
Abstract
Background
Screening, brief intervention, and referral to treatment (SBIRT) is recommended as a strategy to prevent or reduce adolescent substance use. Offering SBIRT in schools may provide an opportunity to reach adolescents not accessing primary care. The objective is to assess school nurses’ attitudes and practices regarding adolescent SBIRT.
Methods
The authors administered electronically and in person a questionnaire including 29 items on SBIRT attitudes and practices to school nurses registered for the Northeastern University's School Health Institute Summer Program in Massachusetts (N = 168). Survey questions were adapted from a questionnaire originally developed by the American Academy of Pediatrics.
Results
One hundred and forty-four nurses completed the survey for a response rate of 85.7%. More than three quarters of the respondents (77.0%) were in favor of universal alcohol screening in schools. None of the respondents reported screening their students on a regular basis. More than half (64.4%) of nurses reported screening students; however, they did so only when they suspected alcohol use. During these instances, only 17.9% used a validated screening tool and almost all (98.2%) used face-to-face clinical interviews. When addressing alcohol use by a student, the large majority of respondents reported including the following recommended clinical strategies: asking about problems related to alcohol use (56.3%), explaining the harms of alcohol use (70.1%), and advising abstinence (73.6%). On average, respondents spend 5 to 10 minutes discussing alcohol use with their students.
Conclusion
Survey respondents were supportive of universal alcohol screening in school, although few were doing so at the time. When respondents identified students using alcohol, their interventions were closely aligned with clinical recommendations for brief intervention. Implementation of SBIRT that focuses on standardized, annual screening has the potential to deliver high-quality care in this setting.
Introduction
Alcohol use during adolescence accounts for a large proportion of life-years lost due to disease, disability, and premature death, 1 results in an array of chronic problems, 2 and is arguably the most important modifiable health behavior for this age group. Brief interventions delivered by medical professionals may delay initiation and reduce alcohol use by teens.3-6
Screening, brief intervention, and referral to treatment (SBIRT) is recommended as part of routine health care, 7 although adolescents have the lowest primary care utilization rates of any age group. 8 In March 2016, Massachusetts passed House Bill 4056, titled “An Act relative to substance use treatment, education, and prevention,” which requires all schools in the state to utilize a verbal screening tool annually at 2 different grade points, as approved by the Department of Public Health. 9 The Massachusetts Department of Public Health has deemed SBIRT as the approved screening practice, in an attempt to increase the number of teens who have the opportunity for a private conversation about substance use with a health care professional. 9 Effective implementation of SBIRT in schools is contingent upon the readiness and the capacity of the workforce to undertake this practice change. The objective of this report is to describe findings of a survey measuring SBIRT attitudes and screening and brief intervention practices among school nurses practicing in Massachusetts prior to the legislation requiring schools to screen all students.
Methods
Survey development
In July 2014, we administered a survey on SBIRT practices and attitudes to Massachusetts school nurses prior to their participation in a 3-day professional development summer program that concluded with 4 hours of SBIRT training. The survey was based on a questionnaire originally administered to pediatricians nationally and subsequently in Massachusetts. 10 Questions about SBIRT practices represented the common components taken from a compilation of published recommendations (Supplemental Table 1).
The brief survey was anonymous and was exempted by the Boston Children's Hospital Internal Review Board.
Participants
The School Health Institute at Northeastern University e-mailed a survey link to all nurses registered for an August 2014 training session (N = 168); nurses also had the opportunity to complete a paper survey in person prior to the training.
Analyses
Responses were entered into REDCap (Research Electronic Data Capture), cleaned in Microsoft Excel 2010, and analyzed using SPSS (version 19; IBM, Armonk, NY).
Response frequencies were computed for all variables. Respondents who answered the question “Do you screen students for alcohol use?” as “Yes, when I do physicals” or “Yes, when I suspect a child has used alcohol or has an alcohol problem” were recorded as positive for having screened. For questions that assessed frequency, responses were dichotomized as Never/Sometimes and Often/Always.
Results
Sample characteristics
Eighty-eight electronic and 56 paper surveys were received for a total of 144 completed surveys from 168 eligible participants (response rate = 85.7%). Data from 87 respondents who worked in middle and high school or only high school settings are included in this report. There were no significant differences between participants who saw middle and high school students (n = 67) compared with participants who only saw high school students (n = 20). Respondents were mostly female (87.4%), median range of nursing experience was 11 to 15 years, most (71.3%) worked in only 1 school, and 69.0% saw more than 60 students per week.
Screening attitudes and practices
Screening practices among a sample of Massachusetts school nurses.
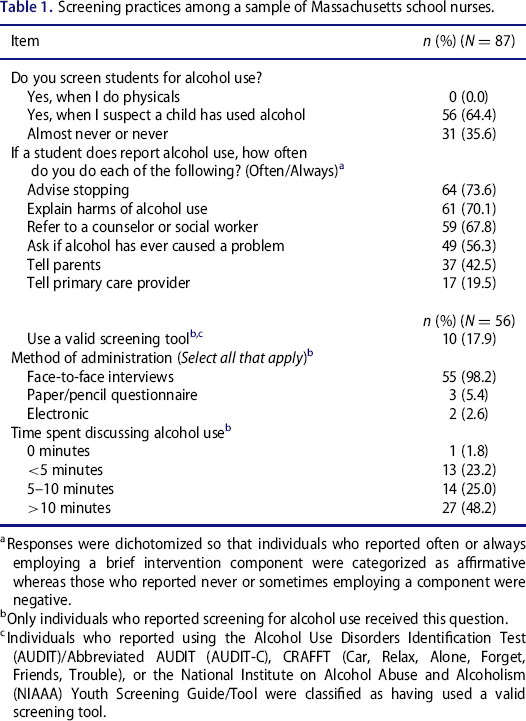
Responses were dichotomized so that individuals who reported often or always employing a brief intervention component were categorized as affirmative whereas those who reported never or sometimes employing a component were negative.
Only individuals who reported screening for alcohol use received this question.
Individuals who reported using the Alcohol Use Disorders Identification Test (AUDIT)/Abbreviated AUDIT (AUDIT-C), CRAFFT (Car, Relax, Alone, Forget, Friends, Trouble), or the National Institute on Alcohol Abuse and Alcoholism (NIAAA) Youth Screening Guide/Tool were classified as having used a valid screening tool.
Brief intervention practices
The median time spent discussing alcohol use was 5 to 10 minutes. Respondents endorsed having used the following intervention strategies: asking about alcohol-related problems (56.3%), explaining harms (70.1%), advising students to stop drinking (73.6%), referring to a counselor (67.8%), notifying parents (42.5%), and notifying primary care providers (19.5%) (Table 1).
Barriers to SBIRT
Barriers to screening among a sample of Massachusetts school nurses.
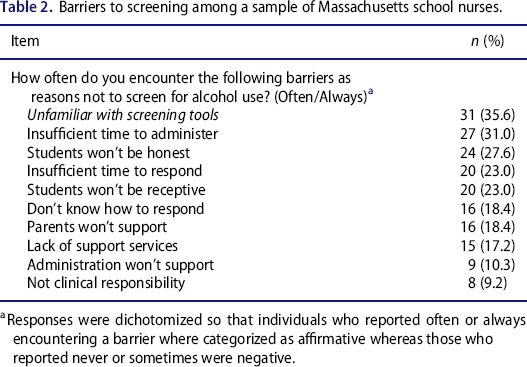
Responses were dichotomized so that individuals who reported often or always encountering a barrier where categorized as affirmative whereas those who reported never or sometimes were negative.
Discussion
A majority of this sample of Massachusetts school nurses were supportive of universal alcohol screening. Despite high levels of support, routine screening was not being employed; typical practice involved assessing and counseling students who were identified as having alcohol problems. Offering annual SBIRT in schools would present an opportunity to counsel students with alcohol problems not identified by school staff, those who have not had alcohol problems, and even those who have not used alcohol.
A large proportion of school nurse respondents endorsed use of brief intervention strategies when discussing alcohol use with students. This finding may reflect significant experience of school nurses in managing students with alcohol problems and suggests that the workforce could be readily trained to respond to students identified with substance use problems when SBIRT programs are implemented. On average, respondents spent 5 to 10 minutes discussing alcohol use. Many respondents reported inadequate time to respond to screen results, consistent with previous reports. 11 This barrier may increase if more students in need of an intervention are identified through universal screening. With the high volume of students seen by nurses, school districts may need to assess their workforce to insure adequate capacity to effectively deliver brief interventions as part of a school-based SBIRT program.
Lack of familiarity with validated screens was another barrier identified. In medical settings, clinical instincts are insensitive for identifying substance use problems. 12 Implementation of a validated screening tool that efficiently identifies risk groups could minimize the chance that early problems go undetected by clinical interview. Self-administered electronic screens are efficient and effective. 13 Use of these instruments could reduce staff time and insure fidelity and are preferred by adolescents, who may be willing to disclose more substance use in this format, 14 addressing a concern expressed by respondents.
A number of limitations to this project should be noted. The survey response rate among nurses participating in a summer educational conference was high. Nevertheless, nurses who attended the summer program may not have been representative of all school nurses in the state. It is possible that attendees’ SBIRT practices and attitudes were systematically different from those of their colleagues, although we believe this is unlikely, as the conference content was wide-ranging and did not focus exclusively on SBIRT. We used a self-report survey that asked respondents to report on whether they used recommended procedures for screening and brief intervention. The tool has been not been formally validated, although it has been used previously in other settings. 10 SBIRT recommendations that were used to form the questions were culled from guidelines designed for primary care providers rather than school nurses, as we were not aware of guidelines specifically prepared for this group. The self-report format has intrinsic limitations, including desirability bias, and it is possible that participants’ responses do not correlate with their actual practices. The sample was limited to nurses practicing in the state of Massachusetts and generalizability to other states is unknown. Despite these limitations, the findings from this report provide important considerations for the implementation of SBIRT programs within the Massachusetts Public School System.
Offering SBIRT in schools appears to have broad support among Massachusetts school nurses, although less than half of the sample reported actually conducting screening. Moreover, when screening was done, nearly all used a clinical interview rather than a validated screening tool. Use of self-administered screening tools could overcome a number of barriers identified by this group.
Footnotes
Acknowledgments
We would like to acknowledge Mary Ann Gapinski at the Massachusetts Department of Public Health for helping prepare the survey instrument and for providing feedback on this manuscript. We would also like to acknowledge, Kathy Hassey, from Northeastern University, for assisting with survey administration and support. The authors declare they have no conflicts of interest.
This study was supported by grant 5U79-TI025389 from the Substance Abuse and Mental Health Services Administration. The funding organization had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication. This study was also funded by Conrad N. Hilton Foundation (CNHF20140273) and the National Institute on Alcohol Abuse and Alcoholism (R01AA021913).
Author contributions
J.L., E.R.W., and S.L. designed and conducted the study. D.K. managed data collection. All authors contributed in the analysis and interpretation of the data. All authors drafted, revised, and approved the final manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.