
Abstract
Background: There has been a dramatic increase in drug overdose deaths in the United States. In the current study, the authors examined factors associated with witnessing a drug overdose. Methods: A sample of 450 substance users in Baltimore, Maryland, were recruited for a behavioral intervention and were administered a survey. Multinomial logistic regression models were used to compare participants who never witnessed a drug overdose with those who witnessed one in the prior 6 months and those who witnessed an overdose over 6 months ago. Results: Most (58%) participants were male, 40% experienced homelessness in the prior 6 months, 63% reported a history of heroin injecting, 84% had snorted heroin, 75% reported witnessing a drug overdose, and 38% experienced an overdose. In multinomial logistic regression models, witnessing an overdose in the past 6 months was associated with number of different types of places where drugs were used (adjusted odds ratio [aOR] = 1.34), history of experiencing an overdose (aOR = 1.80), injecting heroin and/or speedball (aOR = 1.78), and snorting heroin (aOR = 1.54). Witnessing an overdose more than 6 months ago was associated with number of different places where drugs were used (aOR = 1.25), history of experiencing an overdose (aOR = 1.61), snorting heroin (aOR = 1.42), and injecting heroin or speedball (aOR = 1.47). Conclusions: These data suggest that people who engage in more public and frequent drug use, and hence are more likely to witness an overdose, should be targeted for interventions to prevent and treat drug overdose.
Introduction
Drug overdose has become the major cause of injury mortality in the United States and the primary cause of death among opioid users. From 2010 to 2014, the death rate in the United States from heroin overdose more than tripled, with over 10,500 deaths in 2014. 1 Cases of hepatitis C (HCV) among those 30 and younger that were reported to the Centers for Disease Control and Prevention (CDC) more than tripled from 2006 to 2012, and over three quarters of these HCV cases reported prior injection drug use. 2 These increases in injection drug use and HCV cases coincide with increased reports of lower heroin prices and greater use of heroin. 3 - 8
It is well established that naloxone is highly effective for treating opioid overdoses. One feasibility study of bystander-administered naloxone found overdose reversal rates ranging from 75% to 100% of cases. 9 Naloxone can be administered by other drug users with minimal training and can reduce opioid overdose mortality. 10 Naloxone trainings for opioid users have documented significant increases in confidence in the ability to successfully administer naloxone and knowledge of overdose characteristics, as well as improved knowledge of actions necessary in the event of an overdose and risks associated with overdose. 10 Consequently, it is important to identify individuals who witness an opioid overdose to provide them naloxone and overdose prevention training. Research suggests that drug users are willing to administer naloxone in the event of an overdose, with the strongest associations among those who had witnessed or experienced a drug overdose themselves. 11 Findings from one study reported that those who frequently witness drug overdoses are more likely to be male, use heroin, have a prior experience of an overdose, and be embedded in drug networks. 12 Unfortunately, those who had witnessed multiple overdoses were less likely to report seeking medical assistance and more likely to report taking ineffective and potentially harmful actions, such as injecting the victim with salt or bleach, at last witnessed overdose.13
In the current study, which was the baseline assessment of opioid and cocaine users enrolled in a human immunodeficiency virus (HIV) risk reduction study, we examined factors associated with witnessing a drug overdose. We focused on drug economy activities and drug use settings frequented by urban drug users, with the goal of identifying individuals who are more likely to witness drug overdoses to target for naloxone training. We were interested in examining whether individuals who witnessed recent drug overdoses, as compared with those who had not witnessed an overdose, tended to exhibit greater levels of drug dependence, as measured by frequency of drug use, involvement in the drug economy, and using drugs in more settings.
Methods
Participants
The study recruitment and baseline interviewing were conducted from July 2009 to July 2013 in Baltimore, Maryland, as part of a randomized clinical trial for HIV prevention and care and psychological distress among inner-city substance users who reside in impoverished neighborhoods (ClinicalTrials.gov identifier: NCT01380613). Recruitment was conducted by street-based outreach, word-of-mouth, flyers, advertisements in local papers, and referrals from community agencies. Inclusion criteria for enrollment into the study were (1) aged 18–55; (2) willingness to attend intervention sessions; (3) at least 1 sexual HIV risk behavior; and (4) at least 1 drug-related HIV risk behavior. Sex risks were defined as (a) 2 or more sex partners in past 6 months; (b) a sex partner who injected drugs in past 6 months; (c) a sex partner who smoked crack in past 6 months; or (d) a sex partner who is HIV positive. Drug-related HIV risk behaviors were defined as self-reported (a) injection drug use 3 or more times in the past week, or (b) crack use in the prior 6 months. Exclusion criteria included (1) being enrolled in another HIV behavioral intervention or depression study in the past 3 years, or (2) being enrolled in another study conducted at the same research clinic in the past 5 years.
Participants provided written consent, following which a trained interviewer administered the baseline interview at a research clinic located in the community. The interview was administered face-to-face and via audio computer-assisted self-interviewing (ACASI). All study protocols and procedures were reviewed and approved by the university's institutional review board. Participants received $35 for completing the baseline interview, which lasted approximately 90 minutes. Of the 465 participants who completed the baseline survey with the drug overdose items, 15 individuals did not have complete data, resulting in a total sample size of 450 participants.
Measures
Overdose witnessing and experiencing
The 4 overdose questions included (1) “In your lifetime, how many people have you witnessed having an overdose (not including yourself)?” (2) “When was the last time you witnessed an overdose?” (3) “How many times in your life have you overdosed?” and (4) “When was your most recent overdose?” The response options were “in the last 6 months,” “in the last year,” “more than a year ago,” and “never.” Reports of last experiencing and witnessing drug overdose were then collapsed into the categories “in the last 6 months,” “over 6 months ago,” or “never.” The category of “in the last 6 months” was employed to reduce memory biases that may occur from recalling events that occurred in the distant past. The category of “greater than 6 months” was included because individuals who have never witnessed an overdose may differ from those who have ever witnessed an overdose.
Numbers of overdoses ever experienced and ever witnessed were coded from “0” to “10 or more” overdoses experienced and from “0” to “10 or more” overdoses witnessed.
Drug use
Other survey items included measures of last time participants used a particular drug, which were categorized as “in the last 6 months” (2), “over 6 months ago” (1), or “never” (0). The 2 questions on injecting heroin and injecting speedball (a combination of heroin and cocaine) were combined into a single variable to measure opiate injecting with a range of 0–4. For the combined variable, “0” indicated having never injected heroin or speedball; “1” indicated injecting either form of heroin over 6 months ago; “2” indicated injecting one form of heroin within the prior 6 months or both forms of heroin over 6 months ago; “3” indicated injecting one form of heroin over 6 months ago and the other form within the last 6 months; and “4” indicated having injected both heroin and speedball in the past 6 months.
Drug user settings
To measure the number of drug use settings, participants were asked whether they had used drugs in the following 6 settings in the past 6 months: a friend's place, shooting gallery, crack house, abandoned building, outside, or public bathroom. We conducted a polychoric factor analysis of the number of injection settings, and one clear factor emerged with an eigenvalue of 3.21. The loadings ranged from .58 to .83. Consequently, we added these 6 items together as a scale, which had a Cronbach alpha of .74 and a range of 0–6 and treated the measure as a continuous variable.
Baltimore City Health Department's Needle Exchange utilization was assessed by whether participants exchanged needles for themselves in the past 6 months. Involvement in the drug economy included the question of whether participants sold drugs in the past 30 days. Finally, response categories to the question of frequency of buying drugs in their neighborhood in the prior 6 months were “never,” “sometimes,” “always,” and “often.”
Statistical analyses
We utilized bivariate and multivariate multinomial regression models to compare those who reported never witnessing a drug overdose with those who witnessed one in the last 6 months, and with those who witnessed one over 6 months ago. All predictors were treated as continuous, and odds ratios indicated the effect of 1-level change in the predictor. Variables with statistical associations of P < .20 in the bivariate models were then included in the multivariate multinomial regression analyses.
Results
Sample characteristics
Sample characteristics stratified by witnessing an overdose among substance users in Baltimore, Maryland, USA (N = 450).
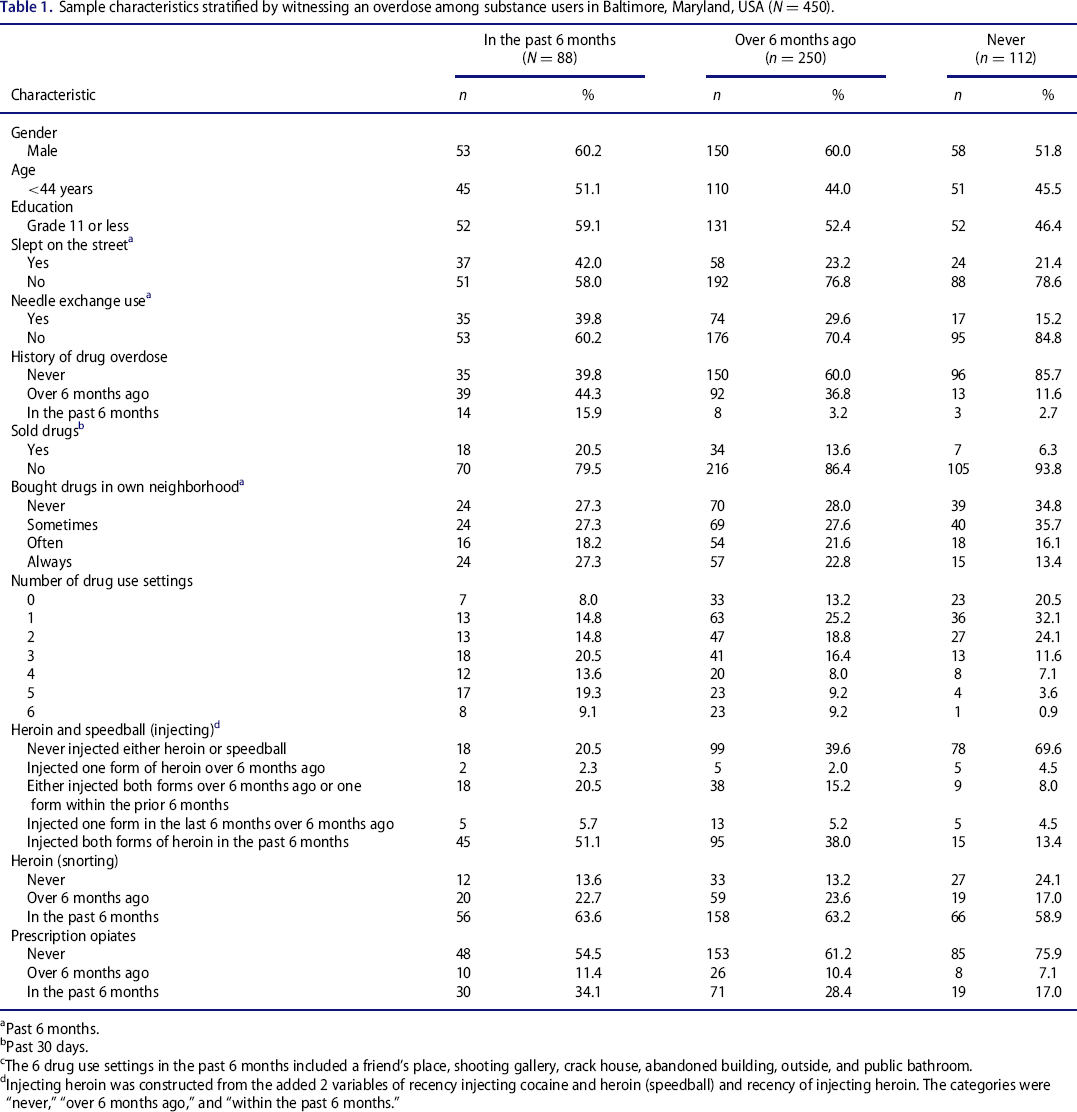
Past 6 months.
Past 30 days.
The 6 drug use settings in the past 6 months included a friend's place, shooting gallery, crack house, abandoned building, outside, and public bathroom.
Injecting heroin was constructed from the added 2 variables of recency injecting cocaine and heroin (speedball) and recency of injecting heroin. The categories were “never,” “over 6 months ago,” and “within the past 6 months.”
Witnessing an overdose
Multinomial logistic regression models of witnessing an overdose among substance users in Baltimore, Maryland, USA (N = 450).
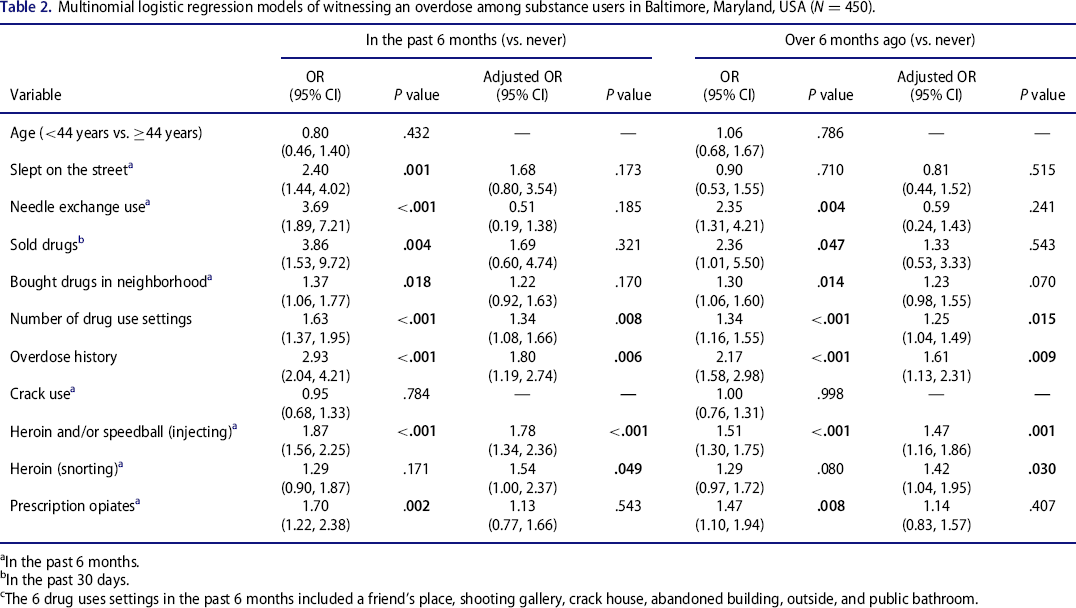
In the past 6 months.
In the past 30 days.
The 6 drug uses settings in the past 6 months included a friend's place, shooting gallery, crack house, abandoned building, outside, and public bathroom.
In the multivariate multinomial model (Table 2), witnessing an overdose in the past 6 months remained positively and significantly associated with injecting heroin or speedball (adjusted odds ratio [aOR] = 1.78), number of different types of places where drugs were used (aOR = 1.34), and history of experiencing an overdose (aOR = 1.80). Bivariate associations with sleeping on the street, needle exchange use, selling drugs, buying drugs in your neighborhood, prescription opiate use, and snorting heroin were no longer independently associated with witnessing an overdose in the past 6 months.
In the multinomial logistic regression model (Table 2), witnessing an overdose over 6 months ago was positively and significantly associated with injecting opiates (aOR = 1.47), snorting heroin (aOR = 1.42), number of different places where drugs were used (aOR = 1.25), and history of experiencing an overdose (aOR = 1.61). Bivariate associations with needle exchange use, buying drugs in your neighborhood, and prescription opiate use were attenuated and no longer independently associated with witnessing an overdose over 6 months ago.
Discussion
The study findings in the multivariate analyses suggest that individuals who have witnessed an overdose in the prior 6 months use drugs in more settings and were more likely to inject and snort heroin recently. Individuals who visit more drug use settings such as shooting galleries and crack houses are likely to be interacting with more drug users and hence have a greater opportunity to witness drug overdose. This variable may be an indication of the amount of drug use in the neighborhood. History of experiencing an overdose was also strongly associated with witnessing an overdose. This association has been found in prior research.12
In the multivariate analyses, participants who reported an overdose more than 6 months ago, as compared with those who had never witnessed an overdose, were more likely to use drugs in a greater number of settings, were more likely to recently inject and snort heroin, and were more likely to report that they had a history of a drug overdose. In the bivariate analyses, there were several significant differences between those who reported overdosing in the prior 6 months compared with those who had never overdosed, and those who reported overdosing more than 6 months ago compared with those who had never overdosed. However, in the multivariate analyses, these differences were attenuated.
It is likely that some of the items that were found to be statistically significant are tapping into the construct of severity of drug dependence. Greater drug severity of dependence may lead to interacting with more drug users and frequenting more drug use settings. Both are likely to lead to a greater chance of witnessing a drug overdose.
The study findings suggest the potential value of identifying and training individuals in overdose prevention and care who use drugs in more types of settings. The value of training drug users who frequent a variety of injection settings is also supported by previous research that found overdoses witnessed in public and/or abandoned buildings, compared with one's home, were more likely to be fatal.13
It is interesting to note that in both multivariate models, needle exchange use was no longer statistically significant. Since the frequency of injecting is the major reason why persons who inject drugs go to needle exchanges, these findings do not negate the importance of utilizing needle exchange as an avenue for overdose prevention and care training. In several cities, needle exchange has been successfully utilized as a venue to recruit drug users for naloxone training.14
Overdose training programs can be effective in leading to the appropriate use of naloxone. At the time of this study, Baltimore City Health Department had instituted naloxone training linked to their syringe exchange program. Since May 2017, a standing order for naloxone has made it available without a prescription, yet it can still be expensive for individuals depending on their health insurance status and type of insurance. Moreover, with the increase in the distribution of fentanyl, drug overdose fatalities have greatly increased in Baltimore and elsewhere in the United States. 15 , 16 This trend suggests the need to train more individuals quickly, as well as target individuals who frequent common injection settings, such as shooting galleries and abandoned buildings. Because fentanyl is a rapidly acting opioid and may require greater amounts of naloxone to reverse its effects, overdose prevention should also emphasize not injecting alone. For individuals who hide their drug use, it is important to train them in skills for disclosing their drug use as well as facilitate drug treatment and naloxone administration training for family members and friends. The establishment of safe drug consumption spaces is another important approach to reduce drug overdose fatalities.
A limitation of the current study is that we do not know what percentage of reported overdoses were due to opiates, rather than alcohol, benzodiazepines, or other drugs that will not respond to naloxone. In this study, 94% of participants were opiate users, which suggests that opiate use was involved in the vast majority of overdoses. It is likely that a large proportion of participants were using substances in addition to opiates. 17 – 19 Toxicology tests may provide accurate information on fatal overdose and those who were treated in medical facilities, but toxicology results are not available to those witnessing an overdose.
There are several other limitations that should be noted. We may have missed key factors among drug users who had a fatal overdose. We also do not know how the question about witnessing drug overdoses was interpreted. For example, participants may or may not have interpreted the observation of someone unconscious as an overdose victim. It is likely that contextual factors associated with overdoses among inner-city opiate users may not generalize to rural and suburban drug users. These results do suggest that regardless of the context, it may be important to examine drug use settings and roles in the drug economy.
Future studies should examine drug overdose in rural contexts, which in the United States have seen sharp increases in nonmedical prescription drug and heroin use and overdose. Such studies should also examine the concordance between observers’ and victims’ overdose reports. However, a critical issue for future research and public health programs is first to identify individuals who are at risk of or witnesses to overdose and to overcome barriers to training and providing these individuals with naloxone. In addition, we must ensure that opioid users do not use alone and have access to low-threshold and effective drug treatment programs that include overdose prevention and care training. In conclusion, the study results suggest that drug users who inject in more types of settings are also more likely to witness a drug overdose. The study results also indicate that there are a cluster of factors associated with witnessing drug overdoses, and future research should try to disentangle these factors. However, regardless of the causal pathways leading to witnessing drug overdoses, it is critical to increase the reach and coverage of naloxone distribution and other methods of drug overdose prevention and care.
Footnotes
Author contributions
All authors contributed to the manuscript. C.A.L., K.E.T., and M.A.D-R. were responsible for the proposal, securing funding, and drafting the protocol. C.A.L., Principal Investigator, supervised all aspects of the study and conducted the statistical analyses. C.E. assisted with the data interpretation. C.A.L. and C.E. worked on the initial draft of the manuscript. All authors contributed to, and approved, the final manuscript.
Funding
Grant DA022961 of the National Institute on Drug Abuse, National Institutes of Health, supported this research. The funding organization had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.