had fathers without a substance dependence diagnosis) as the offspring progress from adolescence into adulthood. A total of 338 individuals were recruited for the larger study. This study only includes those who had complete data at all waves of measurement (n = 225). At baseline/Time 1 (1993–1998), the participating adolescents (60% girls) were 15–19 years old (mean age = 16.70 ± 1.36). Most of the adolescents were Caucasian (62%) or African American (25%), and all were from working class families in Connecticut. Approximately one half of the fathers (53%) had obtained a high school diploma. The mean household gross income was 4.69 (± 2.42) on a scale ranging from 1 = $0–$9,999/year to 9 = $150,000/year or more, which translates to about $40,000/year.
Procedures
Prior to data collection, the university's institutional review board approved the protocol. Youth were recruited from the community (e.g., presentations at high schools, Police Athletic Leagues, YMCA/YWCA) and through their parents (e.g., presentations at alcohol/drug treatment programs and support groups). Interested individuals were invited to call a research assistant for additional information and screening. Exclusion criteria included major psychiatric disorder (e.g., schizophrenia) in the father, a history of substance dependence (including alcohol) in the mother, and a history of DSM-III-R (Diagnostic and Statistical Manual of Mental Disorders, Third Edition, Revised) schizophrenia, major depressive disorder, and/or abuse/dependence on alcohol or another substance in the youth. Individuals also were excluded if they had a neurological or endocrine disorder, had a history of significant head injuries, or were currently taking a psychoactive medication. If none of the exclusion criteria applied, they were asked to come to the university study site to provide informed consent. At that time, youth completed the C-SSAGA-A clinical interview 29 (the child version of the Semi-Structured Assessment for the Genetics of Alcoholism, a psychometrically sound, clinical, diagnostic psychiatric interview that assesses 17 axis I psychiatric diagnoses and antisocial personality disorder) and a series of self-report questionnaires. 30 All of the youth were contacted for follow-up interviews and testing 5 years after the initial testing (1998–2003; Time 2; mean age = 21.35 ± 1.43) and again 5 years after Time 2 (2003–2007; Time 3; mean age = 26.10 ± 1.69). After the completion of data collection, participants received $100 at Time 1 and $150 at Time 2 and Time 3.
Measures
Onset of substance use
At Time 2, participants were asked how old they were when they began drinking regularly. More specifically, they were asked, “At what age did you begin to drink regularly; that is, drinking at least once a month for 6 months or more?” They also were asked how old they were when they first used tobacco, and when they first used marijuana. Because the distributions of these variables were skewed, they were trichotomized. For tobacco use onset, the categories were early onset = 14 years of age or younger, middle/normative onset = 15–19 years of age, and late onset = over 20 years of age. For regular drinking and marijuana use onset, the categories were early onset = 16 years of age or younger, middle/normative onset = 17–22 years of age, and late onset = over 22 years of age.
Alcohol use and abuse
At each time of measurement, participants were asked how often in the past 6 months they drank enough to “get drunk” (loss of control of physical abilities, unsteadiness, aggressiveness, or nausea) and to “get high” (drowsiness, lightheadedness, etc.). The response scale was a Likert scale ranging from 1 = “never” to 8 = “nearly every day or more often.” Participants also completed the Michigan Alcoholism Screening Test (MAST 31 ). At Time 3, they completed the Ethanol Dependence Syndrome Scale 32 as well.
Results
Power Analysis
Based on prior work within the field, it was assumed that small to medium effect sizes would be obtained. Power analyses based on a multivariate analysis of variance (MANOVA) model with a small effect size of .15 and an alpha level of .05 indicated that a sample of 177 would yield 95% power to detect a significant effect.
Multivariate Analyses
Multivariate analysis of variance (MANOVA) models were conducted to examine whether age of substance use onset predicts later alcohol abuse. Separate models were run for the dependent variables at each time of measurement. The between-subjects factors were tobacco use onset, regular drinking onset, and marijuana use onset. The dependent variables were frequency of drinking to get high, frequency of drinking to get drunk, and the MAST score. The dependence total score also was included as a dependent variable at Time 3. Listwise deletion was used to handle missing data. Only individuals who had complete data were included in the analyses.
Of note, across all times of assessment, no significant effects were found for tobacco or marijuana use onset. In addition, interactions between the substance use onset variables were not observed.
Time 1 Results
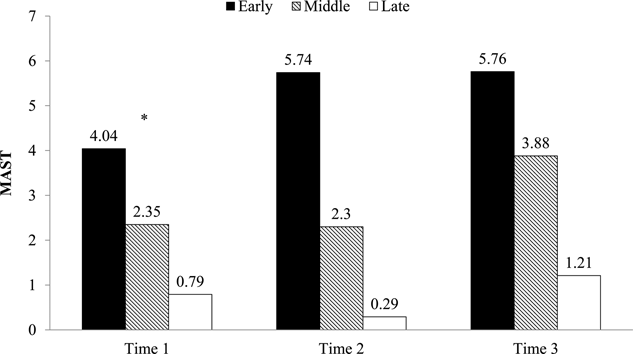
The model predicting alcohol abuse at Time 1 yielded a significant multivariate effect for the onset of regular drinking, F(6, 424) = 2.78, P < .05. As shown in Figure 1, individuals with an early onset of regular drinking drank more frequently to get high, F(2, 213) = 7.29, P < .01, and to get drunk, F(2, 213) = 5.73, P < .01. In addition, those with an early onset of regular drinking had higher MAST scores, F(2, 213) = 4.29, P < .05, in comparison with those with a later onset of regular drinking (see Figure 2).
Drinking behaviors across time by regular drinking onset. MAST score across time by regular drinking onset.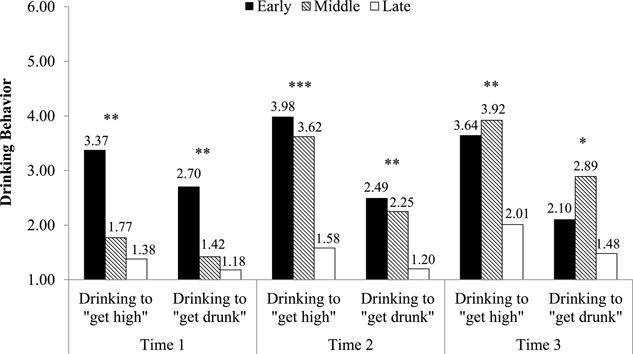
Time 2 Results
The MANOVA model predicting alcohol abuse at Time 2 from the substance use onset variables also yielded a significant multivariate effect for the onset of regular drinking, F(6, 434) = 6.28, P < .001. Results indicated that individuals with an early onset of regular drinking drank more frequently to get high, F(2, 218) = 15.38, P < .001, and to get drunk, F(2, 218) = 5.40, P < .01, during their early 20s (see Figure 1). Young adults who had an early onset of regular drinking also had higher MAST scores, F(2, 218) = 9.61, P < .001, in comparison with those with a later onset of regular drinking (see Figure 2).
Time 3 Results
The MANOVA model predicting alcohol abuse at Time 3 from the substance use onset variables yielded a significant multivariate effect for the onset of regular drinking as well, F(8, 228) = 2.09, P < .05. This model indicated that individuals with an early onset of regular drinking drank more frequently to get high, F(2, 116) = 5.76, P < .01, and to get drunk, F(2, 116) = 4.03, P < .05, during their late 20s (see Figure 1).
Discussion
Research has shown that early adulthood is a critical period for the development of substance use problems. 24 – 26 Moreover, early onset of alcohol use has been associated with a greater risk of experiencing alcohol problems during this vulnerable developmental period. 6 However, few studies have examined whether the risk of early alcohol use onset persists beyond the transition to early adulthood. Moreover, many studies have not taken into account the onset of other drugs and how they may interact with alcohol use onset to influence the risk of later alcohol problems.
The present study included both alcohol and drug use and followed a sample of 15–19-year-old adolescents through their 20s. Results indicated that individuals with an early onset of regular drinking had relatively higher MAST scores through their early 20s and drank more frequently to get high and to get drunk throughout their 20s. Importantly, results from this study indicate that the effects of early onset of regular drinking persist beyond the transition to early adulthood. These findings are in concert with prior research that has shown higher rates of alcohol dependence in individuals who begin drinking at an early age.33
Of note, tobacco and marijuana use onset did not predict later alcohol problems. Moreover, significant interactions between the onset of regular drinking and drug use onset were not observed. However, this study focused only on alcohol outcomes. Future research should examine drug outcomes to explore whether this specificity applies to other drugs over time. For example, early marijuana use onset may be linked to later marijuana abuse, but not to later alcohol abuse. It would be important for future studies to examine gender and racial/ethnic differences as well. The present study was unable to appropriately address these differences due to the relatively small size of the sample. In addition, since the overarching study was designed to follow offspring of alcohol- and drug-dependent fathers over time, the sample was a high-risk sample (ascertained through the community). As such, generalizability of the results should be made with caution. Because the study was not based on a clinical sample, an estimate of a clinical effect was not provided. Nevertheless, the findings have important clinical implications since they strongly suggest that individuals who postpone regular drinking beyond mid-adolescence experience fewer clinical symptoms of alcoholism and drink less dangerously (i.e., to intoxication/drunkenness) during their early adult years than individuals who begin regular drinking before mid-adolescence. These findings also are noteworthy, given that youth who have an early onset of alcohol use are relatively more likely to develop alcohol use disorders. 33 This study has important implications for the prevention of alcohol problems. The findings clearly indicate that delaying the onset of regular alcohol use may protect young people from developing alcohol problems during the transition to adulthood and beyond.
Footnotes
Acknowledgments
We would like to thank all of the participants in the study. We also would like to acknowledge Cheryl McCarter for her unmatched dedication to the project and Magdalena Owczarska for her help with the preparation of the manuscript.
Funding
This research was supported by National Institute on Alcohol Abuse and Alcoholism (NIAAA) grant number AA03510. The authors declare that they have no conflicts of interest.
Author Contributions
Christine Ohannessian conceptualized the study, conducted the data analyses, interpreted the results, and took the lead on writing. Laura Finan assisted with the literature review, figure construction, and revision. Jessica Schulz assisted with the literature review, writing, and revision. Victor Hesselbrock conceptualized the research project, collected the data, and provided feedback.