
Abstract
Background
Syringe exchange programs are uniquely positioned to offer treatment services to interested clients. Prevention Point Philadelphia recently expanded to offer buprenorphine maintenance treatment through its Stabilization, Treatment, and Engagement Program (STEP). Objective: To describe the STEP model of care and report treatment outcomes.
Methods
Retrospective chart review of patients enrolled in STEP (October 2011-August 2014). Our main outcome measure was time retained in treatment, defined as time from treatment initiation to treatment failure. Secondary outcome measures were buprenorphine and opiate use, from urine toxicology screens. We analyzed retention in treatment using Kaplan-Meier survival estimates; patients who remained in treatment at the end of the study period were censored on that day. For buprenorphine and opiate use, we calculated the percentage of patients who were positive for buprenorphine and opiates in each month of treatment.
Results
Of the 124 patients enrolled in STEP, the median age was 41 (range 21 to 63) and 80% reported injection heroin use. Comorbidities were common: 33% had HIV infection, most reported anxiety (78%) or depression (71%), and 20% were homeless. The most common program outcomes were unplanned self-discharge (n = 29; 23%), incarceration (n = 20; 16%), and administrative discharge (n = 19; 15%). The percentage of patients retained in treatment at 3, 6, 9, and 12 months was 77%, 65%, 59%, and 56%, respectively. Among those retained, the percentage with a positive buprenorphine screen at 3, 6, 9, and 12 months was 88%, 100%, 96%, and 95%, respectively. The percentage with a positive opiates screen was 19%, 13%, 17%, and 16%, respectively.
Conclusions
With a program that blended organizational and community resources, retention in buprenorphine maintenance treatment was comparable to retention rates reported from other settings. Further research should directly compare treatment outcomes in syringe exchange program-based settings versus primary care and specialty settings.
Keywords
Introduction
Rates of heroin use, use disorder, and overdose have increased rapidly throughout the United States.1,2 Philadelphia, a major northeastern city, is facing similar trends.3 Despite the scale of the problem, many people with heroin use disorder do not receive effective medication treatment because of limited capacity, financial obstacles, social bias, and other barriers to care.4-8 Syringe exchange programs (SEP) may serve as alternative, or even preferred, venues for treatment;9 however, the ability of such programs to provide heroin use disorder treatment to socially and medically complex patients is largely unknown.
In 1991, Prevention Point Philadelphia founded a community-based SEP to address the high incidence of HIV and hepatitis C infection among people who inject heroin. Its core services include harm reduction through syringe distribution and exchange, overdose education and naloxone distribution, provision of HIV and hepatitis C virus testing, and assistance with social services. In 2008, responding to client interest in heroin use disorder treatment and perceived lack of access by clients and program staff, Prevention Point Philadelphia created a buprenorphine maintenance treatment program called the Stabilization, Treatment, and Engagement Program (STEP) that was fully integrated within the SEP. This program targets current SEP participants who express interest in cessation of heroin use.
In 2014, approximately 6,000 clients sought services at Prevention Point Philadelphia, with 5,500 of those utilizing the SEP. This population is characterized by high rates of poly-substance use, psychiatric illness, unstable housing, incarceration, and HIV and hepatitis C infection. While guidelines suggest many such individuals may not be appropriate for office-based buprenorphine treatment,10 previous research has found comparable treatment outcomes among those who use cocaine,11 take other psychoactive medications,12 lack permanent housing,13 or have been previously incarcerated,14-16 as compared to control populations. The aim of the current study is to describe STEP's model of care and report treatment outcomes over an approximately 3 year period (October 2011 to August 2014).
Methods
The STEP model
The goal of STEP is to provide buprenorphine maintenance treatment to SEP clients interested in cessation of heroin use. STEP's medical director is a volunteer attending physician with a Drug Addiction Treatment Act of 2000 waiver to prescribe buprenorphine and care is provided under the auspices of his clinical license; no additional local, state, or federal licenses were required. One SEP case manager serves as the clinic coordinator, overseeing the logistics of STEP. Other SEP case managers provide education and counseling to SEP clients interested in STEP as well as to those patients enrolled in STEP. STEP visits take place in three clinical rooms at the SEP, one day per week. At visits, the medical director supervises rotating medical students and post-graduate trainees from area schools (3-4 each week) who collect clinical histories, conduct point-of-care urine toxicology screening, and provide education and counseling. Given funding and personnel constraints, all STEP patients are linked to nearby community agencies for additional counseling and other necessary behavioral health care.
Assessment of eligibility
To qualify for enrollment in STEP, patients must meet the following criteria: 1) a history of participation in Prevention Point Philadelphia's SEP or social services program; 2) enrollment in a health insurance program (typically Medicaid or Medicare); 3) possession of a state-issued photo ID; and 4) willing to participate in case management as well as attend all scheduled STEP appointments and regular appointments with a behavioral health care provider. Patients are not eligible for STEP if they are unable to comprehend or consent to treatment, have chronic mental illness and are not in ongoing psychiatric care, have acute mental health issues (e.g., suicidal ideation), or have painful conditions requiring opioid analgesics. Patients who use alcohol or other drugs infrequently remain eligible. Patients receiving methadone maintenance treatment with doses greater than 60 mg per day are excluded. Given patient limits due to federal regulations, there is typically a waiting list of 150 to 200 patients at any given time. The clinic coordinator manages this list and works with the medical director to identify priority patients such as those with special needs like HIV infection.
Treatment induction
On enrollment in STEP, SEP case managers provide patients a 1.5 hour mandatory orientation that covers basic information on buprenorphine/naloxone (e.g. mechanism of action, side effects, drug interactions), the requirements and expectations for the program, and individualized answers to patients’ questions. In addition, patients sign a treatment agreement outlining patient and provider expectations.
At the initial medical appointment the medical director supervises volunteer medical students and post-graduate trainees in collecting demographics, a medical history, and a substance use history including confirmation of a DSM-IV diagnosis of opioid dependence and administration of the Addiction Severity Index questionnaire. Patients then meet with the medical director to verify these data and receive a prescription for a one-week supply of buprenorphine/naloxone and instructions on at-home induction.17-19 The initial buprenorphine/naloxone dose is determined on a case by case basis depending on the daily quantity of heroin a patient is using.
Stabilization and maintenance treatment
Patients are seen weekly for the first 4 weeks and then extended to 2, 3 and finally 4 week appointments depending on self-reported drug use and unsupervised urine toxicology screen results, which are obtained at each visit by volunteer medical students and post-graduate trainees. During the first 1–3 months, all patients are titrated to a maximum maintenance dose of 16 mg because of concerns about diversion. Per the treatment agreement, the expectation is that patients stop using heroin within 4 weeks of treatment initiation. Patients still using heroin at the third week are evaluated for intensified treatment needs (e.g., more intensive counseling or transfer to methadone maintenance or a residential treatment facility), evaluated for a dose increase, and given a pre-discharge letter informing them that they will be discharged if heroin use continues the following week. Patients who do not have buprenorphine in their urine toxicology screen, suggesting possible diversion, face potential immediate discharge depending on the circumstances. SEP case managers provide patients with structured referrals to community resources, including behavioral health care.
After patients stabilize on a maintenance dose (typically after 1–3 months), sporadic heroin use is addressed on a case-by-case basis through counseling, intensification of psychosocial treatment, a buprenorphine dose increase (to a maximum of 16mg daily), or a combination of those interventions. If heroin use continues despite intensification of treatment, patients may be subject to administrative discharge for failure to progress toward treatment goals, depending on individual circumstances. Ongoing patient participation in behavioral health treatment is verified through written documentation from outside providers. In all cases, treatment is tailored by providers to be respectful of individual needs and circumstances and to maximize the potential for success in the program.
Evaluation and outcome measures
We conducted a retrospective evaluation of treatment outcomes among all patients who enrolled in STEP between October 2011 and August 2014. Our main outcome measures were time retained in treatment, buprenorphine use, and opiate use.
Time retained in treatment. Our primary outcome was time retained in treatment, defined as time from treatment initiation to treatment failure. Similar to a previous study of buprenorphine maintenance treatment outcomes,13 we defined treatment failure as unplanned self-discharge from the program (i.e., no active prescription and failure to attend scheduled appointments for 60 days20), discharge from the program for failure to progress toward treatment goals despite increasing buprenorphine dosage and intensified behavioral health intervention, discharge from the program for suspected diversion, or drug overdose death. Patients leaving the program because of incarceration, planned transfer to another program (e.g., methadone maintenance or residential treatment), or death unrelated to buprenorphine or drug use were not considered treatment failures.
Buprenorphine and opiate use. Our secondary outcomes were buprenorphine and opiate use, defined as a urine toxicology screen positive for buprenorphine or opiates, respectively. For each patient in each month of treatment, the patient was classified as buprenorphine positive if all urine toxicology screens were positive for buprenorphine and opiate positive if any urine toxicology screen was positive for opiates.
Statistical analysis
First, we examined patient characteristics using descriptive statistics. For a given characteristic, we excluded patients missing data on that characteristic. Next, we analyzed time retained in treatment by constructing Kaplan-Meier survival estimates. We censored patients not experiencing treatment failure (i.e., incarceration, planned transfer to another program, or death unrelated to buprenorphine or drug use) on the date that the outcome occurred. We censored patients still in treatment at the end of the study period on the last day of the study period. We calculated the percentage of patients retained in treatment at 3, 6, 9, and 12 months. Finally, we analyzed opiate and buprenorphine screen results by calculating the proportion of patients who were positive for buprenorphine and opiates in each month of treatment; we then graphed this proportion. This research was approved by our affiliated Institutional Review Board.
Results
Baseline sociodemographic characteristics among patients initiating buprenorphine maintenance treatment at Prevention Point Philadelphia, a syringe exchange program (n = 124) a
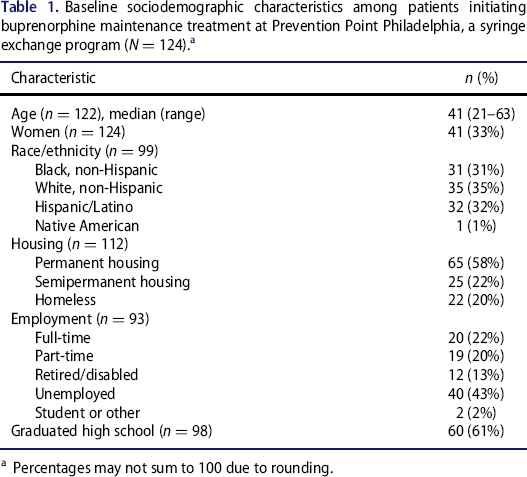
Percentages may not sum to 100 due to rounding.
Baseline substance use, medical, and psychiatric characteristics among patients initiating buprenorphine maintenance treatment at Prevention Point Philadelphia, a syringe exchange program (N = 124)
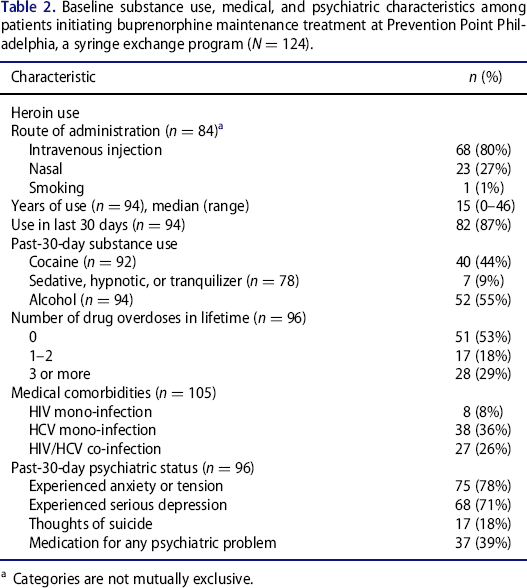
Categories are not mutually exclusive.
Program outcomes among patients in buprenorphine maintenance treatment at Prevention Point Philadelphia, a syringe exchange program (n = 124)
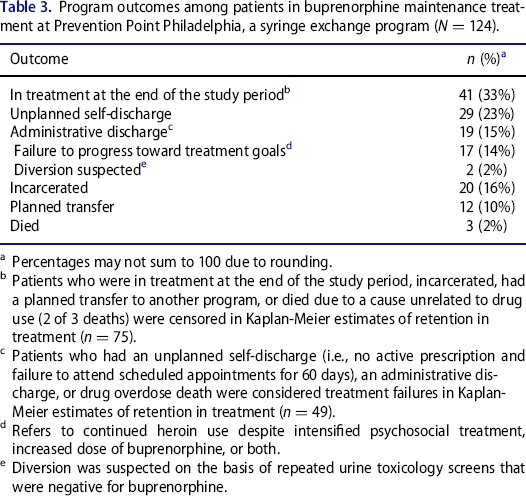
Percentages may not sum to 100 due to rounding.
Patients who were in treatment at the end of the study period, incarcerated, had a planned transfer to another program, or died due to a cause unrelated to drug use (2 of 3 deaths) were censored in Kaplan-Meier estimates of retention in treatment (n = 75).
Patients who had an unplanned self-discharge (i.e., no active prescription and failure to attend scheduled appointments for 60 days), an administrative discharge, or drug overdose death were considered treatment failures in Kaplan-Meier estimates of retention in treatment (n = 49).
Refers to continued heroin use despite intensified psychosocial treatment, increased dose of buprenorphine, or both.
Diversion was suspected on the basis of repeated urine toxicology screens that were negative for buprenorphine.
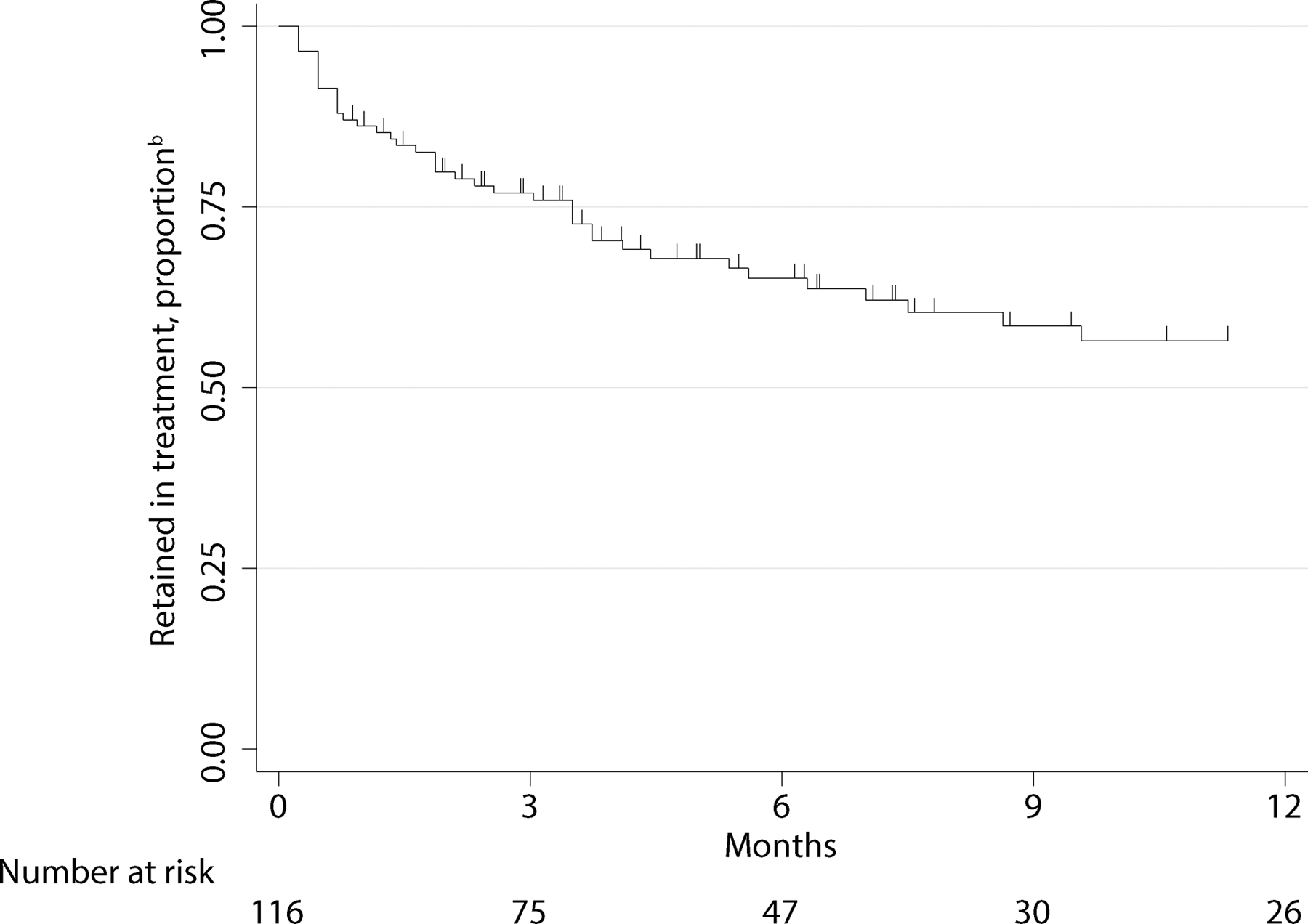
Time retained in buprenorphine maintenance treatment at Prevention Point Philadelphia, a syringe exchange program (n = 124)
At the initial visit prior to induction, 36% (n = 35/96) of patients had a positive buprenorphine screen and 88% (n = 84/96) had a positive opiate screen (Figure 2). Among patients in treatment, the percentage with a positive buprenorphine screen at 3, 6, 9, and 12 months was 88% (n = 50/57), 100% (n = 31/31), 96% (n = 23/24), and 95% (n = 18/19), respectively. The percentage of patients in treatment with a positive opiate screen at 3, 6, 9, and 12 months was 19% (n = 11/57), 13% (n = 4/31), 17% (n = 4/24), and 16% (n = 3/19), respectively.
Urine toxicology screen results over time among patients in buprenorphine maintenance treatment at Prevention Point Philadelphia, a syringe exchange program (n = 124)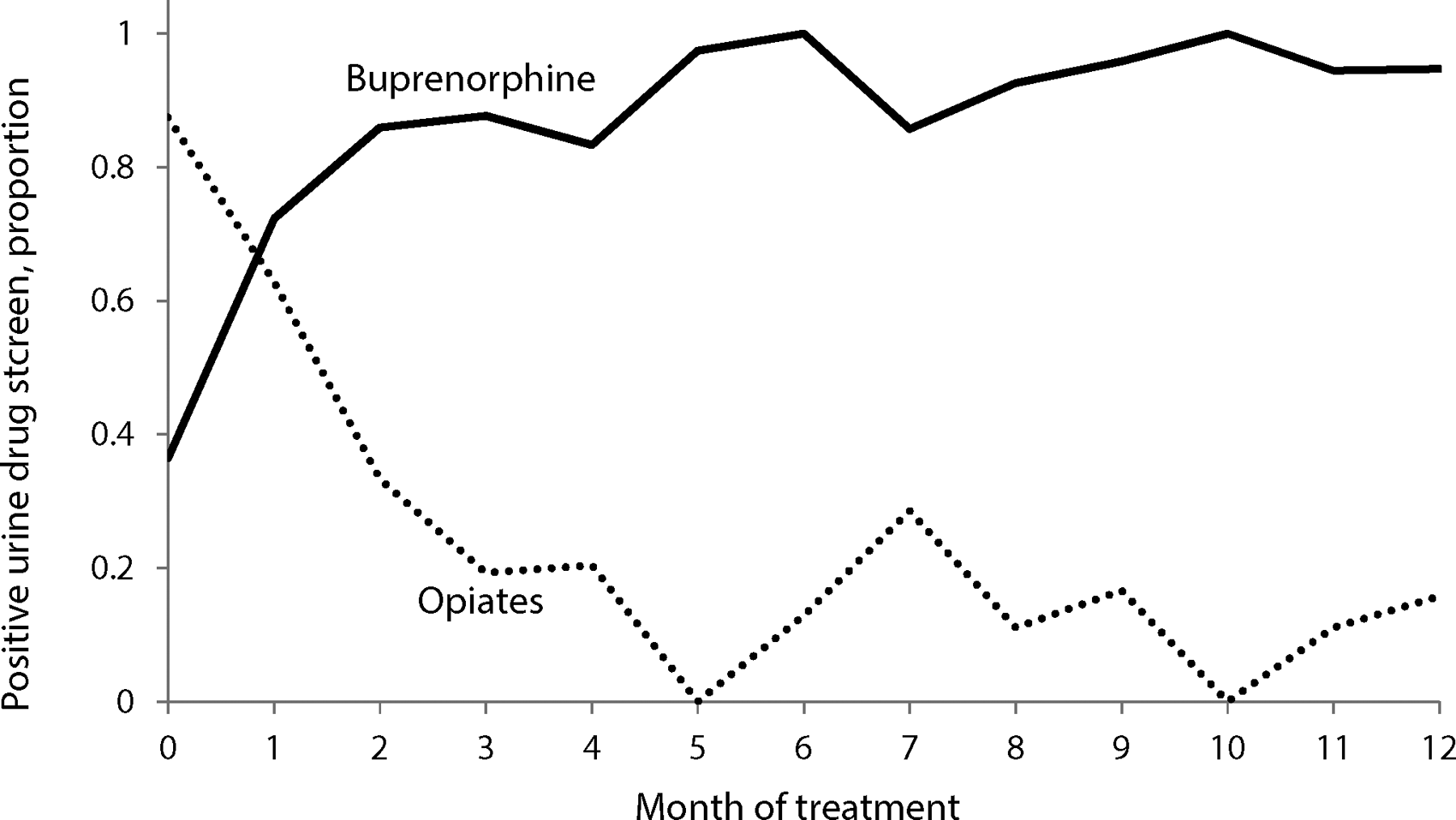
Discussion
Through integration of buprenorphine maintenance treatment alongside harm reduction services, Prevention Point Philadelphia provided treatment to clients interested in cessation of heroin use. The aim of the current report was to describe the STEP model of care and report treatment outcomes. Despite high rates of poly-substance use as well as medical and psychiatric comorbidities, many patients demonstrated sustained retention in treatment and reductions in heroin use. To our knowledge, this is the first report of a buprenorphine maintenance treatment program directly integrated into an SEP.
Among those entering treatment, the percentage of patients retained in treatment at 3-, 6-, and 12-months in the current study (77%, 65%, and 56%, respectively) was comparable to a report of low-threshold buprenorphine treatment in a New York City harm reduction agency (68% at 3 months, 63% at 6 months, and 42% at 12 months).21 However, in contrast to STEP, that program did not require patients to discontinue heroin use or collect urine toxicology screens. While direct comparisons are limited by differences in study populations and methods, retention in treatment in the current study was also comparable to reports from other more traditional settings, such as primary care offices and specialty addiction treatment facilities (45-93% at 3 months, 33–80% at 6 months, and 42–67% at 12 months).11,13,20,22-33 Prevention Point Philadelphia's experience indicates that providing buprenorphine maintenance treatment within SEPs is possible and has the potential to address gaps in access to treatment. While our findings suggest that SEP-based buprenorphine maintenance treatment may provide similar outcomes as other treatment settings, further research is needed to directly compare outcomes within the same population (e.g., a randomized controlled trial)..
Several factors likely explain the retention rate of patients enrolled in STEP at Prevention Point Philadelphia. First, patients often had prior relationships with program staff and were familiar with the organization before entering into treatment. Second, many patients had prior experience with either illicit or prescribed buprenorphine (as indicated by positive urine toxicology screens), which has been associated with improved treatment outcomes in previous research.34,35 Finally, patients in STEP were linked to all other social service programs at Prevention Point Philadelphia in addition to community resources.
Given the novelty of providing buprenorphine maintenance treatment within an SEP, the STEP model of care included mechanisms to prevent diversion. Patients underwent urine toxicology screening to assess for buprenorphine metabolites at every visit and dosages could not exceed 16mg of buprenorphine daily. Patients suspected of diversion were discharged from the program; however, this was infrequent, with only 2 individuals discharged during the study period due to repeated urine toxicology screens negative for buprenorphine. While further research evaluating potential for diversion is needed, our experience is reassuring that risks of diversion can be addressed.
This study has limitations. First, patients enrolled in STEP were, by definition, seeking treatment with buprenorphine for the purpose of stopping heroin use. Therefore, our results may not be generalizable to other types of patients. Further, because of confidentiality, we could not determine the degree to which STEP patients were representative of the greater SEP client population. Second, as data were not collected for research purposes, a substantial proportion of patients were missing one or more variables. The high amount of missing data combined with a modest sample size precluded more complex analyses to identify factors associated with retention in treatment. Third, findings may not generalize to other SEPs located in different areas or serving different clients. Fourth, 16% of patients were incarcerated during the study period; however, specific charges were not known and so we censored these individuals (as opposed to considering this a treatment failure). If incarceration frequently represented a true treatment failure, our estimates of retention in treatment could be biased upward. Future studies in populations with high levels of criminal justice involvement should collect more detailed information on reasons for incarceration to determine if incarceration is related to the current episode of treatment (e.g., drug possession or sales while in treatment) and could be considered a treatment failure or if it is potentially unrelated (e.g., from charges that pre-date the initiation of treatment).
In the setting of increasing heroin use in the United States, SEPs already fulfill a vital role in providing harm reduction services. Through a model of care blending organizational and community resources, Prevention Point Philadelphia expanded to offer critically important treatment services to clients. In this study, treatment outcomes of these complex patients were comparable to reports from other settings. Further research is needed to directly compare SEP-based buprenorphine maintenance treatment to treatment in other settings. If outcomes are similar, efforts to increase treatment capacity should broadly include outreach and engagement with SEPs to support providing onsite treatment to interested clients.
Footnotes
Author contributions
All authors contributed to study concept and design as well as acquisition, analysis, and interpretation of the data. M.A.B. performed the statistical analysis. M.A.B., C.T., and A.P. drafted the manuscript, and all authors provided critical revisions for important intellectual content. D.B. provided study supervision.
Marcus A. Bachhuber received funding support from the Corporal Michael J. Crescenz Veterans Affairs Medical Center and the Robert Wood Johnson Foundation Clinical Scholars Program. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.