
Abstract
Background
Provider–patient communication underpins many initiatives aimed at reducing the public health burden associated with prescription drug abuse in the United States. The purpose of this qualitative analysis was to examine the characteristics of provider–patient communication about prescription drug abuse from the perspective of prescribers.
Methods
From 2014 to 2015, 10 semi-structured interviews were conducted with a purposive sample of prescribers from multiple professions and medical fields in Central and South Central Appalachia. The interviews were conducted using a guide informed by Social Cognitive Theory and community theory research, audio-recorded, and transcribed verbatim. Thematic analysis, facilitated by NVivo 10 software, was used to generate themes.
Results
Prescribers described 3 primary communication patterns with patients related to prescription drug abuse—informative, counteractive, and supportive. Prescribers also reported multiple factors—personal (e.g., education, experiences, and feelings of tension) and environmental (e.g., relationship with a patient, clinical resources, and policies on controlled prescription drugs)—that affect provider–patient communication and, by association, delivery of patient care related to prescription drug abuse.
Conclusions
The findings suggest that provider–patient communication about prescription drug abuse is multidimensional and dynamic, characterized by multiple communication patterns and contributory factors. They have implications for (1) research aimed at advancing theoretical understanding of prescriber prescription drug abuse communication behaviors with patients and (2) interventions aimed at strengthening prescriber prescription drug abuse communication behaviors with patients.
Introduction
Prescription drug misuse and abuse are a pressing public health issue in the United States. 1 – 4 In 2016, approximately 6.2 million persons 12 years or older misused prescription drugs in the past month, with approximately 3.3 million persons misusing prescription opioids in particular. 5 Prescription opioid use disorder is among the most common types of substance use disorder related to illicit drug use. 5 , 6 In 2016, approximately 1.8 million persons 12 years or older had a prescription opioid use disorder in the past year. 5 Prescription opioids helped fuel the drug overdose epidemic, 7 contributing to more than 200,000 drug overdose deaths from 1999 to 2017 according to the Centers for Disease Control and Prevention (CDC).8
Multiple initiatives have been put forward in response to the public health burden associated with prescription drug misuse and abuse 1 , 3 , 9 – 11 —hereafter referred to as prescription drug abuse (PDA). They commonly target the clinical knowledge and practices of health care providers, a population optimally positioned to advance PDA prevention, identification, and treatment. Examples of provider-targeted initiatives include (1) increased pain management and substance abuse education; (2) increased use of clinical practice tools (e.g., prescription drug monitoring program [PDMP]); and (3) increased substance abuse screening and treatment services. The emphasis on providers underscores their centrality to an effective public health response.
Interpersonal communication between providers and patients underpins many provider-targeted initiatives for PDA and associated harms. 12 Provider–patient communication accordingly plays a fundamental role in clinical practice. 13 – 15 When effective, provider–patient communication could contribute to positive outcomes for providers (e.g., reduced job-related stress) and patients (e.g., improved satisfaction). 15 – 19 In clinical practice, however, communication problems can be common. 17 , 20 Ineffective provider–patient communication is concerning, as it could contribute to negative outcomes for providers (e.g., malpractice claims) and patients (e.g., missed chances to enhance self-management). 16 , 18 Effective, situational communication about PDA between providers and patients could thus be critical to maximizing the public health impact of provider-targeted initiatives. PDA communication is especially salient to prescribers, referring herein to providers licensed to prescribe controlled prescription drugs (CPDs). Prescribers are among the gatekeepers of CPDs. 21 Evidence suggests that a sizable proportion of providers—physicians and pharmacists—consider physicians to hold the primary responsibility for preventing PDA and addiction. 22 Similarly, provider-targeted initiatives frequently impact or necessitate action from physicians. 23 Multiple provider-targeted initiatives, for example, aim to improve prescribing practices, often for opioids. The National Institute on Drug Abuse further indicated that prescribers—specifically physicians—are in a “unique position” to recognize PDA and prevent progression to a substance use disorder. 24 For example, they have the potential to facilitate recognition of a problem, access to treatment, and formation of recovery goals among patients. 24 Communication between prescribers and patients is integral to all of these clinical practices.
Succinctly, provider–patient communication about PDA remains understudied relative to its underlying role in mitigating PDA and associated harms in the context of health care encounters. Prior research suggests providers, including prescribers, agree that PDA communication with patients is important and, if improved, could deter PDA. 12 , 25 A comprehensive report on CPD diversion and abuse, however, suggests many physicians do not inquire about PDA when taking the health history of patients and find it hard to discuss PDA with patients. 22 A study of prescribers and pharmacists similarly found PDA communication to be “uncomfortable, variable, multifactorial, and often avoided.” 12 While qualitative research methods could advance understanding of the characteristics of provider–patient communication about PDA, few studies have used them, 12 and fewer, if any, have focused exclusively on prescribers. Hence, this qualitative analysis examined the characteristics of provider–patient communication about PDA using data collected through interviews with prescribers. The findings could inform prescriber-targeted interventions to strengthen provider–patient communication about PDA and, ultimately, prescriber capacity to mitigate PDA and associated harms.
Methods
Study design and sample
This study employed a qualitative design involving semi-structured interviews with prescribers. Prescribers of CPDs practicing in a clinic affiliated with, or practicing within the service area of, the Appalachian Research Network (AppNET)—a rural, primary care practice–based research network in Central and South Central Appalachia—were eligible. The AppNET infrastructure supported efficient connection to and recruitment of prescribers. The scope of services delivered by AppNET-affiliated clinics, coupled with their rural locale, were presumed to be representative of many clinics in the region.
Purposive sampling was predominantly used to identify and recruit prescribers. Snowball sampling was incorporated after an enrolled prescriber recommended another prescriber for participation. Study staff selected prescribers for (1) understanding of the PDA problem or clinic proximity to counties where PDA is prevalent and (2) willingness to discuss the subject. Recruitment entailed an e-mail invitation followed by a telephone call to prescribers interested in participating. The sample (n = 10) included 3 female and 7 male prescribers from multiple professions (i.e., dentistry, medicine, and nursing) and medical fields (e.g., addiction and family medicine). Of relevance to the sample size, prescribers were sampled as part of a mixed-methods study focused largely on the patient perspective. A primary goal was to collect data to inform the development of a theory-based survey instrument to explain patient engagement in situational PDA communication with providers. Data saturation was reached on concepts related to the survey instrument.
Data collection
From May 2014 to April 2015, 10 semi-structured interviews were conducted using a guide. The guide was grounded in Social Cognitive Theory (SCT) 26 and communication theory research, 27 internally reviewed and refined, and pilot tested with several prescribers prior to use. Prescriber perceptions, behaviors, and experiences regarding PDA communication with patients, along with general perceptions of PDA, were explored. Specific to the development of the patient-targeted survey instrument, prescriber perceptions of 4 survey instruments—3 validated 28 – 30 and 1 researcher-developed—were explored. One male researcher with interviewing experience and PDA expertise conducted the interviews in a private setting selected by the prescriber, often the clinic where he or she practiced. Another researcher or research assistant took field notes. The interviews were audio-recorded and transcribed verbatim. The transcripts were de-identified and imported into QSR International's NVivo 10 software.31
Data analysis
Inductive thematic analysis was used to generate themes. 32 , 33 The researchers, most of whom had experience in qualitative research, engaged in an iterative process of independent transcript review and open dialog to generate preliminary codes. One researcher refined and finalized the codes to include defining and organizing the codes into a coding frame. An initial subset of transcripts (n = 2) was randomly selected and independently coded by two researchers to evaluate coding consistency and coding frame reliability. 34 Consensus-based discussion was used to resolve coding inconsistencies and modify the coding frame for improved reliability. The remaining transcripts were coded by the two researchers thereafter. One researcher compared and combined codes to generate themes to include a repetitive process whereby the themes were assessed in relation to the coded data and complete data set. 32 , 33 The same researcher defined and named the themes and selected representative quotes. 32 ,33
Ethical considerations
The Institutional Review Board at East Tennessee State University reviewed and approved this study. One researcher explained the study and attained written informed consent before interviews. Prescribers received modest compensation ($50).
Results
Two themes and 9 subthemes were identified (Figure 1). Specifically, theme 1—factors affecting prescriber communication with and care of patients—included 6 subthemes, and theme 2—prescriber communication patterns with patients—included 3 subthemes.
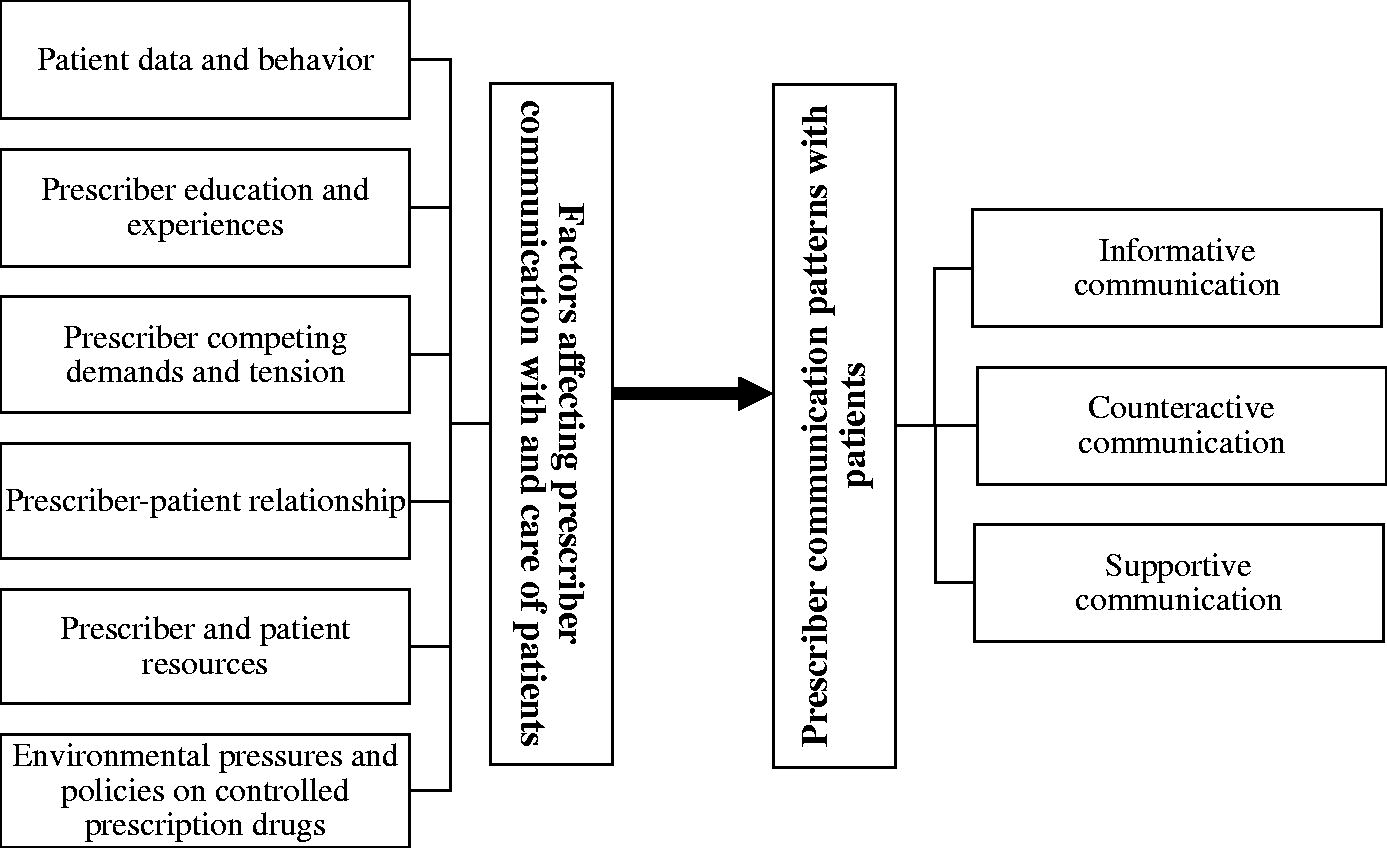
Thematic map of the themes and subthemes identified in provider–patient communication about prescription drug abuse from the prescriber perspective.
Theme 1: Factors affecting prescriber communication with and care of patients
Prescribers described multiple factors that affect patient communication and care. They focused on not only PDA and addiction but also the intersection of PDA with pain evaluation and treatment, particularly prescribing CPDs. Six subthemes were generated, with representative quotes presented in Table 1.
Representative quotes for theme 1: Factors affecting prescriber communication with and care of patients.
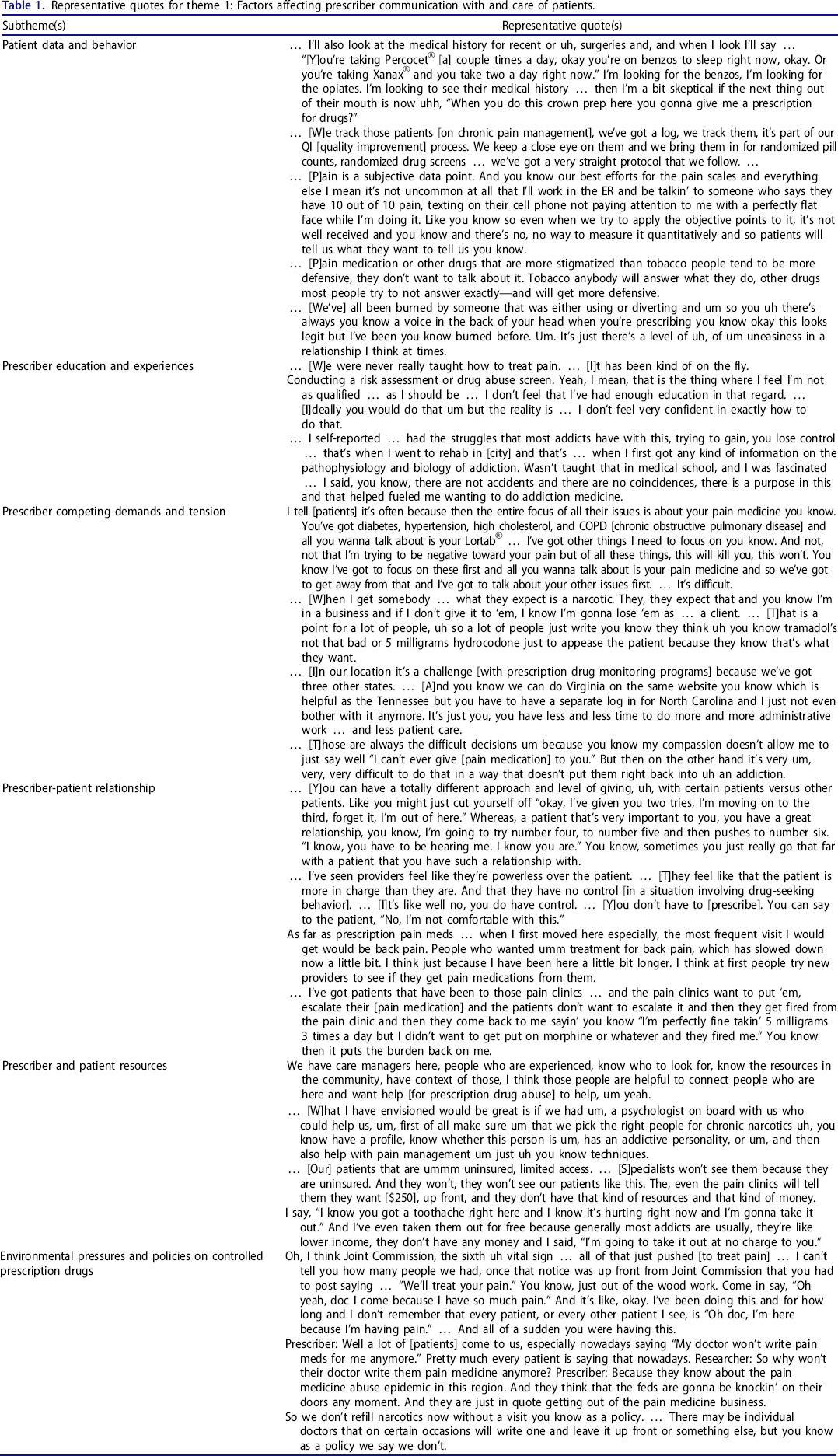
Patient data and behavior
Most prescribers identified patient data as a significant factor, including data from direct and self-reported measures. They indicated that data may not only influence and, at times, initiate patient communication and care related to PDA and addiction but also influence CPD prescribing. Many prescribers described “red flags” considered indicative of PDA, addiction, or related problems. Among these were “failed” urine drug screens and pill counts; PDMP query results; patient inquiries into and requests for CPD prescriptions; and patient self-reported drug abuse, addiction, and unintentional diversion (e.g., “medications being stolen”). In addition to the influence of data, multiple prescribers reported the collection of data through patient monitoring, especially patients on CPDs. Terms such as “monitor” and “police” were used.
Concerning patient behavior, many prescribers described the role of possible deception among patients. They indicated that patients can not only be “deceiving” and “pretending and hiding” drug abuse, but will also “manipulate” and “try to trick” prescribers for CPD prescriptions. Some prescribers suggested connections between deceptive patient behaviors and challenges in pain evaluation and treatment, including an inability to “measure [pain] quantitatively” and having to “trust” that patients are in pain. Moreover, several prescribers described deceptive patient behaviors as possible barriers to communication. For example, one prescriber expressed doubt that “people are really willin’ to be honest” about drug abuse histories. Several prescribers further indicated incidents in clinical practice involving deceptive patient behaviors that could have residual effects, such as apprehension about the legitimacy of patient problems and “lower confidence” in patient communication.
Prescriber education and experiences
Most prescribers identified education and training as factors in patient communication and care related to PDA and addiction. Multiple prescribers reported limited or inadequate education and training on addiction or pain, including in medical school and residency. A few prescribers similarly described the impact of education and training, including not “enough education,” on specific clinical practices (e.g., screening). Moreover, some prescribers described the impact of time since education or training completion. Challenges associated with “first start[ing]” and the “different mindset” of an “older practitioner” and a “newer practitioner,” for example, were noted.
Similarly, several prescribers described the influence of personal and familial experiences on patient care related to addiction and pain. A prescriber reporting personal experience with addiction, for example, suggested that it prompted the attainment of addiction information and specialization in addiction medicine. Likewise, a prescriber reporting familial experience with addiction suggested that it limited the strength and dosage of CPDs prescribed for pain.
Prescriber competing demands and tension
Many prescribers described competing demands—multiple “demand[s]” on their “time”—as a factor. They generally posited that competing demands can limit patient communication and care related to PDA and addiction. Multiple prescribers specifically described the role of competing demands in face-to-face patient interactions, including “a ton of other things to talk about” and contrasting priority health issues or treatment goals/preferences between prescribers and patients. Treatment goals/preferences were conveyed as particularly impactful. Multiple prescribers indicated that patients “expect” and “want pain medications” and may resist “taking them away.” They suggested that not fulfilling or aligning with patient treatment preferences/goals (e.g., refusing to prescribe CPDs, prescribing CPDs at dosages that do not satisfy perceived needs, or discussing drug abuse histories) could contribute to the realization of negative or unwanted outcome expectations (e.g., monetary repercussions). Although less common, several prescribers reported competing demands outside of patient interactions, including administrative and other “time-consuming” tasks.
Relatedly, many prescribers reported experiencing tension related to CPD prescribing, primarily “narcotics.” They described difficulties and “internal battle[s]” inherent in deciding to prescribe CPDs and feelings of discomfort and concern for patients on CPDs, especially “higher doses.” Further, some prescribers mentioned tension related to the realization of negative outcome expectations by prescribing CPDs, including patient addiction and overdose.
Prescriber–patient relationship
Many prescribers described characteristics of the prescriber–patient relationship as a factor. First, some prescribers indicated the influence of the relationship quality and “dynamic” on patient communication and care related to PDA and addiction. Multiple relationship elements were mentioned, including knowledge, trust, and the balance of power between prescribers and patients. Second, some prescribers mentioned the relationship length, especially its influence on patient communication and care related to CPDs. For example, the “initial visit” and receipt of patients formerly “under the care of other providers” were noted as conditions that may increase the likelihood of prescribing. Last, some prescribers described, at times with frustration, the influence of cyclic relationships with chronic pain patients, particularly on CPD prescribing. They reported referring patients to specialty care for pain management, or “pain clinics,” only for patients to “come back,” often because they were “stable,” “discharged,” or “fired.”
Prescriber and patient resources
Many prescribers identified “resources” as a factor, including prescriber and patient resources. Specific to prescriber resources, they described both available clinical resources and clinical resources that if available could facilitate patient communication and care related to PDA and pain. Risk assessment and communication tools, “ancillary staff,” and mental health professionals (e.g., “psychologist”) were among those noted. Similarly, some prescribers reported the influence of deficits in patient resources, including “money,” health insurance, and social support. They often described such deficits as barriers to patient communication and care (e.g., referring patients to specialty care). Concurrently, several prescribers reported actions taken to compensate for patient deficits and facilitate patient care (e.g., “free” services).
Environmental pressures and policies on CPDs
Multiple prescribers described the influence of “external pressures” or “voices” as a factor. Several prescribers mentioned pressures to “treat pain,” including those from health care accreditation organizations and accrediting patient experience surveys. They suggested that such pressures influenced CPD prescribing and amplified patient treatment seeking and expectations for pain relief. Moreover, some prescribers reported pressures informing and regulating CPD prescribing, such as clinical guidelines, state laws, and state/federal actions. Several prescribers indicated that such pressures have contributed to prescribing reductions, while others indicated they could “make it harder and more stressful” and contribute to prescribers “getting out of the pain medicine business.”
Consistent with pressures, some prescribers highlighted the role of clinic policies. As one explained, “I think there's external pressures on doctors. … We in turn are applying that pressure to all of our patient populations as well.” Prescribers mentioned multiple policies, many standardizing CPD prescribing. They suggested that policies influenced CPD prescribing and, at times, informed patient communication related to PDA and pain. Policies establishing processes for new prescriptions (e.g., requiring a “contract”) and prescription refills (e.g., no “early refill”) and prohibiting CPD prescribing (e.g., “strict no narcotic policy”) were among those noted.
Theme 2: Prescriber communication patterns with patients
Prescribers described multiple communication patterns with patients related to PDA, generating three subthemes.
Informative communication
Most prescribers reported informative communication, a pattern that provided PDA-related information, instructions, or explanations to patients. They commonly conveyed it as one-way communication in the context of prescribing CPDs for the treatment of pain and, to a lesser extent, addiction. Some prescribers reported informing patients of the abuse potential of CPDs or instructing patients on the “proper way to take” CPDs. One stated, “… I discuss the side effects and possibility of … addiction.” Another said, “… ‘[D]on't take any other medicines or alcohol or drive or operate any machinery,’ that's what I say. … ” Likewise, some prescribers mentioned informing patients of treatment plan components, including stipulations for CPD prescriptions. Several specifically reported providing a “contract,” while another recalling a previous patient situation explained: … I went through everything on that [researcher-developed instrument] practically about why we shouldn't be going here … I finally just said, “Fine, this is what you're getting.” … Signed the prescription … I made my goals clear, cut off clear, and that was the end of that.
Conversely, many prescribers described informative communication in the context of refusing to prescribe CPDs, especially “narcotics.” Prescribers reported multiple explanations used to justify a refusal, including patient history of addiction, clinic policies, and state laws. One said, “… I really use … the state laws now because I tell people that I'm not gonna be a pain clinic so I'm not going to be writing prescriptions.” Likewise, several prescribers mentioned clinic signs informing patients of “no narcotic” policies, with one stating, “… [T]hey have signs saying they don't prescribe.”
Counteractive communication
Many prescribers described counteractive communication, a pattern that involved “address[ing]” PDA-related “problems” with patients. Problems included PDA, addiction, and other behaviors (e.g., diversion). Prescribers frequently framed it as reactive communication in the context of problems that were suspected or verified, whether by observation or “data.” One stated: Again it's typically initiated by … some trigger that has led me to think that they have an issue with [PDA]. Whether that's requesting prescriptions early … a pharmacy calling me to tell me that you know they're getting from multiple pharmacies … the controlled substance database … when I do feel like there's an issue then I certainly will address it.
Another said, “Um discussing the results of prescription drug monitoring program query … yeah I have … when I actually found something.” When addressing problems, some prescribers described two-way communication that entailed seeking information from patients. Referring to telephone calls by persons alleging a patient of PDA, one explained, “… [I] confront the patient and say, ‘Hey, you know I'm getting some phone calls. Here's what they're telling me. Tell me why I shouldn't believe this. … ’” Several prescribers, however, reported a more austere approach—dismissal. One stated, “… [W]hen they do fail their drug screen and you know that they've brought in urine. … We're done with them.”
While more commonly described as a response, some prescribers reported counteractive communication that may preempt problems. One said, “And in fact we tell them if you go to the ER, then you'll be kicked outta here.” Apart from clinical repercussions, several prescribers noted warning patients through oral or written communication of legal repercussions, especially for diversion. One explained, “I had to get a letter from the sheriff and post it in every exam room saying that … you will be prosecuted if you are found selling or distributing.”
Supportive communication
Some prescribers reported supportive communication, a pattern that supplied various types of social support (e.g., informational and instrumental) to patients. It was commonly described in the context of concerns and treatment needs related to PDA, addiction, and pain, including those expressed by patients. One prescriber said: And I get patients that say, “I'm addicted.” And I will say, “Why do you say you're addicted?” And they will say, “Well ‘cause I missed a dose and god I felt terrible. … I took a dose and then I was okay.” And I have to explain to them that's dependence. … And they feel better about themselves.
Another stated: … [W]hat I tell a patient, “if you've been doing great and … your brother-in-law … had this Roxicet®, and you took it … for me personally, that's not a relapse … that's a bad damn decision” … [I]f I immediately go, “you've relapsed.” It's going to be like … “what's the use, I'm back to square one.” I go look, “you're not under a bridge with a needle in your arm.” … That was a bad decision. … So, let's learn from those. …”
Several prescribers reported supportive communication specific to facilitating treatment seeking or receipt, including specialty care for chronic pain and addiction. One explained: … I'll say, “look, man … you might have … some drug issues … But if I can help you, I'm on your team and I want to help you. So what I'm going to do is I'm going to tell you where to go to a Suboxone® clinic where they have counselors.” … and I give them one of these pamphlets … where the AA and the NA meetings are in [city].
Discussion
This qualitative analysis examined provider–patient communication about PDA from the prescriber perspective. Prescribers reported different communication patterns with patients and multi-level factors that affect communication with and care of patients. By advancing knowledge of these patterns and factors, the findings can inform prescriber-targeted interventions to improve provider–patient communication about PDA.
Three communication patterns with patients were identified. First, prescribers reported informative communication, characterized by giving PDA-related information, instructions, or explanations to patients. Although most reported at least one form of informative communication, prescribers generally did not report communication behaviors to verify patient understanding. Patient understanding could be associated with patient recall. 35 , 36 Given such an association, the findings align with prior research that suggests that patient recall of verbal counseling from providers when receiving a new prescription for an opioid-acetaminophen drug, including topics pertinent to averting harm, is often limited. 37 Information verifying behaviors, however, could be “critical to many aspects of clinical care.” 38 Patient understanding could likewise be a prerequisite for patients to take steps and make decisions concerning their health. 39 Taken together, the findings point to a potentially significant, yet modifiable gap in provider–patient communication about PDA. Prescriber use of effective methods (e.g., teach-back 40 – 42 ) to verify patient understanding in the context of PDA-related communication, for example, could be beneficial.
Second, prescribers reported counteractive communication, characterized by addressing PDA and related problems with patients. Although a common purpose, they described different approaches. One dimension on which the approaches differed was the extent to which they were patient-centered. According to the Institute of Medicine, patient-centered care is characterized by “providing care that is respectful of and responsive to individual patient preferences, needs, and values and ensuring that patient values guide all clinical decisions.” 43 It involves patients in care and individualizes care to patients. 44 , 45 Communication is important in patient-centered care 43 , 44 , 46 ; patient-centered communication is likewise recognized as a “central component of high-quality health care.” 47 Prescribers described some approaches that aligned more closely with patient-centered communication and care (e.g., seeking information from patients), while others aligned far less (e.g., patient dismissal). By extension, the approaches underscore opportunities—often missed—for PDA identification and treatment. Given the current unmet need for substance use treatment 5 , 48 and drug overdose epidemic in the nation, 7 the potential for even one missed opportunity to address PDA, and substance abuse in general, is concerning.
Last, prescribers reported supportive communication, characterized by supplying social support to patients. Despite its potential positive implications, supportive communication was less commonly reported than informative and counteractive communication. The distribution suggests that prescriber communication behaviors related to PDA could have a stronger tendency to be characterized by a more prescriber-directed, biomedical style relative to a more patient-centered, psychosocial style. Although this finding aligns with prior research on communication patterns in the primary care setting, 49 it remains noteworthy. Patient-centered care, for example, has become of interest to multiple stakeholders (e.g., health care organizations). 45 – 47 Evidence suggests that it could contribute to positive patient outcomes 44 , 45 , 50 and that patients frequently prefer a patient-centered communication style. 51 , 52 Patient preferences in communication, though, have been posited as a potential intermediary between physician style and patient outcomes. 51 Future research could therefore explore the degree of concordance between provider styles and patient preferences specific to PDA communication.
Similar to communication patterns, previous qualitative research identified approaches for PDA communication with patients among prescribers and pharmacists. 12 Along with approaches describing behavioral engagement in PDA communication, an approach describing non-engagement was identified—“communication avoidance.” 12 Although not distinct patterns, findings within informative and counteractive communication are consistent with avoidance of and withdrawal from communication. 27 Posting clinic signs and providing patient contracts, for example, could indicate avoidance of communication. Written communication could thus be a means of avoiding oral communication related to PDA with patients. Alternatively, patient dismissal and refusal to prescribe CPDs, for example, could reflect partial withdrawal from communication. 27 In other words, prescribers could be only communicating as much as needed to minimize further interactions with patients. 27 Avoidance of and withdrawal from communication denote a decrease in willingness to communicate; communication apprehension and self-perceived communication competence are antecedents of willingness to communicate. 27 Such relationships suggest that the findings are consistent with previous qualitative research 12 and the communication theory research 27 that partially guided interviews.
Prescribers identified an array of factors that affect provider–patient communication and, by association, delivery of patient care related to PDA. Multiple factors paralleled, at least in part, the “influencers” of PDA communication and prescribing/dispensing behaviors found in prior qualitative research. 12 For example, the factor patient data is similar to the influencer “subjective vs. objective patient information,” prescriber education to “level of [healthcare professional] training and experience,” and prescriber–patient relationship to “patient relationships.” 12 The parallels underscore that provider–patient communication about PDA is a dynamic process and provide a solid basis from which future research can draw to better quantify its contributing factors. When considered as a whole, a commonality across the factors was the intersection of PDA with pain evaluation and treatment. Although notable, this is not surprising. Opioid prescribing and sales, particularly for chronic non-cancer pain, increased substantially in recent decades, concomitant with opioid-related harms. 53 – 56 Prescribers could be a direct, or indirect, source of prescription opioids for misuse. 57 , 58 Individuals often report physical pain relief as a reason for misuse, 59 and a notable proportion of patients receiving opioids for chronic pain have been estimated to misuse them. 60 , 61 The connection between aspects of pain care (e.g., lack of an objective measure) and prescriber difficulty, discomfort, and even frustration at times in PDA-related patient interactions emphasized the intersection of the two conditions. The CDC Guideline for Prescribing Opioids for Chronic Pain likewise describes chronic pain prevention, assessment, and treatment as “challenges.” 62 Moreover, “improv[ing] communication between clinicians and patients about the risks and benefits of opioid therapy for chronic pain” is among the intended purposes of the guideline. 62 In short, the findings substantiate both the need for the guideline and its potential utility in PDA-related patient interactions.
Interestingly, the factors identified by prescribers represent personal and environmental factors, illustrating the perceived role of factors at different levels of influence. Education, experiences, and tension, for example, represent personal factors. Conversely, prescriber–patient relationship, prescriber and patient resources, and pressures and policies on CPDs, for example, represent social and physical environmental factors. Multi-level influence is consistent with SCT, 26 a theory that partially guided interviews. Specifically, it is consistent with reciprocal triadic causation, describing the interplay among behavior, personal factors, and environmental factors. 63 , 64 Additional findings within the factors identified align with SCT constructs. For example, low self-efficacy, or “confidence,” in patient communication was connected to insufficient education and experiences with patient deception, whereas negative or unwanted outcome expectations were connected to competing demands and tension. While these findings may not substantiate SCT in totality (i.e., all constructs), they provide support for its utility in understanding prescriber PDA communication behaviors and a theory-based direction for future research.
Evidence suggests that interventions could improve physician communication behaviors during patient interactions. 38 The findings of this qualitative analysis could inform prescriber-targeted interventions specific to PDA communication. Patient-centered communication can be conceptualized as a trait (i.e., “overall style of practice”) and a state (i.e., “behaviors during a particular interaction”). 47 Hence, interventions aimed at increasing state-like patient-centered communication behaviors during PDA-related patient interactions could be beneficial. A focus on patient-centered communication behaviors is supported by both the growing interest in patient-centered care and its relevance to PDA and the findings. For example, patient-centered communication aims to “build trust and understanding between physicians and patients,” 46 a relevant characteristic considering that the prescriber–patient relationship was found to be an influential factor. Patients could also be more inclined to discuss sensitive information, such as PDA, with providers they trust, 65 potentially facilitating PDA identification and treatment. Similarly, patient-centered communication could enhance chronic disease self-management, 46 a relevant characteristic considering that addiction is a chronic disease. 66 Although further research is needed, the examples illustrate the possible benefits of state-like patient-centered communication behaviors in PDA-related patient interactions.
Limitations
Prescribers were recruited from one region and represented multiple professions and medical fields. The findings may not represent the diversity of prescriber perspectives in general or prescriber perspectives in a specific profession or field. Given the biases associated with self-reported data and that providers could overestimate competence in patient communication, 15 some prescribers could have described communication with patients as more frequent or positive than that which transpires. Despite the potential role of nonverbal communication in provider–patient communication, only verbal communication was examined. Future research can address these limitations and use the findings to inform quantitative, theory-based research on provider–patient communication about PDA.
Conclusions
Provider–patient communication about PDA underpins many initiatives aimed at curbing the PDA-related public health burden. A comprehensive understanding of this interactive process is important for optimizing these initiatives. The findings of this qualitative analysis suggest that it is multidimensional and dynamic, characterized by multiple communication patterns and factors at different levels of influence. They support the application of SCT as a theoretical foundation for understanding prescriber PDA communication behaviors. Further, they suggest that enhancing prescriber state-like patient-centered communication behaviors during PDA-related patient interactions could be beneficial.
Footnotes
Acknowledgements
The authors extend appreciation to the prescribers for their participation in the study. The authors also thank the study staff, graduate students, and other key collaborators for their support and assistance with the study.
Author contributions
RP and NH contributed to study conception and design, data collection and analysis, and interpretation of the results. SM and AH contributed to data collection and analysis and interpretation of the results. KB contributed to interpretation of the results. SM drafted the article, and all authors critically revised it. All authors approved the final article for submission and report no conflicts of interest.
Funding
This study was supported by the National Institute on Drug Abuse of the National Institutes of Health under award number R24DA036409. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The funding agency had no role in the design of the study; the collection, analysis, and interpretation of data; the writing of the manuscript; or the decision to submit the manuscript for publication.