
Abstract
Background
The aim of this study was to characterize human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS)-related knowledge and stigma among methadone maintenance treatment (MMT) patients and evaluate the contribution of an educational lecture in reducing risky behavior and unjustified overprotective behavior due to fear and stigma among MMT patients.
Methods
Patients from an MMT clinic within a tertiary medical center were invited to an educational lecture on HIV/AIDS. Seventy participants (of current 330) were chosen by a random sample (December 2015), plus at-risk patients and HIV patients. Attendee compliance and change in scores of questionnaires on knowledge (modified HIV-K-Q-22) and on sexual and injection behaviors were studied.
Results
Forty-six patients (65.7% compliance) attended the lecture, and their knowledge and behavior scores improved 2 weeks post-lecture (knowledge: from 14.2 ± 3 to 19.0 ± 2.2 [P < .0005], sexual behavior: from 12.1 ± 2.9 to 8.8 ± 3.0 [P < .0005], and injection behavior: from 7.3 ± 6.2 to 0.2 ± 1.3 [P < .0005]). The unjustified fear of proximity to HIV carriers reported by 50% attendees fell to 35% post-lecture. Eight months post-lecture, the scores on knowledge and risky behavior of 21 randomly chosen attendees were still better than pre-lecture scores (knowledge: 15.4 ± 2.3 vs. 17.2 ± 1.8 [paired t test, P = .001], sexual behavior: 13.2 ± 2.3 vs. 9.7 ± 2.9 [P < .0005], and injection behavior: 9.3 ± 5.6 vs. 2.8 ± 3.1 [P < .0005]). Drug abuse and treatment adherence were not related to intervention and to risky behavior.
Conclusions
More knowledge, less fear, and less risky behavior immediately and at 8 months post-lecture reflect the success and importance of the educational intervention. Future efforts are needed in order to reduce ignorance and fear associated with HIV/AIDS.
Introduction
Lack of knowledge about the human immunodeficiency virus (HIV) can lead to risky behavior that may bring about infection, fear, and stigma. 1 Methadone maintenance treatment (MMT), the best treatment for opioid addiction, 2 substantially reduces drug injecting, but there is still a risk for HIV infection. 3 Also, MMT patients who are already HIV seropositive may suffer from poor quality of life associated with stigmatization. 4 The Israeli Ministry of Health requires that all MMT patients be tested for HIV antibody on admission and annually thereafter. The levels of knowledge about HIV/acquired immunodeficiency syndrome (HIV/AIDS) and stigmatization of this population have not yet been studied, but it is suspected that the level of knowledge is low whereas that of stigma is high. It was reported that women living with HIV/AIDS experience are being rejected, shunned, and treated differently by physicians, family, and close friends.5
Substance use disorder on its own is an incriminating condition. Individuals with an opioid use disorder who are receiving medication-assisted treatment, particularly, MMT, also suffer from stigma. 6 – 10 Several studies have considered the stigma of MMT as being a major barrier to that approach to treatment of opioid use, not only influencing the person seeking treatment and his/her social environment 6 – 8 but also reflecting the attitudes of professional caregivers as well. 9 ,10
Our aims were to evaluate the extent of knowledge about HIV infection risk and its relation to sexual/injection risky behavior among MMT patients, the compliance of MMT patients in attending a lecture on HIV, the effect of an educational intervention (lecture) on knowledge and risky behavior, and the relation between knowledge and risky behavior and MMT outcomes (substance abuse and treatment adherence).
Methods
The study was approved by the local medical institutional review board.
Study population
Between December 2015 and September 2016, 70 of the current 330 patients in treatment at the Adelson MMT clinic participated in the study. Sample size of 25 per group was needed to achieve power of 80% and alpha value of 5% with effect size of 0.4 according to calculation for 1-way independent analysis of variance (ANOVA).
Characteristics and effectiveness of the clinic have been described in depth elsewhere. 11 , 12 Participants were a nonselective random sample. Forty-eight non-native Hebrew-speaking patients were excluded, and additional participants at risk (n = 16) and seropositive for HIV (n = 6), not randomly sampled, were also included.
Study protocol
After having signed the informed consent, patients were interviewed to fill in the questionnaires (see below), which were again completed by the attendees and nonattendees (persons invited to attend the lecture but who did not attend) for the second time 2 weeks after the lecture. Eight months later, a random half of the attendees were asked to complete the questionnaires for the third time.
Urine tests
Observed and random urine tests, twice per month, for opiates, the cocaine metabolite benzoylecgonine, tetrahydrocannabinol (THC), benzodiazepine, amphetamines, and methadone metabolite were detected using enzyme immunoassay systems (DRI [Thermo Scientific, Canada] and CEDIA [Thermo Scientific, Canada]). 13 Positive urines for each drug at the month prior to pre-lecture questionnaire and 8 months following the lecture questionnaire were taken for analyses.
Questionnaires
The first questionnaire was on HIV/AIDS knowledge, modified and adjusted according to the HIV-K-Q 45-item version 14 and the HIV-K-Q 18-item version.15
Knowledge about HIV/AIDS was measured by a 22-item set of questions covering the subjects of transmission and nontransmission, routes of HIV, and basic knowledge of HIV/AIDS diagnosis and treatment. The participants were asked to respond whether the statement was true or false, and the scores were calculated as the total number of correct answers (range: 0–22).
The second questionnaire was on risky sexual and risky injection behaviors and included 18 questions. The questionnaire was modified from Metzger et al. 16 and is used by the Israel AIDS Task Force for at-risk populations. The section for risky sexual behavior included 7 questions (Table 3) scored on a Likert scale from 0 (no risk) to 18 (highest risk). The section for risky injection behavior included 4 questions (Table 3), with the score ranging from 0 (no risk) to 11 (highest risk). Additional questions on fear and stigma (Table 3) were also included.
Educational intervention lecture
The intervention in the form of a lecture was carried out by a member of the National AIDS Task Force (I.B.). The 1-hour lecture was given in the MMT clinic, in groups of 15 patients each time. It consisted of knowledge on epidemiology, ways of infection and prevention, prevention of HIV infection after exposure, the disease clinical course, antiretroviral therapy for people living with HIV and its impact on the chances of transmitting the virus, prolonging life expectancy in HIV-positive individuals, behaviors that are associated with risk for infections and behaviors that are not involved with risk for infections, risky sexual and injection behaviors, and demonstration of the right use of condoms. The last part of the lecture included questions asked by participants.
Statistical analyses
The chi-square test and Fisher exact test were used for categorical variables, and an analysis of variance (ANOVA) was performed for continuous variables to compare between groups (i.e., attendees vs. nonattendees). Logistic regression was used for multivariate analyses for dichotomic variables (i.e., attendance vs. nonattendance), including significant variables in univariate analyses (P < .05). To evaluate the effect of the intervention, a paired t test and repeated-measures multivariate analyses were used to detect score changes over time and by selected group variables.
Results
Characteristics of the study groups
A total of 70 patients filled in the questionnaires and were invited to attend a lecture. Forty-six patients (65.7% compliance) attended the lecture and filled in the questionnaires again 2 weeks after the lecture. Twenty-four patients did not attend the lecture. The characteristics of those who did and did not attend the lecture are listed in Table 1. The characteristics of the not-invited rest of the patients in the clinic are also described.
Characteristics of attendees, nonattendees, and noninvited groups.
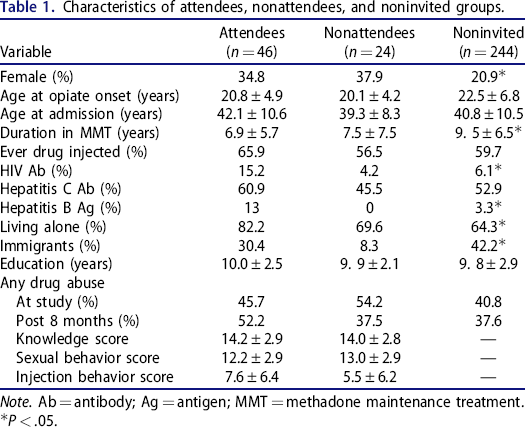
Note. Ab = antibody; Ag = antigen; MMT = methadone maintenance treatment.
P < .05.
The attendees and nonattendees were comparable with respect to age, gender proportion, years of education, duration of opioid usage, and duration in MMT. The only difference was a higher proportion of immigrants among the attendees (P = .04). The attendees and nonattendees did not differ in their pre-lecture knowledge on HIV/AIDS (14.2 ± 2.9 vs. 14.0 ± 2.8, respectively, P = .8), risky sexual behavior (12.2 ± 2.9 vs. 13.0 ± 2.9 respectively, P = .3), and risky injection behavior (7.6 ± 6.4 vs. 5.5 ± 6.2, respectively, P = .2).
The 70 study participants (attendees and nonattendees) had shorter durations in MMT, a higher proportion of HIV-seropositive and hepatitis B–seropositive individuals, a higher proportion of subjects who lived alone, and a lower proportion of immigrants, compared with the 244 nonparticipant patients (Table 1).
Pre-lecture knowledge about HIV/AIDS
The knowledge score of the 70 participants before intervention was 14.1 ± 2.9, reflecting about 64% of correct answers (out of maximum score of 22). It was significantly related to years of education, with the lowest scores among 7 patients with less than 8 years of education (12 ± 1.4), followed by 41 patients with 8–11 years of education (13.8 ± 2.8), and the highest scores among 22 patients with ≥12 years of education (15.5 ± 2.9, P(F = 5.6) = .006). The knowledge score was higher among 8 HIV-seropositive patients compared with the seronegative patients (16.1 ± 3.4 vs. 13.9 ± 2.8, respectively, P(F = 4.4) = .04), and it was not related to gender or age (data not shown). Table 2 lists the responses to 22 true/false statements that reflect knowledge on the various elements of the tested knowledge and the responses of the study participants.
Knowledge questionnaire: level of knowledge and educational efficiency (successfully learned).
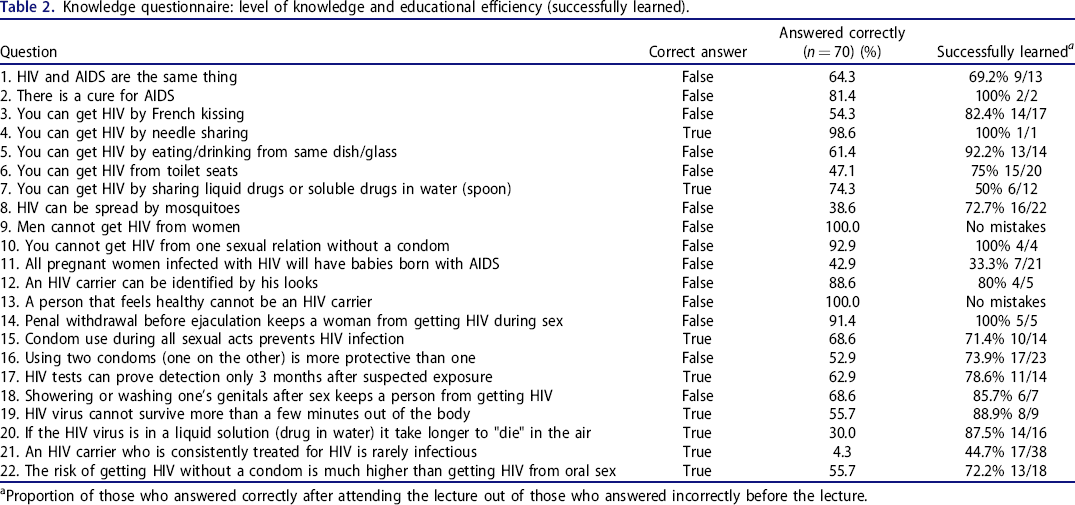
Proportion of those who answered correctly after attending the lecture out of those who answered incorrectly before the lecture.
Table 3 lists the responses to questions on risky behaviors before and after the lecture and on fear and ignorance associated with HIV/AIDS. Fear from HIV infection was reported among 47.1% of the 70 patients, whereas 50% were afraid even of being at a close distance from an HIV carrier. The fear of infection was more prevalent among females (64% vs. 37.8%, P = .04), as was the fear even of being at a close distance from an HIV carrier (76% vs. 35.6%, P = .002). Table 3 also presents distribution of the level of fear. The 35 patients who were afraid of being close to HIV carriers had lower knowledge scores (13.4 ± 2.5 vs. 14.9 ± 3.1, P(F = 4.5)=.04) and higher risky sexual behavior scores (13.2 ± 2.7 vs. 11.7 ± 2.9, P(F = 4.5)=.04), compared with the 35 patients who were not afraid.
Risky behaviors during the previous year.
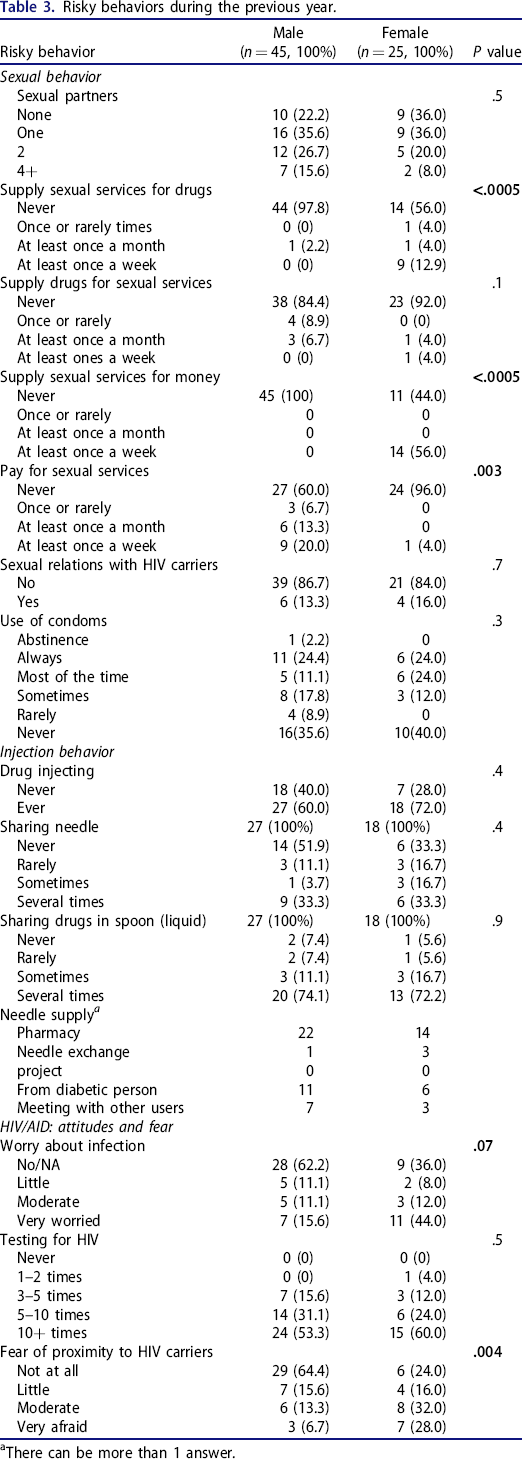
There can be more than 1 answer.
Intervention—Knowledge and risky behaviors
The scores of knowledge and risky behaviors post-lecture improved significantly compared with the pre-lecture scores (knowledge: from 14.2 ± 3 to 19.0 ± 2.2, P < .0005; sexual behavior: from 12.1 ± 2.9 to 8.8 ± 3.0, P < .0005; injection behavior: from 7.3 ± 6.2 to 0.2 ± 1.3, P < .0005) (Table 4). Eight months later, the knowledge scores were still higher than the pre-lecture scores, and the scores for risky behaviors continued to be lower than the pre-lecture scores (Table 4).
Pre- and post-lecture mean scores of the study cohort and of 21 randomly chosen lecture attendees 8 months later.
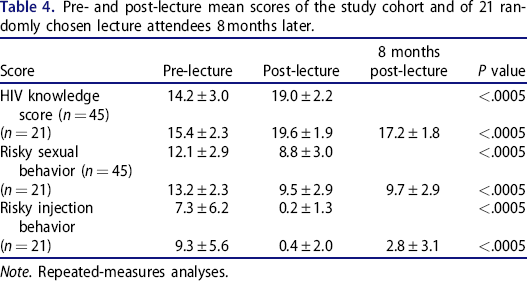
Note. Repeated-measures analyses.
More than 70% of those who answered incorrectly prior to the lecture gave correct answers after the lecture (Table 2). Interestingly, most patients apparently had not learned that all pregnant women infected with HIV will not have babies born with AIDS as long as they are on treatment and/or appropriate measures are taken during delivery.
Twenty-one of the 45 attendees (46.7%) were afraid of being close to an HIV carrier before the lecture, compared with 35.6% who continued to be afraid after the lecture (P < .0005). Level of fear changed significantly post-lecture, with an interaction by gender. Women who were more afraid reduced significantly (Time: F = 9.9, P = .003; Group: F = 10.5, P = .002; Time × Group: F = 3.9, P = .05,). Nineteen patients were afraid of being infected (42.2%) pre-lecture, and 37.8% only post-lecture (P = .03). However, no change was observed with respect to score of being afraid of being infected, still a significant difference by gender (data not shown).
Discussion and conclusions
MMT patients have limited knowledge about HIV/AIDS, including risky behaviors in terms of HIV acquisition and unjustified fear of proximity to HIV/AIDS individuals. Importantly, a single explanatory lecture successfully improved that level of knowledge, reduced fear, and reduced self-reported risky behaviors. These findings continued to be retained 8 months after the lecture had been delivered.
The mean pre-lecture score on knowledge about HIV/AIDS was 14.1 ± 2.9, which was about 64% of the highest achievable score if all 22 questions were correctly answered. A higher knowledge score was associated with more years of education and with being HIV seropositive. No other variable, including gender, were related to pre-intervention level of knowledge, including the compliance to attend the lecture. With respect to risky sexual behavior, the HIV-seropositive patients had a lower behavior score (lower risky behavior than the non-HIV-seropositive), in accordance with their higher knowledge level. Women, however, had higher score of risky sexual behavior than men. Risky behavior related to drug injection was similar between genders, but the score was higher (more risky) among hepatitis C–seropositive patients and with a statistical trend for being higher among HIV-seropositive patients as well. Again, risky sexual behavior was not related to the lecture attendance.
Being afraid of HIV infection was more prevalent among females. A higher proportion of females reported fear of even being close to HIV carriers than males.
Following the lecture, the mean score of knowledge improved significantly, with 86% of the questions being answered correctly. The unjustified fear of HIV was substantially lessened as well. Specifically, the score of being afraid to be in close proximity to HIV carriers that was higher among females was lower for both females and males as well.
As a result of one educational lecture, misconceptions about several common daily activities posing a possible risk to getting infected with HIV among a significant amount of patients (i.e., using a toilet) were rectified. The more important of which are the types of behavior that involve social interrelation, such as eating from the same dish (pose no infection risk); they would most likely change fear and improve quality of life among persons seropositive for HIV.
Finally, 40% of our patients had reported not using a condom before attending the lecture and that figure improved significantly following the lecture.
The results emphasize the importance of even as few as one educational intervention in enhancing knowledge, lessening fear, and reducing risky behaviors in association with HIV/AIDS. Study limitations include the absence of a comparison group, the inclusion of one clinic only, and the short follow-up. Expanding the study to other clinics, having a control group and a longer follow-up, is necessary.
Footnotes
Author contributions
E.P. designed the research and did the analyses, I.B. carried out the intervention, and A.S. collected the data. All authors contributed, edited, and approved the final version of the manuscript.