
Abstract
Background
Housing plays a crucial role in providing resources for and aiding an individual's reentry into the community following incarceration and substance use treatment. As such, this study examined the influence of recovery homes on a sample of former female substance-using women with criminal justice involvement.
Methods
Two hundred women who had been involved with the criminal justice system within the preceding 2 years were recruited from multiple sites in metropolitan Chicago. These women were assigned to either 1 of 2 conditions: Oxford House (OH) recovery homes or usual aftercare (UA).
Results
Those with longer stays in OH (6 months or more) had better outcomes in terms of alcohol and drug use, employment, and self-efficacy than those with shorter stays. Outcomes for those who stayed in OH were not appreciably different than the UA condition on substance use and employment, but fewer deaths occurred for those in the OH condition.
Conclusions
Findings suggest that length of stay of 6 or more months is critical for those in recovery homes, but it is important for us to better understand the processes through which longer stays influence better outcomes.
Introduction
Approximately 600,000 individuals per year are released from correctional settings; many have not received adequate mental health services, substance abuse treatment, or housing. 1 This is unfortunate, as many individuals released from incarceration have severe, long-standing substance abuse problems, 2 with active substance use representing the strongest predictor of recidivism among people in community reentry. 3 Without adequate community reentry resources, over half will recidivate.
Women in particular may benefit from reentry resources. When women are released from jail without community reentry resources to meet these needs (e.g., housing, continued substance abuse treatment, physical and mental health services), their risk increases for many types of problems. 4 A study of women in Cook County Jail, the largest single site jail in the United States, found that women's lack of stable housing was a strong predictor of incarceration. 5 Twenty-three percent of unemployed women indicated that they were unemployed because they had no place to live, and 34% were regularly involved in sex work. In addition, the majority of women surveyed were unsure of their housing options upon release.6
Several researchers maintain that the most effective interventions to prevent relapse are those that engage clients 7 and promote naturally occurring healing processes 8 (e.g., self-help treatments). Two common interventions are self-help groups and recovery homes such as Oxford House (OH). The OH model, a network of over 1700 homes in the United States, is an intervention for individuals recovering from substance use problems seeking a supportive setting with recovering peers. This model promotes the development of long-term skills to maintain abstinence. 9 OH residents are required to self-govern and assume leadership positions within their houses, according to established protocols that foster consistency across houses and create a supportive milieu. This democratic feature of OHs helps create the abstinence-specific supportive environment. Recovering individuals can live in an OH for as long as they remain abstinent and contribute to paying house expenses, which reinforces seeking and maintaining employment.
Recovery homes have been shown to extend sobriety, increasing residents’ odds of achieving longer-term recovery. 10 , 11 Although recovery homes enable residents to help sustain recovery in the community during those first crucial months of abstinence, they are not effective for all. Dropout from recovery homes hovers around 50% and commonly occurs within the first few months of residence. Dennis et al. 12 found that the odds of remaining abstinent improve as time passes; a minimum stay of about 6 months appears necessary to improve these odds. Jason et al. 13 found that those who stayed in OH for at least 6 months were less likely to relapse. It is likely that those that drop out before 6 months have an insufficient amount of time for the needed personal change to occur. For many who prematurely leave these recovery homes, drop out leads to relapse and behaviors that negatively affect their physical and mental health, relationships, employment, and ability to avoid recidivism.
Several studies demonstrate that OH represents an inexpensive aftercare model that can empower individuals in recovery through increased employment and income and decreased relapse and criminal behavior. 10 , 14 Although previous studies have found that OHs promote abstinence in several ethnic groups, 15 , 16 it is unclear whether these recovery homes are effective in reducing substance use and increasing employment among African American women who have been released from jail. The current study evaluated supportive housing services for formerly incarcerated women. We hypothesized that participants assigned to the OH condition would report increased abstinence, improved employment, and decreased rates of arrests than those assigned to the usual aftercare (UA) condition. Additionally, longer stays in OH were hypothesized to be associated with better substance use, employment, and criminal justice outcomes.
Methods
Two hundred women reporting an alcohol and/or other substance use disorder were recruited from metropolitan Chicago and its suburbs from 2008 to 2011. Recruitment sites included the Cook County Sherriff's Women's Justice Programs at Cook County Jail and various substance abuse treatment sites throughout Chicago and northern Illinois. Recruitment flyers were posted and/or distributed in multiple community-based organizations serving formerly incarcerated women or substance users. Participants were also recruited using snowball techniques. All women recruited had to report some criminal justice involvement over the past 2 years to be eligible for inclusion in the study (information on lifetime arrests and charges, as well as length of most recent incarceration, is in Table 1). All participants were enrolled in this study with institutional review board (IRB)-approved informed consent procedures that included outlining the study. Interviewers tracked and interviewed participants over a 24-month period. This study was approved by the study institution's IRB.
Sociodemographic variables of participants at baseline.
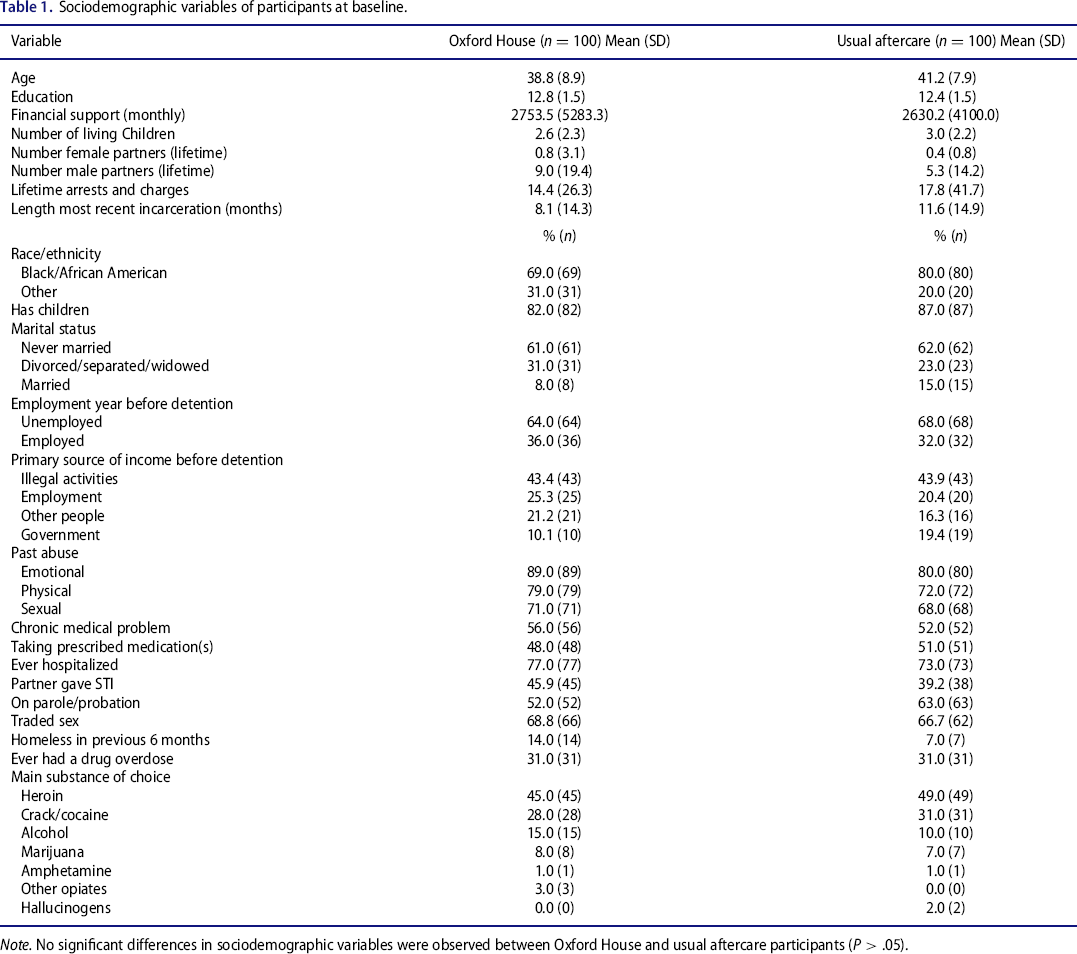
Note. No significant differences in sociodemographic variables were observed between Oxford House and usual aftercare participants (P > .05).
At baseline, we collected participants’ general demographics (e.g., race, education, marital status, housing and employment status, income history, and source of income). At baseline, participants were asked to obtain a voluntary human immunodeficiency virus (HIV) test (data not analyzed in this paper), provide tracking information in order to be followed longitudinally, and participate in an interview using a standardized survey. Participants received stipends of $45, $30, $35, $40, and $45 for participating in the initial, second, third, fourth, and fifth interviews, respectively. They also received bus cards to travel to the interview and an additional bus card if they chose to receive HIV testing.
After providing informed consent, participants were assigned into 1 of 2 groups. Usual Aftercare (UA) involved what occurred naturally after completing treatment or leaving jail (e.g., living with a relative, outpatient treatment). The Oxford House (OH) condition involved living in an OH recovery home. OHs are self-run, abstinent settings for individuals dealing with substance abuse problems. There are no resident counselors or professional staff. There are about 65 OH recovery homes in Illinois; for this study, we focused on 23 OHs in the Chicago metropolitan area. Residents may remain in these settings as long as they pay their rent, which is about $100 a week, abstain from alcohol or drug use, and comply with assigned weekly chores. Assignment was not random, as individuals were assigned to the OH condition if an opening was available at the time of recruitment. There was no systematic bias in assigning individuals into 1 of the 2 conditions.
The targeted population was quite transient, so we utilized multiple tracking strategies to find participants, including calling participants around their interview date; collecting updated contact information during each interview; sending postcards reminding participants of upcoming appointments; and contacting known associates, neighbors, and family if participants’ phones were disconnected. Staff also utilized multiple databases to find the locations of participants, and a team visited last-known addresses of participants, treatment facilities, and peer support groups.
We were provided by the Oxford House organization weekly updates on who was continuing to reside in the OHs and who had left, and these data were used to tabulate length of time in OHs. Those assigned to the OH condition stayed in these settings a mean of 131 days (SD = 14.0) and a median of 94.5 days. By the 24-month follow-up, we were able to interview the majority of the participants in each condition (OH: 86/100 = 86%, UA: 84/100 = 84%). Most attrition was due to our interviewers not being able to contact participants. Over the course of the study, 4 individuals in the UA condition died. In addition, 1 UA participant withdrew after the baseline assessment. No participants in the OH condition died. We confirmed participant death either through the participant's family, newspaper obituaries, or through various public databases when searching for the location of the participant.
Measures
Form-90 timeline follow-back17
This instrument provides a measure of alcohol and substance consumption within a 180-day time span. 18 Because our study had a 6-month follow-up, we wanted to assess all substance use occurring since the baseline assessment. The 2 primary outcome measures of the Form-90 used in this study were number of days using alcohol and number of days using drugs. As both variables had a non-normal distribution, for our analyses, we transformed alcohol use and substance use into a binary variable (use or no use during the past 6 months).
Addiction Severity Index (ASI)19
At each assessment, participants completed the 5th edition of the Addiction Severity Index—Lite. This instrument has been reliably administered in face-to-face interviews. The ASI assesses problem severity in areas affected by alcohol and substance abuse: medical and psychiatric problems, drug use, alcohol use, illegal activity, family relations, and family history. We focused on the following variables for our analysis: employed during the last 8 months, arrested or charged with a new offence at any point during the last 6 months, and awaiting charges during the last 6 months. Given that most women at baseline had been recruited from a treatment facility and were not employed, we did not have information regarding employment status at baseline.
Situational Confidence Questionnaire20
At each interview, all participants were administered the 39-item Situational Confidence Questionnaire (SCQ-39) to measure abstinence self-efficacy. The overall score of the SCQ-39 has been demonstrated to be predictive of posttreatment drinking outcome. Respondents were instructed to imagine themselves in each of 39 situations and to indicate how confident they are that they would resist the urge to use in that situation. A factor analysis by the questionnaire authors indicated 8 factor subscores: unpleasant emotions (8 items), physical discomfort (4 items), pleasant emotions (3 items), testing personal control (4 items), urges and temptations (4 items), social problems at work (3 items), social tension (5 items), and positive social situations (8 items). A confidence score is calculated for each of the 8 subscales (0% = not at all confident; 100% = very confident), each of which has excellent reliability (.81 to .97). 20 Additionally, at each wave we gave the Drug-Taking Confidence Questionnaire (DTCQ), a version of the SCQ-39 that assesses drug use in addition to alcohol use. Besides measuring drug use, the DTCQ is exactly the same as the SCQ-39—both instruments contain the same 8 subscales corresponding to Martlett's high-risk categories.21
Statistical analyses
We used a generalized linear mixed model (GLMM) to assess our major outcomes in the areas of substance use and employment. The GLMM predicts a continuous or categorical target based on 1 or more predictors. As this is a multilevel model, if the data are missing at level 2, the person is deleted. However, if the data are missing at level 1, it uses the available data and still estimates the model. This allows for nested data structures, including longitudinal designs. The main hypotheses used the intent-to-treat approach, including all participants. We report all P values, but we a priori considered levels of <.05 as significant, and all tests were 2-tailed. In our first model, we investigated whether there were condition, time, or interaction effects and investigated the effect of length of time in OH (dose). For dose, we used the continuous variable, number of days in OH (this variable produced comparable results as living in OH for fewer than 6 months and greater than or equal to 6 months). We tested models with random effects, but the Akaike information criterion corrected (AICC) and Bayesian information criterion (BIC) did not support their use. Because this was not a randomized study and there were several baseline differences between the OH and UA conditions, we used the baseline dependent variable as a covariate in the corresponding analyses.
Results
Table 1 summarizes socioeconomic data for the 2 conditions. The 2 conditions appeared to be well matched. The 200 participants in this study were predominately African American women (74.5%). The average age was 39.94 (SD = 8.58). Approximately half of the women (40.5%) reported education levels lower than a high school diploma. The majority of the women were never married (63.5%) and had had children (84.5%). The average number of children was 2.8 (SD = 2.25). The main substance of abuse for this sample was heroin (47%). At baseline assessment, 10% of the sample reported being homeless at some point in the last 6 months. More than two thirds of the sample (67.9%) reported having traded sex in their lifetime. Over half of the sample said they were currently dealing with a chronic medical problem (54.5%), and the average number of chronic medical problems was 1.8. Consistent with past research, this sample exhibited high rates of physical, emotional, and sexual abuse. Three quarters of the sample had been hospitalized in their lifetime, and about half were currently taking prescription medications.
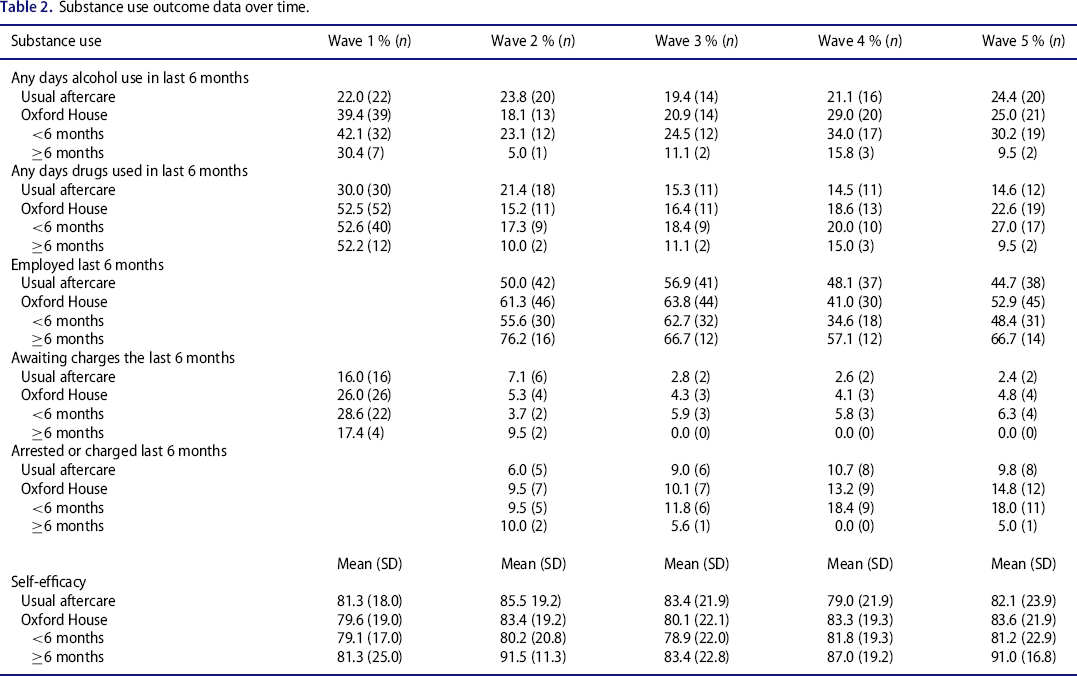
Substance use outcomes
Table 2 presents the data for use of alcohol versus no alcohol use over 6-month periods. The main effect of time was not significant, indicating that the sample over time did not evidence higher likelihood of drinking (see Table 3). The main effect of condition was not significant, indicating no significant difference between the OH and UA conditions. The condition by time interaction effect was not significant, indicating that impact of time on the probability of alcohol use did not vary by condition. The covariate, alcohol use versus no alcohol use at baseline (alcohol use as reference group), was significant, indicating that for those using alcohol at baseline, their odds of usage at subsequent waves were 2.84 (1/0.352; see Table 3) of those who did not drink. In other words, those using alcohol at baseline were over 2 times more likely to use at subsequent waves. There was a significant dose effect, indicating that number of days in an OH had a significant effect on alcohol use. Those residents with 180 days in an OH had significantly lower odds (odds ratio = exp(0.72) = 0.49) of using alcohol over time.
Substance use outcome data over time.
Generalized linear mixed model for major outcomes.
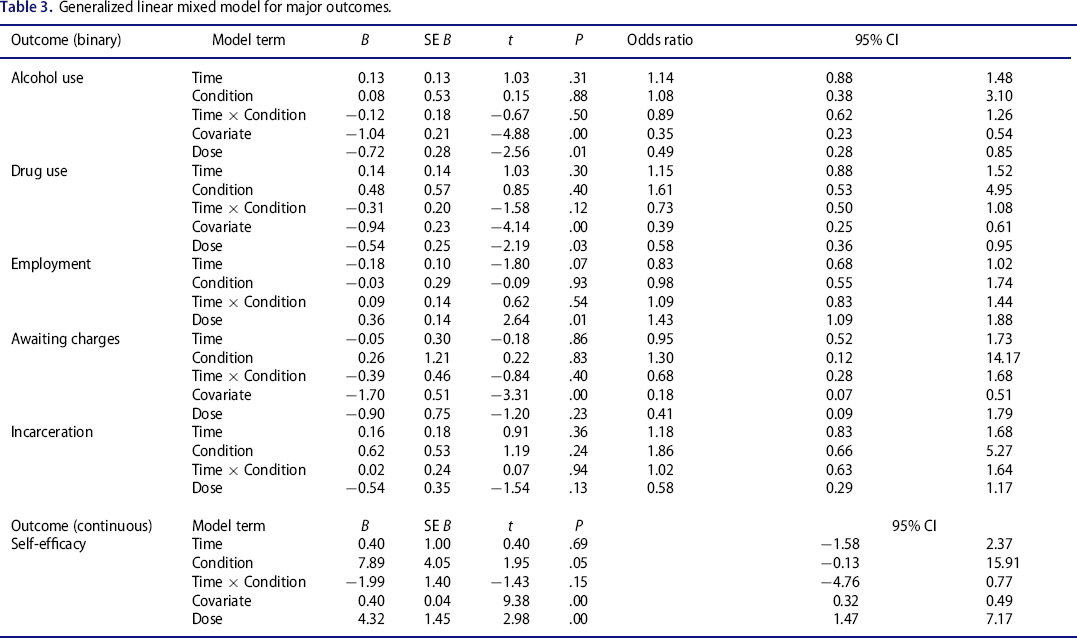
For drug use, the binary variable indicated whether drug use occurred over the past 6 months. There were no significant time, condition, or time by condition interaction effects. The covariate, baseline drug use versus no drug use, was significant, indicating that for those using drugs at baseline (drug use as reference group), their odds of usage at subsequent waves were 2.57(1/0.390; see Table 3) of those that did not use drugs. There was a significant dose effect, indicating that number of days in an OH had a significant effect on drug use. Those residents with 180 days in an OH had significantly lower odds (odds ratio = exp(−0.54) = 0.58) of using drugs over time.
Other outcome variables
For employment (whether a person was employed over the past 6 months), there were no time, condition, or time by condition interaction effects (see Tables 2 and 3). As data for the period before the baseline were not available, employment at baseline was not used as a covariate. There was, however, a significant dose effect, indicating that number of days in an OH had a significant effect on employment. Those residents with 180 days in an OH had significantly higher odds (odds ratio = exp(0.36) = 1.43) of being employed over time.
For the outcome variable awaiting criminal charges, there was not a significant time, condition, time by condition interaction, or dose effect. The covariate, awaiting criminal charges versus not awaiting criminal charges at baseline (awaiting charges as reference group), was significant, indicating that for those awaiting charges at baseline, their odds of awaiting charges were 5.46 (1/0.183; see Table 3) of those that did not await charges at subsequent waves.
For arrests or being charged with any new offense, there was no significant time, condition, time by condition interaction, or dose effects. As baseline data were not available for this variable, arrests or being charged with any new offense at baseline was not used as a covariate in this analysis.
Finally, for self-efficacy, there was not a significant time, condition, or time by condition effect, although the condition effect approached significance. Those with higher self-efficacy scores at baseline (the covariate) had significantly higher self-efficacy scores over time. Dose was significant, indicating that for every 180 days residing in OH, a resident would gain 4.32 points in self-efficacy.
Discussion
We found that for study participants, length of stay in a recovery home influenced several recovery outcomes. For individuals within the OH condition who were able to maintain residency and secure and maintain jobs for at least 6 months, outcomes were considerably better. Those able to stay at least 6 months by Wave 5 reported using alcohol or drugs less than those with less than 6 months residence in an OH. Longer-staying OH residents were also more likely to be employed and less likely to be awaiting criminal charges. Longer stays in OH also corresponded to increases in abstinence self-efficacy. It is still important to note that being assigned to recovery homes versus the UA condition did not significantly change substance abuse, employment, or arrest outcomes. However, one finding suggesting more positive overall outcomes for those in the OH condition was that no participants in this group died over the 2-year study, whereas 4 died in the UA condition.
The current study supports a prior study that found that for individuals assigned to the OH condition, those who stayed for at least 6 months had better outcomes than those who stayed less than 6 months. 7 , 13 However, the prior study also found several significant differences between OH participants and UA participants. In that prior study, at 24 months post discharge from residential treatment, 14 OH participants had lower relapse (31.6%) than UA participants (64.8%), were more likely to be employed than UA participants (76.1% vs. 48.6%), and were less likely to report engagement in illegal activities (0.9% vs. 1.8%). The reason for the differences may be due to societal and economic factors that contributed to shorter stays in OH in the current study compared to the prior study. Whereas the prior study occurred during a time in the early 2000s when there were more job opportunities, the current study began recruiting participants in 2008, at a time when there was a recession that made jobs harder to find, particularly for people in community reentry. This is critical, as one must have a source of income to remain in OHs. Additionally, a number of the OHs had recently opened in Chicago, and many of these houses eventually had to close due to problems with residents being unable to secure jobs and pay their share of expenses. In the current study, all participants had been or were currently involved with the criminal justice system, which was not the case in the prior study. In sum, these factors could have influenced the briefer stays in the current study, which impacted the overall outcomes of the study.
Our study as well as previous research has shown that individuals who participate in recovery homes for longer periods of time are better able to sustain abstinence. 22 One study found that each additional month spent in recovery homes led to a 20% increase in the odds of continued abstinence. 23 However, given that staying in recovery homes requires abstinence, it is possible that improved abstinence may be due in part to the requirements of recovery homes. It is thus important to attempt to understand the processes through which better outcomes might be generated by longer stays. 24 In our study, the finding that longer stays in OH corresponded to increased abstinence self-efficacy suggests that this is one mechanism through which recovery homes may influence continued abstinence. It is possible that longer stays in OHs provide high levels of general social support, which promotes abstinence self-efficacy among those who are faced with multiple stressors in relation to their risk behaviors, mental health, medical conditions, and financial status. Furthermore, previous research has shown that women who have social support networks that support abstinence may be more likely to maintain their recovery. 25 – 28 It is possible that longer residence in an OH communal living experience might provide residents adequate exposure to the essential abstinence social support. For instance, more experienced residents of OH may act as positive role models and advocates for recovery by showing newer residents how to respond when exposed to a variety of situations that place them at high risk for relapse (e.g., medical nonadherence, alcohol/drug cravings). In short, with 6 or more months of support, OH residents may be provided the critical support and information to enhance their abstinence self-efficacy, maintain employment, and stay abstinent. The findings of reduced mortality among OH residents may have also been impacted by some of these factors.
Although there appears to be some consensus in the literature that extended stay in recovery homes is beneficial for abstinence, we do not yet know which recovery home characteristics are associated with optimal length of stay. Also, we lack understanding of why so many residents drop out before such benefit is attained. Therefore, there is a need for future research to identify individual- and house-level conditions that promote recovery for residents. This may be especially important in a population of individuals exiting the criminal justice system, as recovery from substance use is one critical barrier to community reentry and reduction of stigma for this population.
This study had several limitations. Participants were not randomized to the 2 conditions, and it is very possible that the 2 groups differed prior to the start of the study. Indeed, those in the OH condition had higher substance use at Wave 1 than those in the UA condition. In addition, there were a number of important baseline differences that may have influenced the outcomes, although we did try to statistically control for them. We also had limited data regarding the whereabouts of those in the UA condition following recruitment into the study. Furthermore, we relied on self-report data for substance use outcomes, and having biological confirmations would have strengthened the study. Another limiting factor is the standard deviation of lifetime arrests in Table 1. Finally, the study occurred during what was considered to be the worst recession since the depression of the 1930s, and this economic climate seriously reduced the opportunities for those in the OH condition to secure employment to pay for their OH shared expenses, leading to lower lengths of stays than in prior studies.
African American women and other people of color in the criminal justice system experience multiple health risk factors such as substance abuse, poverty, involvement in abusive relationships, and mental illness. 29 – 31 Helping transition these women back to our communities so that they can resume their lives is an important objective for our society. For those with substance use disorders, halfway houses and therapeutic communities can offer professionally led environmental support following substance use treatment. However, there are limitations with these approaches, including high cost, attendant restrictions on length of stay, and the requirement that residents have completed or be involved in some type of substance abuse treatment. 32 In contrast, recovery homes are potentially lower cost, community-based residential programs for people with substance use disorders. The current study suggests that length of stay in these recovery homes is critical for more successful outcomes, and future research should focus on ways to help individuals remain in these settings for adequate periods of time.
Footnotes
Author contributions
L.J. and D.S. were involved in the research conception and design. All 3 authors were involved in the collection of data, data analysis, interpretation of the results, writing, and revision.
Funding
The authors appreciate the financial support from the National Center on Minority Health and Health Disparities (grant MD002748). This grant supported the authors during the design and conduct of the study, data analysis, and manuscript preparation. The authors declare that they have no conflicts of interest.