
Abstract
Background
Opioid analgesics are effective and appropriate therapy for many types of acute pain. Epidemiologic evidence supports a direct relationship between increased opioid prescribing and increases in opioid use disorders and overdoses. Objective: To tailor our residency curriculum, we designed and fielded an unannounced standardized patient (USP) case involving a patient with acute back pain who is requesting Vicodin (5/325 mg). We describe residents’ case management and examine whether their management decisions, including opioid prescribing, were related to their core clinical skills.
Methods
Results are based on 50 (USP) visits with residents in 2 urban primary care clinics. Highly trained USPs portrayed a patient with acute lower back pain who was taking leftover Vicodin with effective pain relief but was running out. We describe how residents managed this case, using both USP report and chart review data, and compare summary clinical skills scores between those who prescribed Vicodin and those who did not.
Results
Of the 50 residents, 18 prescribed Vicodin (10–60 pills). Among those who did not prescribe (32/50), most (50%) prescribed ibuprofen. Eighty-three percent of the prescribers and 72% of nonprescribers ordered physical therapy (nonsignificant). Of the 18 prescribers, 13 documented checking the prescription monitoring database. Prescribers had significantly better communication scores than nonprescribers (relationship development: 80% vs. 58% well done, P = .029; patient education: 59% vs. 31% well done, P = .018). Assessment summary scores were also higher (60% vs. 46%) but not significantly (P = .060). Patient satisfaction and activation scores were higher in the prescribers than nonprescribers (71% vs. 39%, P = .004 and 48% vs. 26%, P = .034, respectively).
Conclusions
Most Vicodin prescribers did not follow prescribing guidelines, and they demonstrated better communication and assessment skills than the nonprescribers. Results suggest the need to guide residents in using a systematic approach to prescribing opioids safely and to develop an acceptable alternative pain management plan when they decide against prescribing.
Keywords
Introduction
Epidemiologic evidence supports a direct relationship between increased opioid prescribing and increases in chronic opioid use. 1 – 4 Growing recognition that the opioid epidemic is the unfortunate consequence of our efforts to adequately recognize and manage patients’ pain seems to have led to recent declines in prescriptions. 5 Yet, opioid analgesics are an effective and potentially appropriate therapy for many types of acute pain. Years of emphasis on the undertreatment of pain has given way to calls for more judicious opioid prescribing that range from guidelines to legislation.
Several states have laws limiting the quantity of opioids that may be prescribed. 6 In June 2012, the New York State legislature passed the I-STOP Act, which included deployment of an online prescription monitoring program (PMP). Effective August 2013, most prescribers were required to consult the PMP Registry when writing prescriptions for Schedule II, III, and IV controlled substances. 7 , 8 Additionally, in July 2013, the New York City Department of Health issued new opioid prescription guidelines, specifying that emergency departments should not prescribe long-acting opioid painkillers, should not prescribe more than a 3-day supply of opioid painkillers, and should not refill lost, stolen, or destroyed prescriptions. These guidelines would also apply to an individual seeking acute care in a nonemergency setting.
In order to tailor our residency education and confront the challenge of pain management in this increasingly complex landscape, we sought to describe our residents’ practices around the common outpatient clinical issue of how to manage acute pain. We designed an unannounced standardized patient (USP) case involving a person with acute back pain who is requesting Vicodin. Our study aims to systematically describe how residents manage a patient with acute pain requesting opioids and whether their management decisions were related to their core clinical skills, exploring whether residents who chose to prescribe Vicodin were different from those who did not prescribe Vicodin in terms of their communication skills, specific assessment behaviors, patient education practices, and treatment plan.
Methods
Since 2009, we have been using unannounced standardized patients (USPs) to assess our learners as well as the clinical microsystem. USPs are the medical version of “secret shoppers”—standardized patients trained to present as real patients in actual clinical settings, consistently portraying the same patient scenario. They are able to accurately and unobtrusively assess performance, providing a means for measuring responses to a standardized clinical scenario free from the bias associated with knowing that one is being observed. They have been used to assess clinical skills, residents’ professionalism in an emergency room setting, physician compliance with clinical guidelines, patients’ requests for direct-to-consumer advertised antidepressants, and the efficacy of educational interventions. 9 – 12 Other studies have explored the feasibility and validity of USPs compared with chart reviews and clinical vignettes for assessment of quality.13
Our USP program invests heavily in training of USPs, including at least 4 hours on case portrayal and 3 hours on assessment. Training includes standard-setting videos, role-play practice sessions that include both portrayal with and rating of trainees at various levels, and review of ratings to calibrate the quality of SPs’ assessment. Consistency of portrayal and quality of assessment is monitored and maintained through periodic review of audiotaped encounters (USPs carry concealed recorders), and such quality assurance reviews have found accuracy of key elements of the case to exceed 85% and agreement between original and rerating of encounters to average 80% (kappa coefficients). The risk of detection is minimized through design of realistic and common scenarios, careful casting of SPs to reflect patient populations, and the use of at least 4 actors for each case (in this case we used 5). In addition, we survey residents to elicit whether they believe they've seen a USP and ask the SPs to indicate in their assessment of each visit whether they think the visit was detected. Our detection rate for the overall USP project involving over 500 cases has been under 20%, with detection generally occurring after the visit has been completed and the resident discusses the case with a colleague.
The study was conducted in the 2 urban safety-net clinics where our residents practice: an ambulatory care clinic within the oldest continuously operating hospital in the country with 450,000 clinic visits per year, and a free-standing outpatient continuity site for residents with 270,000 clinic visits per year. The back pain/request for Vicodin case was one of a 6-case series delivered to residents that focused on important patient safety issues in the outpatient setting.
Acute back pain case description
The case involves a Caucasian woman in her early 40s with no significant past medical history presenting with complaints of acute back pain radiating down her leg for a week. For the past 4 years she has had several yearly episodes of this pain that last a week to 10 days. She is new to the clinic and because she just moved here, does not yet have medical insurance or a primary care provider. When asked, she states that she had a magnetic resonance imaging (MRI) with her previous doctor that revealed a “bulging disc.” The pain was initially relieved by ibuprofen 400 mg, 3 times a day, but that medication is no longer effective. Consequently, she began taking “leftover” Vicodin 5/325 mg pills 3 times/day, with effective pain relief. She began with 20 tablets and is now down to 4, so she is seeking a refill. (Of note, she sought care at an urgent care center a few days ago and was told to continue ibuprofen with a “muscle relaxant.”) She is very concerned because her pain (9/10 in intensity) is interfering with sleep and work. She does not smoke cigarettes, has no personal or family history of a substance use disorder or mental illness, and drinks only several alcoholic beverages weekly, if at all.
Sample
Sixty-one internal medicine residents saw the acute back pain USP; charts could not be located for 4 of these visits. Of the 57 visits with charts, 50 residents (88%) had previously provided consent for their routinely collected educational and practice data to be included in a longitudinal, de-identified database to be used for medical education research purposes (ROMEO Resident Research Registry, approved by the NYU School of Medicine institutional review board) 14 and these comprise the sample. Sixty percent of consenting residents were in the categorical internal medicine program, 40% in the primary care program (same distribution as in the full sample). Most were postgraduate year (PGY) 2 (58%; n = 29) and PGY 3 (36%; n = 18) residents, but a handful (6%; n = 3) were PGY 1 residents.
Measures
We used 2 types of assessments to describe residents’ management of this case and to explore the relationship between their management, including whether they prescribed Vicodin, and their clinical skills. USPs completed a comprehensive behaviorally anchored checklist tool that included 19 generic communication skills assessment items constituting 5 domains: information gathering (4 items), relationship development (5 items), patient education (3 items), patient activation (3 items), and patient satisfaction (4 items). These communication skills items are common to all of our USP cases, and internal consistency as measured by Cronbach's alpha for each domain is greater than or equal to .70. The acute back pain case assessment tool also employed 20 case-specific history and physical examination items.
Individual items were scored as not done, partly done, or well done, based on behavioral anchors. Summary scores were calculated for each domain as percent of items rated well done. Percent well done was chosen as the summary score in order to represent mastery of the core skills assessed in that domain. The USPs also provided open-ended responses to questions about the overall competence and professionalism of the physician.
The second source of data was from a systematic chart review of the residents’ notes and prescriptions from the electronic medical record. The chart review established actual prescription orders, referrals, and radiologic orders as well as recommended time frame for a follow-up visit.
Results
Figure 1 details the treatment patterns for our sample of residents. Of the 50 residents included in the analysis, 32 did not prescribe Vicodin, with over half recommending either continued ibuprofen or another non-narcotic analgesic such as acetaminophen or naproxen. Many prescribed gabapentin in addition to the ibuprofen. Five prescribed tramadol. Most residents, including both Vicodin prescribers and nonprescribers, also referred the patient to Physical Therapy for exercises and other pain control modalities such as cold, heat, massage, or TENS (transcutaneous electrical nerve stimulation); with many acknowledging that the wait for an appointment would be weeks to months.
Patterns of treatment for lower back pain in USP visits (N = 50).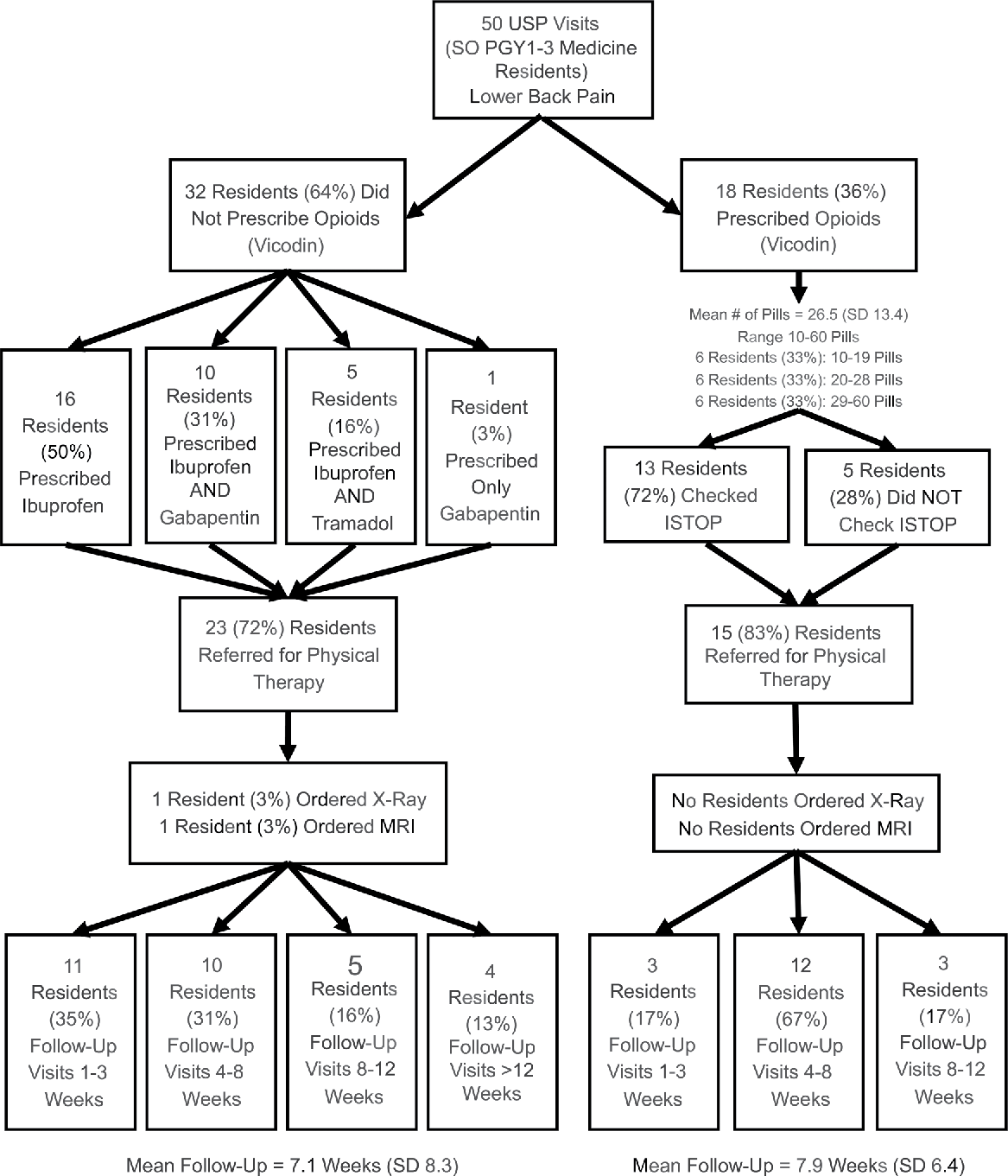
Overall clinical skill scores (% items rated well done)—Prescribers (n = 18) versus nonprescribers (n = 32).
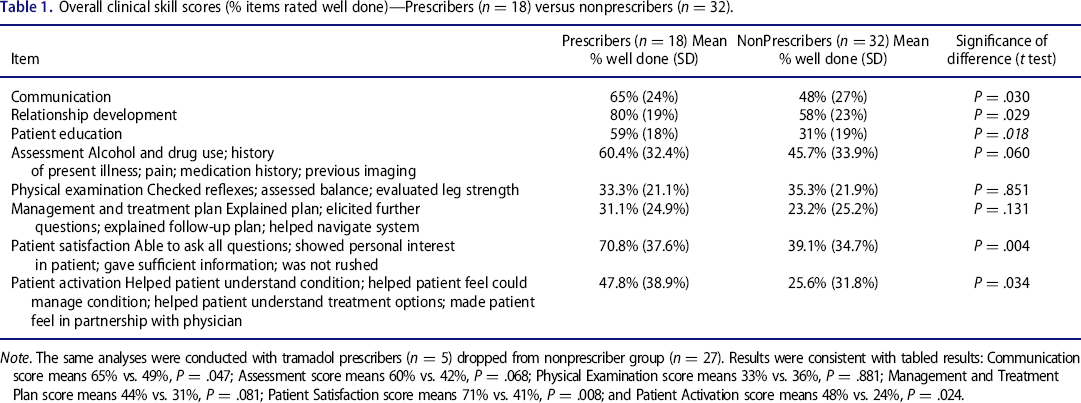
Note. The same analyses were conducted with tramadol prescribers (n = 5) dropped from nonprescriber group (n = 27). Results were consistent with tabled results: Communication score means 65% vs. 49%, P = .047; Assessment score means 60% vs. 42%, P = .068; Physical Examination score means 33% vs. 36%, P = .881; Management and Treatment Plan score means 44% vs. 31%, P = .081; Patient Satisfaction score means 71% vs. 41%, P = .008; and Patient Activation score means 48% vs. 24%, P = .024.
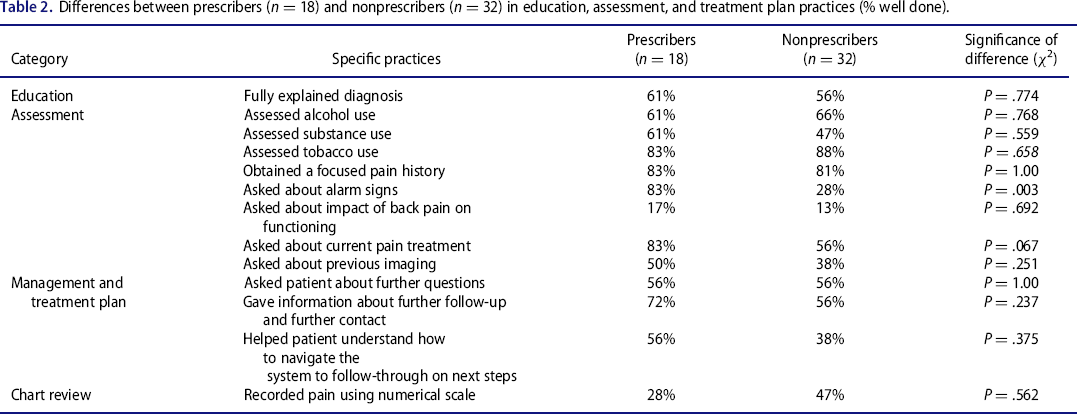
Differences between prescribers (n = 18) and nonprescribers (n = 32) in education, assessment, and treatment plan practices (% well done).
The majority of comments written by the USPs about the opioid prescribers (not shown) involved themes related to navigating the system of care, including how long it might take to get the physical therapy appointment; none commented specifically about medication and there were no negative comments about any of the 18 prescribers. Nonprescribers received similar comments about the system, but unlike prescribers, there were many comments relating to the USP's frustration with not getting Vicodin or any other new medication to relieve their pain, expressing that the patient they were playing might feel like they left the appointment no better off in terms of managing the pain.
Notably, the 50 residents were precepted by 29 different attending physicians, with each preceptor having precepted no more than 4 residents. Preceptors were scattered across the nonprescriber and prescriber groups; among those with 2 or more visits (n = 21), all but one ended up precepting both at least 1 prescribing and at least 1 nonprescribing visit. In surveys conducted over the period of the USP visits, no residents reported “detecting” this visit and only 1 USP reported suspecting that the resident might have “detected” that this was a USP visit based on an administrative snafu that led to delays in the “processing of the patient.”
Discussion
Just under 36% of the residents who saw a woman with severe acute back pain that was not relieved by a nonsteroidal anti-inflammatory drug (NSAID) and at apparent low risk for opioid use disorder prescribed the opioid she requested. Among those who prescribed, the number of pills given varied substantially and almost all prescriptions exceeded the 3-day supply recommended in the guidelines for acute care settings. 6 , 8 Most prescribers documented in the electronic medical record (EMR) that they had checked the online prescription monitoring program (PMP), although the location of documentation varied greatly, as there is no standard field for documenting this in our EMR. Opioid prescribers demonstrated better communication and more thorough assessment skills than nonprescribers. That said, many prescribers and nonprescribers did not do a thorough assessment of the patient's other substance use except for tobacco use, which is prompted by our EMR. Nonprescribers did not offer a satisfactory alternative acute pain management strategy, with most recommending that the patient continue an ineffective treatment—reflected by the low patient satisfaction scores these residents received. SPs’ comments about the encounters indicate that residents may have lacked skills to explain their treatment plan, including why they would not prescribe the requested opioid. We would like to stress that the USPs were not trained to rate the provider lower if they did not receive the Vicodin. The wide variations in care and failure in many cases to adequately address the patient's problem are especially striking, since all residents were supervised by attending physicians and trained in the same internal medicine residency program. Findings, however, cannot simply be explained by preceptor effects, as attending physicians were equally distributed across the 2 prescription groups.
There are several limitations to our study. Our USP methodology only allows us to use new patient visits in which there is no prior relationship with either the provider or the clinical site. Our sample size was small and included residents from one large internal medicine training program. Because this is a cross-sectional observational study, we can't determine direction of causality—whether those with better communication and assessment skills may be more open to Vicodin prescribing to begin with or whether better clinical skills may function to increase readiness to prescribe. Because we did not solicit residents’ feedback on the case, it is also unclear how much of a role attitudinal issues have and the influence of individual attending supervisors may have played in their prescribing behavior. We did not find differences in prescribing rates by site or resident characteristics (gender, PGY) or by SP, but we were not able to fully account for these and other related variables such as resident ethnicity given our relatively small sample size and the nature of the data contained in our educational registry.
Despite these inherent limitations, the USP acute back pain case helped uncover important skills deficits and possible knowledge and attitudinal issues with respect to treating acute pain and managing requests for opioid analgesia. Such results are perhaps not surprising given the lack of emphasis on pain education in medical school curricula 15 and our inability to find any literature reporting on formal curricula for residents on opiate prescribing for acute pain, even though there are many educational programs and guidelines addressing opioids and chronic pain. 16 , 17 Given the complexity of the current state of flux in both our knowledge and regulatory policies, curricula must be developed to help physicians to avoid both over- and underprescribing opioids in acute non-postoperative pain. 18 The American College of Physicians published evidence-based guidelines for the treatment of back pain that can inform curriculum development in this important area. 19 Based on our findings, we plan to augment our current residency and faculty development curriculum to include more content on acute pain management and opioid prescribing. Our finding that the Vicodin-prescribing group performed better in terms of communication and assessment and received higher patient satisfaction and patient activation scores aligns with suggested best practices for education and trainings that include skills-based workshops emphasizing communication skills 20 , 21 to create a supportive physician-patient relationship; and best practices for safer use of opioids when appropriate, including use of an opioid risk assessment tool. Given that virtually all of our Vicodin prescribers wrote prescriptions for more pills than guidelines deem safe and that both prescribers and nonprescribers suggested follow-up appointments with similarly long time frames on average, it is also clear that our trainees need education on the importance of prescribing a limited (3-day) supply of medication with short-term follow-up to reassess symptoms. And although many prescribers did document checking our state's online prescription monitoring database, additional training is needed to encourage consistent documentation in the most appropriate location. We will also advocate for updates to our EMR to support this.
We are not aware of any other studies that have used the USP methodology to assess pain management strategies or opioid prescribing, and our study documents the effectiveness of this method for an important patient care and safety issue. We suspect our sample of resident physicians are not unique in terms of the variation we captured in pain management practices, and we encourage others to implement focused curricula in this area and consider using USP visits to evaluate the effectiveness of pain management education and training.
Footnotes
This work was supported by US Department of Health and Human Services Health Resources and Services Administration (grant D58HP10328) and the Agency for Healthcare Research and Quality (grant R18 HS021176-03). The funding organizations had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication. The authors declare they have no conflicts of interest.
Author contributions
Drs. Hanley, Zabar, and Gillespie conceived of, implemented, and designed this study and contributed significantly to the drafting and revision of the manuscript. Dr. Gillespie conducted the data analysis. Drs. Hanley and Gillespie had full access to all of the data in the study and take responsibility for the integrity and accuracy of the data analysis. Dr. Altshuler provided substantial feedback in study design and conceptualization, supervised the data collection, and assisted in editing the manuscript. Ms. Lee, Mr. Marvilli, and Mr. Rivera participated in data collection and along with Ms. Ross assisted with writing the background.