
Abstract
Background
Hospital discharges against medical advice (AMA) is associated with negative health outcomes and re-admissions. Patients with substance use disorders (SUD) are up to three times more likely to be discharged AMA as compared to those without SUD. Studies suggest that undertreated withdrawal and a perception of stigma may increase the risk, however, to date, there are no published qualitative studies exploring the specific reasons why patients with SUD leave prematurely.
Methods
Semi-structured interviews with patients (n = 15) with SUD with documented AMA discharges from our hospital between 9/2017 and 9/2018. Maximum variation sampling was employed to display diversity across gender, race, age, and type of substance use disorder (alcohol vs opioids). Patients were interviewed until no new concepts emerged from additional interviews. Two coders separately coded all transcripts and reconciled code assignments.
Results
Four core issues were identified as patients’ reasons for leaving the hospital prematurely: undertreated withdrawal and ongoing craving to use drugs, uncontrolled acute and chronic pain, stigma and discrimination by hospital staff about their SUD, and hospital restrictions, including not being allowed to intermittently leave the hospital floor. For patients with histories of criminal involvement, being hospitalized reminded them of being incarcerated.
Conclusion
These findings shed light on the reasons patients with SUD are discharged from the hospital AMA, an event that is associated with increased thirty-day mortality and hospital re-admission. AMA discharges represent missed opportunities for the health care system to engage with patients struggling with a SUD. Our findings support the need for inpatient addiction treatment, particularly for management of withdrawal and co-occurring pain, and the need to address health care provider associated stigma surrounding addiction.
Introduction
In the United States, there are approximately twenty-two million adults with substance use disorders (SUD). 1 People with SUD are at risk for medical complications of their use that can result in hospitalization, ranging from infectious complications such as cellulitis to liver disease from alcohol use. Patients with SUD are also at higher risk for many other chronic co-morbid conditions, such as psychiatric illness, that increase their likelihood of requiring hospitalization. As a result, nearly one in five patients on a general medicine ward in the hospital has a SUD. 2
Complicating high rates of hospitalization, patients with SUD are at nearly threefold increased risk of being discharged from the hospital against medical advice (AMA) as compared to patients without SUD. 3 While there are no professional, regulatory or legal standards that delineate when physicians should designate a discharge as AMA, many factors influence a physician's decision to discharge a patient AMA, including the fear of legal liability and to document concern about the patient leaving. 4 , 5 AMA discharges are associated with an increased thirty-day mortality; in one study, the risk of death was double when comparing AMA discharges to those who had planned discharges even after adjusting for confounders such as disease severity and comorbidities. 6 Furthermore, patients who leave AMA are at increased risk of hospital readmission in the following thirty days, ranging from a two-fold to twelve-fold increased risk, as compared to those with a planned discharge. 3 , 7 , 8
A few studies have explored the factors that put an individual with SUD at higher risk for being discharged AMA. Chan et al. found that among patients hospitalized to a particular HIV ward with a history of injection drug use (IDU), approximately 25% of them were discharged AMA, nearly double the percentage of those without a history of IDU. 9 Ti et al. showed that among patients who use illicit drugs, those who reported using heroin at least daily, had experienced incarceration, and/or were unstably employed were more likely to be discharged AMA. 10
Notably, in-hospital methadone and social support are two factors that have been shown to independently reduce the odds of an AMA discharge. 3 Another qualitative study by McNeil et al. found that patients with SUD who had been previously discharged AMA thought hospital-based harm reduction interventions, such as supervised drug consumption services and pharmacotherapy for withdrawal management, would reduce the risk of being discharged AMA. 11 No previous qualitative studies to our knowledge have specifically focused on the reasons patients with SUD are discharged from the hospital AMA.
The purpose of the present study is to describe what patient-reported factors contributed to AMA discharges through semi-structured, open-ended interviews among patients with SUD and previous AMA discharges. This study is unique as it is the first to explore variables associated with AMA discharge among patients with SUDs through qualitative analysis.
Methods
Study design and sample
This is a qualitative, descriptive study. We conducted individual interviews with hospitalized patients (n = 16) at Massachusetts General Hospital who had a history of alcohol use disorder and/or opioid use disorder and who had documentation of having left AMA between 9/01/2017 and 9/01/2018. Patients were identified through the hospital's research patient data registry. Search terms included “alcohol use disorder,” “opioid use disorder,” “addiction,” “injection drug use,” and “alcohol withdrawal”, as well as “discharge against medical advice,” and “AMA discharge.” Maximum variation sampling was used to select patients, identifying patients who displayed diversity across gender, age, race/ethnicity, and type of SUD (alcohol vs opioids). 12 Patients were excluded if they did not speak English. Patients were also excluded if they were admitted to an intensive care unit or psychiatric unit as we assumed their critical clinical situation prevented them from participating in an interview.
Patients were given a $20 gift card for participating. Patients were interviewed until theoretical saturation, the point at which no additional concepts emerged from subsequent interviews. 13 Informed consent was obtained from all participants. Two patients declined to participate in interviews. The Partners Human Research Committee approved this study (Protocol # 2018P000012).
Data collection
The interviewer approached the hospitalized patient at the bedside. Prior to the interview, the interviewer told the patients that the goal of the study was to better understand why patients with SUD often leave the hospital AMA, with the goal to ultimately improve the care provided to these patients. The interviewers clarified that the study was being conducted for research and that they had no role in the care of the patient. Only the interviewer and participant were present during the interview.
We used semi-structured guides with follow-up prompts to conduct the interviews (Supplementary Appendix A). The interview guides encouraged respondents to share specific experiences, which may provide greater specificity and accuracy than general statements. Two interviewers (R.E.S., R.L.S.) who had no prior clinical relationship with any of the participants and were trained in qualitative interviewing 14 conducted and recorded all interviews. Each participant was interviewed once. The average interview time was 18.5 min (standard deviation of 8 min). Interviews were professionally transcribed.
Data analysis
We used the constant comparative method for analysis of interview data. Two researchers (R.E.S., R.L.S) separately assigned codes to four transcripts. Inductive coding was used. Each time a new idea was identified in the transcript, it was assigned a label or ‘code,’ and then the same code was assigned to other quotes with the same idea. 8 By the end of the fourth transcript, no new codes emerged, suggesting that it was not necessary to use additional transcripts to develop the preliminary code list. The researchers then reviewed the four transcripts together, blending their code lists into a single, comprehensive list.
Two researchers (R.E.S., R.L.S.) then separately coded each transcript using the code list. If a new idea emerged during coding that was not captured in the initial code list, it was added. Prior transcripts were then reviewed to search for instances of this new code.
Coded transcripts were entered into ATLAS.ti (version 8.2.34.0 Scientific Software Development GmcbH, Berlin, Germany) to organize data and review quotes within codes. The research team used the coded data to identify themes seen in all or many codes as well as to identify codes that were not captured in these themes. The researchers frequently returned to the original data to ensure that they represented the ideas of the participants. A preset theoretical framework did not guide data collection and analysis.
Results
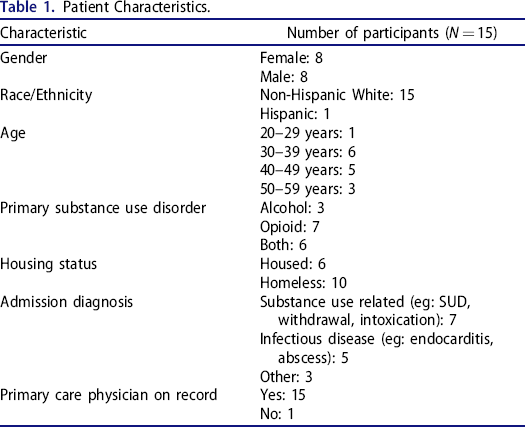
Patient characteristics are displayed in Table 1.
Patient Characteristics.
Interactions with hospital staff
Nearly all patients reported negative interactions with hospital staff which they perceived to be because of their SUD. Patients believed they were judged and treated differently than other patients without a SUD. One patient remarked, “…Anytime that they hear that you're a drug addict they immediately like shut down…it's like they just don't want anything to do with you.” Another patient said, “I felt like I'm an outcast…you always feel like the outcast when you're a drunk. People judging you, and you get sick of people having their opinion on you.”
Some patients commented that they felt that they were immediately stereotyped when they presented to the emergency room because clinicians saw they had a history of SUD in the medical record. One patient said, “If you come here a couple times and you're known on the records as you're a drug addict or you're an alcoholic or whatever, then they label you, and they don't give you the care that you normally should receive.”
On the other hand, a few patients had positive experiences with hospital staff, remarking that they received compassionate care. One patient said, “I've been here, unfortunately, oh, I would say, twenty times. And I've always been treated extremely kind. Everybody's been extremely professional, extremely kind, very caring, understanding, and nonjudgmental.” Most patients had been treated at different local hospitals and commented that the care and compassion they received varied. “[Hospital A] has always been really, really good. They've been always really nice…I've never had that experience at this hospital, ever. And I've never had that experience at [Hospital B]. It's always been at [Hospital C]. And I really don't go to [Hospital D], so don't really know that experience. But as far as those hospitals, [Hospital C] has always been a very bad experience for me.”
Some patients described being reprimanded for their SUD when they were hospitalized for a complication of their use, such as an infection. “Well, I did go there once with an abscess and they weren't very compassionate with that. They were very rude…they was like, “Well, maybe next time you'll think about this before you do this.” Another patient said, “I was getting my blood taken one time and I was like, “Ow, that hurts.” And the nurse was like, “Well, don't you do this for fun?” On the other hand, patients also mentioned that if they presented to the hospital with a medical complaint unrelated to their substance use, health care staff often did not take them seriously. One patient said, “They think you're only there to fucking have the painkillers or whatever, you know what I mean?”
A few patients believed they were not treated well by staff because staff did not understand SUD. One patient said that staff would say, “Sorry that you're sick. Your own fault.” This patient continued, “Like I'm just a piece of shit because I decided to pick a needle up and stick it in my arm and because I continue to do that I'm still just a piece of shit. They don't understand that addiction is a disease.” Some patients believed they would have been treated differently if instead of presenting with a complication of their SUD, for example, they presented with another medical condition that was more clearly understood and relatable. Another patient said, “and because you don't have an obvious open wound or you don't have cancer or you don't have something that they can clinically right there treat on the spot, I think that it becomes – they get confused…they don't understand the problem.”
Some patients also discussed that they were not trusted by staff because of their SUD. One patient said, “If you're in the bathroom and the nurse comes in to do something, she always wants to just open the door, without knocking, just open the door, just to try to bust you in doing something so she can be hero of the day.” Two patients described interactions with hospital security. One was a violent interaction—“I've gotten choke slammed by security into the bed.” Another patient described having security called on them simply because of their SUD. “They make you feel like a criminal because you have substance abuse issues,” he said.
Pain and pain management
Some patients reported that their pain was not adequately controlled which they attributed to the fact that providers felt uncomfortable prescribing pain medications to people with SUD. Patients found this frustrating and disheartening. One patient said, “As we speak, my foot's infected. I'm in a lot of pain. They won't give me nothing for pain because I'm an addict.” Another patient described an experience she had in the emergency department, when she presented in severe pain. She said to the provider, “‘Please give me something. I don't have any money to get any ibuprofen, I don't want to go steal it,’ and I got thrown out by security in a wheelchair.” A third patient described a hypothetical scenario of two patients in the emergency department, one with a SUD and one without. She said, “They both have the same stomach pains. They're going to take care of the person that doesn't do the drugs first, and probably give them medicine to help them, whatever's going on. The other person, no. They'll make them wait for hours and probably give them nothing.”
Many patients mentioned that once health care providers knew they had a SUD, they did not want to treat their pain. From then on, providers did not trust their report of pain and thought instead they wanted pain medications to get high. One patient said, “Anytime that they hear you're a drug addict they immediately like shut down, they don't want to work with you. They don't want to work with pain management.” Another patient reported, “They think you're only there to fucking have the painkillers or whatever, you know what I mean?”
Some patients described that inadequately treated pain was the reason they left the hospital AMA. After leaving, all of these patients used drugs to control their pain. One patient described, “And I've gone through points where the pain – they couldn't get it at a reasonable level, like a tolerable level. And so I left, because I didn't want to sit there and continue suffering. And then as soon as I left, I went straight into self-medication, trying to self-medicate to make the pain lessen.” Similarly, another patient said, “I ended up going to using because I was in so much pain. And doctors don't do nothing for the pain.”
Withdrawal and withdrawal management
Many patients reported that their withdrawal was not adequately treated when they were hospitalized. When discussing how his withdrawal was managed, one patient said, “There's some hospitals that won't give you anything that makes you go through it like cold turkey, which is like impossible.” A few patients specified that certain medications were given to help with withdrawal but this was not sufficient. One patient described, “They [health care staff] just tell you sorry…They'll give you some clonidine and some bentyl and send you on your way. So that doesn't work.” A few patients, however, described that their withdrawal was well addressed. One patient reported, “They've given me Suboxone and that's helped a great deal. That's huge. If I didn't have that, I'd probably be going out of my mind right now.” Some patients also described that hospitals around the city treated withdrawal differently; some hospitals effectively treated withdrawal while others did not.
While most patients described going through withdrawal of illicit substances while hospitalized, a few patients mentioned being denied controlled substances they were prescribed by outpatient providers, causing them to experience withdrawal. One patient said, “They took away all my psych meds, which would be fine except I detoxed off all my meds… I'm detoxing off Klonopins, gabapentin, clonidine. You know what I mean. It's ridiculous. So I'm having cold and hot sweats, shits, everything,”
Nearly all patients made clear how painful it was to go through withdrawal. One patient said, “Dope sick is hell. That's what I explain it. You want to know what hell is? I think dope sick is that. That's hell. It's hell. Hell on earth. I would rather have somebody saw my leg off at the knee than go through that.” A few patients mentioned that they were so afraid of going through withdrawal when presenting to the hospital that they would use drugs before coming in. “I had a few drinks this morning so I could get here,” a patient said. He continued, “But it [the withdrawal] is going to come on, and it's going to come on full force. And I just hope and pray that they just keep my vitals stable so I don't die.” Another patient stated that he planned to bring alcohol with him the next time he needed to be hospitalized to prevent withdrawal. He said, “I wouldn't bring a big bottle. I would bring a little pint. Just to make sure I'd stay for a little while.”
Some patients attributed ongoing withdrawal and cravings to the reason they left the hospital AMA. “Like they weren't giving me detox meds or whatever. So you get to that point, and you're like, “I'm fucking out of here,” and then you leave, and then you go cop,” said one patient. Another patient commented, “I went to the ER…I was getting no help, no nurse came and saw me….My hangover got worse and worse, because the liquor store is still open and I can go get another bottle and take care of myself.” When asked why he left AMA in the past, a patient responded simply, “Just the need to use was more reinforcing than the one to be here.”
When asked what patients did immediately after leaving the hospital, many said they used drugs. One patient said, “When I woke up from anesthesia, I was withdrawing so bad…I was like ‘Just give me my discharges papers and I'm out of here,” because I couldn't wait no longer…Yes, I did get high. I mean, it was the only thing that took those shakes away.”
Hospital restrictions
Some patients described hospital restrictions they found at times unbearable, prompting them to leave the hospital. The most common restriction discussed was the inability to go outside the hospital to “get some air” or smoke a cigarette. One patient said, “…it's just that people that are coming off of a substance is hard enough alone, and the people here don't seem to understand the whole, “I got to go get some air,” thing. When somebody says that they really need to go get some air, I mean, it's either air or it's going to come back on you some type of way.” When asked why they left AMA, a patient said, “Frustration. Dying for a cigarette and the patch and all that wasn't holding me over…and that's when I was a real heavy smoker and I was just, I'd had it, I was like I'm out of here.”
Patients described feeling powerless when they were told they couldn't walk off the floor. One patient said, “It's just powerless, I feel like. You know what I mean? I don't have any control over anything anymore. I pretty much have to put everything in– and even have to have– other people's hands.” A few patients described the hospital as reminding them of when they were incarcerated. When asked why the patient left AMA, one patient said, “Not having a smoke break, not seeing the sun on my face. Just feeling like I'm in an institution.” Another patient commented, “I think if you can walk, you can walk off the floor…It makes it seem more like a prison than a helpful place.”
In addition to the restrictions on mobility, a few patients also described having restrictions on who could visit them in the hospital. One patient reported that her husband was not allowed to visit her because he had a history of drug use. He said, “They won't even let me go out with my husband… He been clean for almost eight months now. He's on the methadone. That's ridiculous.”
Discussion
This study explored why patients with SUD are at higher risk of being discharged from the hospital AMA, the results of which can hopefully inform future interventions to reduce AMA discharges among this population. Through exploratory interviews with patients with SUD with a recent history of an AMA discharge, we have identified four key contributors to this type of discharge: withdrawal and suboptimal withdrawal management, uncontrolled pain, strained relationships with hospital staff, and hospital imposed patient restrictions.
Studies indicate that physicians do not feel equipped to diagnose or treat patients with SUD. 15 Physicians find this type of care overwhelming and they worry about being deceived and manipulated by patients, particularly around pain management and controlled substance prescribing. 16 The lack of standardization of such care leads to inconsistencies and fosters mutual mistrust between providers and patients. Our study supports these findings, as patients describe inadequate withdrawal and pain management. Patients reported this suboptimal care as a major reason they left AMA; many used drugs immediately after leaving the hospital.
Hospitals across the country have been working to improve the care of patients with SUD. Addiction consult teams are becoming increasingly commonplace and can assist in initiating pharmacotherapy, such as buprenorphine and methadone, for the treatment of opioid use disorder, as well as engaging the patient in motivational interviewing and post-hospital navigation to community-based treatment programs. 17 Post-discharge clinics with a low barrier to treatment as well as the incorporation of recovery coaches to assist in navigating the health care system are other examples of how patients with SUD can be engaged in treatment in the hospital and on discharge. 18 These hospital initiatives have been shown to increase physicians’ sense of preparedness and clinical practice in treating patients with SUD. 19 Despite the advent of these various treatment modalities, however, much remains to be done to engage patients with SUD in treatment while they are in the hospital and minimize the risk of harm, including being discharged AMA. This study affirms the need for ongoing research and development of initiatives to better care for patients with SUD in the hospital.
This study also highlights the perceived discrimination experienced by patients with SUD by hospital staff. Patients with SUD perceived that their acute illness and pain—whether related to their SUD or not—was not taken as seriously as for other patients without a SUD. Patients reported feeling judged and reprimanded for their use. Perceived discrimination by health care providers has been documented for many marginalized populations, including patients who are homeless, have HIV and belong to a racial and/or ethnic minority group. 20 , 21 A few studies have examined health care provider discrimination among patients with SUD. One meta-analysis found that such discrimination is common. 22 Providers hold stigmatizing views of patients with SUD, including concerns that these patients are out to manipulate them, that they are dangerous and lack motivation for treatment. 23 , 24 Health care provider discrimination of patients with SUD not only impacts the therapeutic alliance between provider and patient, but has also been shown to negatively impact health care outcomes. 22 Brener et al. showed that perceived discrimination decreased the likelihood that patients completed treatment. 25 The results from this study emphasize the importance of addressing health care provider stigma and discrimination of patients with SUD. Empowering providers to care for these patients through SUD education and awareness of SUD-related stigma, including the importance of language in describing the disease, are key first steps.
In this study, patients emphasized perceived differences in treatment of pain when compared to patients without SUD, describing situations when they would be denied opioid analgesia for their acute pain. This often created an adversarial relationship between the health care provider and patient, and contributed to a patient's decision to leave the hospital prematurely. Providers worry that providing opioid analgesia will precipitate an addiction relapse, or that patients are reporting pain in an attempt to obtain opioid medication to get high. However, as outlined by Alford et al., these fears are unfounded. 26 Opioid analgesia can be clinically indicated to manage acute pain, and the patient's history of SUD should not affect this decision. 26 Educating providers on the management of acute pain for patients with SUD, particularly those with opioid use disorder on methadone or buprenorphine, will likely improve medical treatment and foster a therapeutic relationship.
Patients also highlighted hospital restrictions—for example, not being able to leave the hospital floor—as reasons for being discharged AMA. To our knowledge, this is the first study to document the impact of hospital restrictions on AMA discharges. For some patients, these restrictions reminded them of being incarcerated. One prior study showed that patients with histories of incarceration are more likely to be discharged AMA, 27 and our data suggest that the association between hospitalization and incarceration may play a role. Patients with SUD experience high rates of incarceration, a traumatic and disruptive life event. 28 This finding indicates that it is important for providers to recognize the impact of prior incarcerations on the experience of hospitalization. For this vulnerable population it is particularly important to sensitively weigh the risks and benefits of allowing patients to leave the hospital floor, examine the potential harm of hospital policies, and be mindful of the impact that negative interactions with security could have for someone with a history of trauma within the correctional system.
Nicotine craving as a reason for getting discharged AMA was another important finding from the study. It has been shown that over half of smokers develop nicotine cravings in the first forty-eight hours of hospitalization and one-third report difficulty refraining from smoking. 29 The prevalence of tobacco use disorder is very high among patients with other SUD, approaching 70%. 30 This finding supports the importance of proactively and aggressively addressing nicotine withdrawal once patients are admitted to the hospital.
Limitations
There were limitations to this study. First, the study was conducted at a single hospital, limiting the generalizability of our findings. Notably, however, patients ended up describing their experiences at hospitals across the city. Second all but one of the patients interviewed were non-Hispanic whites. The hospital where this study was conducted serves a predominately white patient population but regardless, the fact that only one nonwhite patient was interviewed greatly limits our generalizability to patients of various racial and ethnic backgrounds, especially given that Black and Hispanic patients are more likely to be discharged AMA. 31 Third, majority (63%) of the patients we interviewed were homeless, which is higher than the rate of homelessness documented in other studies on patients who are discharged AMA. 7 , 32 Fourth, patients interviewed were those who were currently hospitalized, excluding patients who did not return to the hospital after an AMA discharge; it is possible that people who did not return had different experiences than those who did. Additionally, patients interviewed had a diagnosis of either alcohol use disorder or opioid use disorder, which are the most common types of SUD seen in this hospital. However, patients with other types of SUD may offer different perspectives on reasons for leaving AMA.
More qualitative studies are needed to explore the reasons for AMA discharges with a more diverse patient population, ideally those who have been hospitalized at different institutions, are not currently re-hospitalized, and display diversity across racial and ethnic backgrounds. Future studies could evaluate how clinical data such as pain or opioid withdrawal scales predict AMA discharges, and if interventions such as addiction consult teams impact rates of these discharges among patients with SUD.
Conclusions
Patients with SUD frequently are discharged from hospitals AMA. Four major reasons that patients leave AMA are suboptimal withdrawal management, ongoing pain, strained relationships with hospital staff, and hospital imposed patient restrictions. These findings highlight the importance of standardizing interventions to address stigma among hospital staff, to improve withdrawal, pain, and SUD management, and to critically appraise policies that impact patients with SUD during hospitalization.
Footnotes
Disclosure statement
The authors declare that they have no conflict of interest.
Funding
This work was supported by Massachusetts General Hospital (Jackson Society White Coat Grant). The funding organization had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.