
Abstract
Modafinil is a nonamphetamine nootropic drug with an increasingly therapeutic interest due to its different sites of action and behavioral effects in comparison to cocaine or amphetamine. A review of modafinil (and of its prodrug adrafinil and its R-enantiomer armodafinil) chemical, pharmacokinetic, pharmacodynamic, toxicological, clinical and forensic aspects was performed, aiming to better understand possible health problems associated to its unconscious and unruled use. Modafinil is a racemate metabolized mainly in the liver into its inactive acid and sulfone metabolites, which undergo primarily renal excretion. Although not fully clarified, major effects seem to be associated to inhibition of dopamine reuptake and modulation of several other neurochemical pathways, namely noradrenergic, serotoninergic, orexinergic, histaminergic, glutamatergic and GABAergic. Due its wake-promoting effects, modafinil is used for the treatment of daily sleepiness associated to narcolepsy, obstructive sleep apnea and shift work sleep disorder. Its psychotropic and cognitive effects are also attractive in several other pathologies and conditions that affect sleep structure, induce fatigue and lethargy, and impair cognitive abilities. Additionally, in health subjects, including students, modafinil is being used off-label to overcome sleepiness, increase concentration and improve cognitive potential. The most common adverse effects associated to modafinil intake are headache, insomnia, anxiety, diarrhea, dry mouth and raise in blood pressure and heart rate. Infrequently, severe dermatologic effects in children, including maculopapular and morbilliform rash, erythema multiforme and Stevens-Johnson Syndrome have been reported. Intoxication and dependence associated to modafinil are uncommon. Further research on effects and health implications of modafinil and its analogs is steel needed to create evidence-based policies.
Keywords
Introduction
Cognition is defined as the acquisition and use of knowledge and involves memory, attention, perception language, psychomotor functions and executive functions such as response inhibition, interference control, working memory, and cognitive flexibility. 1 Cognitive enhancers, also known as nootropics, are substances thought to improve these mental functions. 2 – 4 Nootropic is a term derived from the Greek words “noos” (mind) and “tropos” (bend), and it was firstly used in late 1990's, by Corneliu Giurgea, to classify piracetam and its memory enhancing properties. 2 , 5 , 6 Nootropics can be pharmaceutical products, although some occur naturally in foods, plants and herbal preparations. 5 Table 1 presents the classification of drugs acting on nervous system including nootropics, based on the Anatomical Therapeutic Chemical classification system and the Defined Daily Dose (ATC/DDD index). This classification includes three main groups of nootropics: i) the centrally acting sympathomimetics (N06BA; e.g., d-amphetamine, d-methamphetamine, cocaine, lisdexamfetamine, methylphenidate, adrafinil, modafinil and armodafinil) that mimic the actions of catecholamines in the central nervous system by stimulating the release and/or reducing the reuptake of monoamines; 7 – 12 ii) the xanthine derivatives (N0BC; e.g., caffeine and propentofylline) function as nonselective adenosine receptor antagonists and therefore counteract the adenosine-dependent inhibition of neurotransmitters release in CNS, promoting psychomotor activity; 13 , 14 and iii) other psychostimulants and nootropics (N0BX) that modulate cholinergic (e.g., meclofenoxate, piracetam, pramiracetam, aniracetam and oxiracetam) and glutamatergic systems (e.g., piracetam, pramiracetam, aniracetam and oxiracetam) and increase mitochondrial activity (e.g., acetylcarnitine and idebenone).15–18
Classification of drugs acting on nervous system including nootropics, based on the anatomical therapeutic chemical classification system and the defined daily dose (ATC/DDD index).
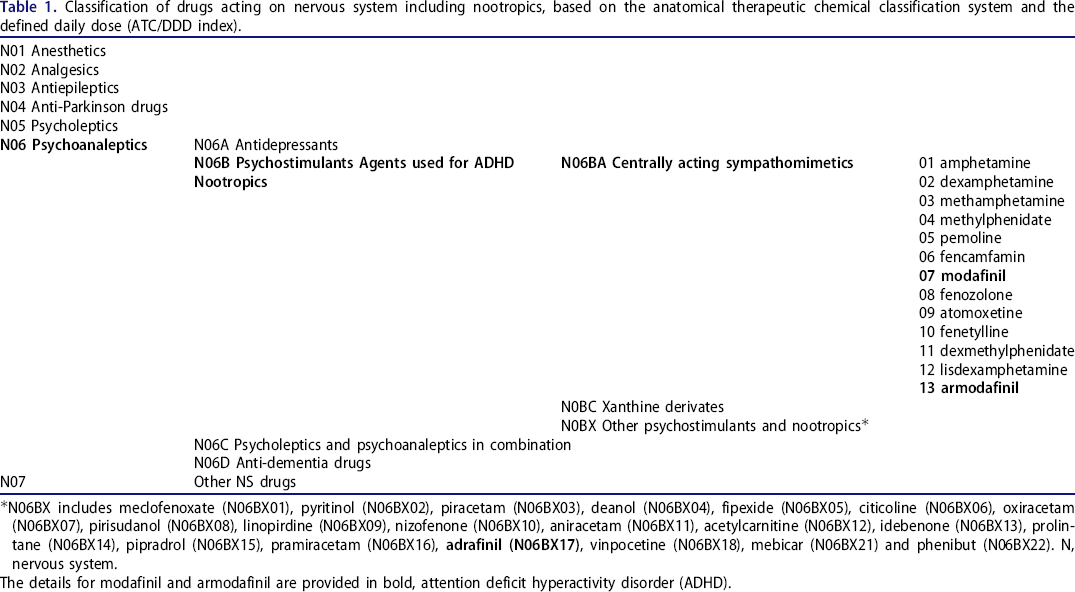
N06BX includes meclofenoxate (N06BX01), pyritinol (N06BX02), piracetam (N06BX03), deanol (N06BX04), fipexide (N06BX05), citicoline (N06BX06), oxiracetam (N06BX07), pirisudanol (N06BX08), linopirdine (N06BX09), nizofenone (N06BX10), aniracetam (N06BX11), acetylcarnitine (N06BX12), idebenone (N06BX13), prolintane (N06BX14), pipradrol (N06BX15), pramiracetam (N06BX16),
The details for modafinil and armodafinil are provided in bold, attention deficit hyperactivity disorder (ADHD).
From a clinical perspective, pharmacological nootropics are supposed to be available only by prescription. Therapeutically, these are mostly used to improve impaired brain performance following various neuropathological or age-related processes such as Alzheimer's disease, schizophrenia, stroke, attention deficit hyperactivity disorder, or aging. 2 However, these substances are also likely to improve intellectual functions in absence of mental disfunction, leading to their use by healthy people for nonmedical purposes (i.e., without official approval). Typically, students use nootropics aiming to increase their learning capacity, concentration and memory, and thus, their academic performance. 19 – 21 Particularly, modafinil (i.e., 2-[(diphenylmethyl)sulfinyl]acetamide) is a psychoactive compound with potential for wake promotion and cognitive enhancement. It was firstly approved by the US Food and Drug Administration (FDA) in 1998 and is currently commercially available under the brand names of AlertecTM, ModavigilTM, or ProvigilTM 22–24
The present work has two main goals: i) describe modafinil and its analogues, including their pharmacokinetic and pharmacodynamic, current clinical use, pharmacologic interactions, toxicological and adverse effects and abuse potential; ii) analyze their off-label use, not only in other medical areas, but also by students for cognitive enhancement and academic performance improvement.
Methodolody
An exhaustive search was carried out in PubMed (U.S. National Library of Medicine) was performed, without a limiting period, focusing on the contextualization of nootropics class and specific information about modafinil and its analogues, namely their chemical and pharmacologic aspects, clinical and off-label uses, forensic and toxicologic information and cognitive enhancement proprieties. Furthermore, FDA and World Anti-Doping Agency (WADA) documents as well as books were reviewed for possible additional information related to this topic.
Chemistry of modafinil and related agents
Figure 1 presents chemical structures of modafinil and analogues. Modafinil is commercially available as racemate (d or S and l or R) with a single chiral center at the sulfur of the sulfoxide 25 – 27 Methods for enantiomeric separation have been developed 28 but both enantiomers were shown to have the same pharmacological activities. 29 It is a white crystalline solid practically insoluble in water and cyclohexane, and slightly soluble in methanol and acetone. 22 Adrafinil (i.e., 2-[(diphenylmethyl)sulfinyl]-N-hydroxyacetamide), is the N-hydroxy prodrug and it is metabolized in its bioactive amide modafinil in the liver. 30 Armodafinil, which contains only the R-enantiomer of modafinil, possesses a specific FDA approval and it is sold by the brand names of ArtvigilTM and WaklertTM. 22 Modafinil is a highly researched compound, with many analogues created and studied (Figure 1); the wakefulness promoting agents CRL-40,490 and modafiendz are the fluoro and N-methyl analogs of modafinil and the CRL-40,491 is the fluoro analog of adrafinil. 30 ,31
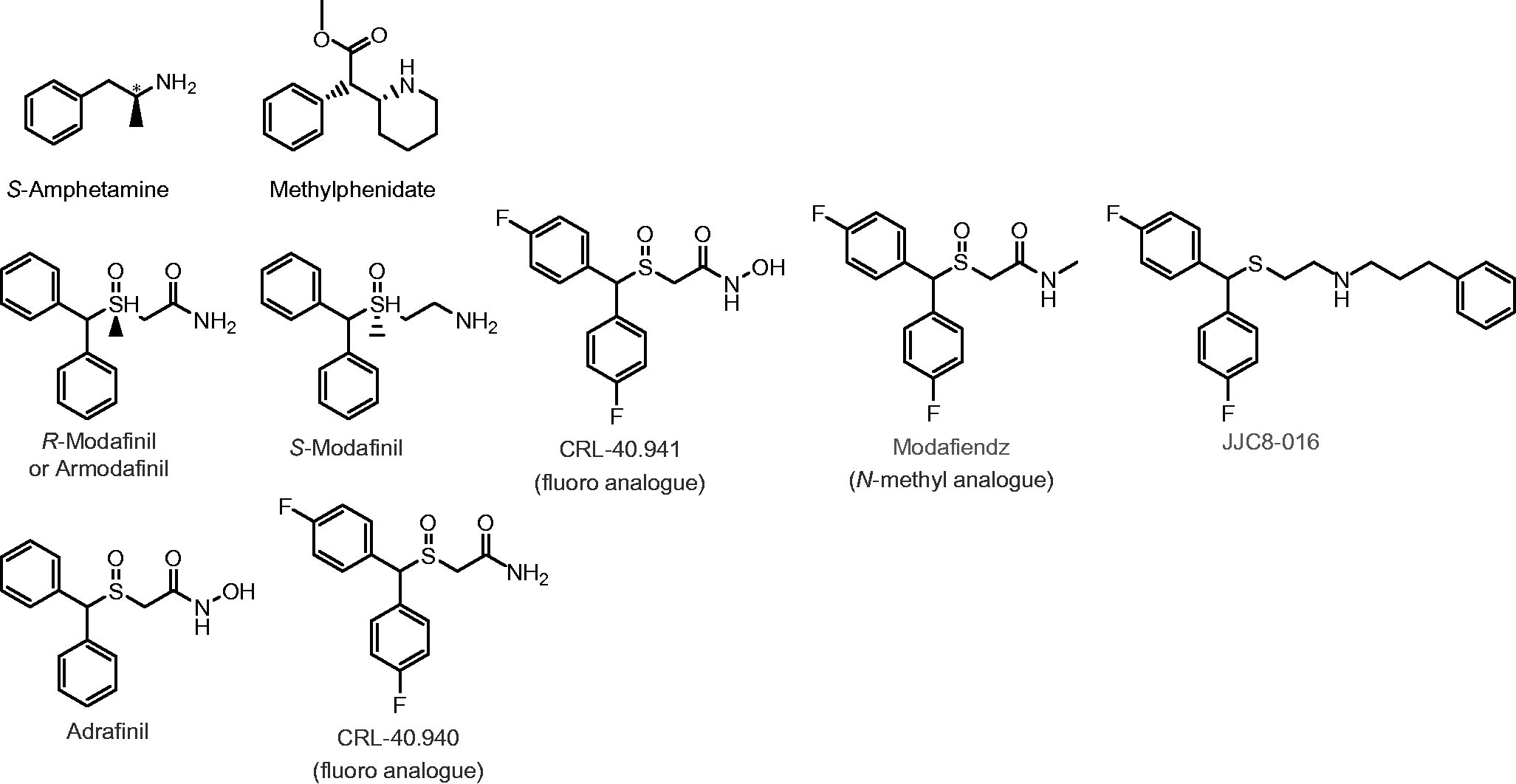
Chemical structures of modafinil and adrafinil, and respective analogs. Amphetamine and methylphenidate structures are also provided for comparison. Note that despite its actions on dopamine reuptake inhibition, modafinil is structurally different from amphetamine and methylphenidate.
Pharmacokinetics
Absorption
Modafinil is at least 40 to 65% absorbed (oral bioavailability) and reaches maximum plasma concentrations (Cmax) 2–4 h after multiple or a single oral intake. Intravenous administration in humans has been precluded due to its low aqueous solubility. 26 Both Cmax and Ctmax are similar for R and S modafinil enantiomers, suggesting a comparable absorption. Although the extent is not affected, absorption may be delayed in 30 min–1 h by the presence of food in the gastrointestinal tract. 27 , 32 An in vitro study demonstrated that both modafinil enantiomers are substrates of P-glycoprotein but also weak inhibitors of this efflux transporter; the clinical significance is yet unknown.33
Distribution
When in circulation, modafinil has a plasma protein binding of approximately 60%, mainly to albumin, and an apparent volume of distribution - after single or multiple oral doses - of 0.8 L/kg, being readily able to penetrate tissues. 27 , 32 At steady state, reached within 4 days of any given dose, R-modafinil constitutes 90% of the concentration of modafinil, proving that the R-enantiomer is metabolically more stable and has a longer elimination half-life. 27 Therefore, when compared on a milligram-to-milligram basis the armodafinil produces consistently higher plasma drug concentrations then modafinil at steady state.34
Elimination
Elimination half-life is approximately 12–15 h, due primarily to the kinetics of its R-enantiomer, as the S-enantiomer has a smaller half-life of 4–5 h. 27 This may be increased in patients with renal or hepatic disease and in elderly, 26 , 35 since metabolization and elimination occurs primarily in the liver. 36 Indeed, renal clearance of the parent drug is not a major contributor to modafinil elimination, comprising less than 10% of the dose. 36 , 37 Modafinil clearance is decreased by approximately 60% in patients with cirrhosis and its Cmax is doubled in patients with chronic hepatic insufficiency. 38 Modafinil acid is the major urinary metabolite, accounting for 35% to 60% of the dose.29
Metabolism and pharmacologic interactions
Modafinil is extensively metabolized in the liver to inactive metabolites before being eliminated in urine: 35 , 39 i) primarily by amide hydrolysis to produce an acid metabolite ((±)2-[(diphenylmethyl) sulfinyl] acetic acid; modafinic acid) catalyzed by an esterase and/or amidase; ii) by S-oxidation via cytochrome CYP3A4 or CYP3A5 to produce a sulfone (2-[(diphenylmethyl) sulfanilyl] acetamide); iii) by aromatic ring hydroxylation; and iv) by glucuronide conjugation (Figure 2). There is no evidence that these metabolites contribute to wake-promoting activity. Adrafinil is a prodrug, and it is primarily metabolized in vivo to its bioactive amide modafinil. 40 Regarding armodafinil (i.e., the R-enantiomer of racemic modafinil), two inactive metabolites reach measurable concentrations in plasma, R-modafinil acid and modafinil sulfone. 26 However, modafinil sulfone does appear to possess anticonvulsant effects, and this is a property that it shares with modafinil.41
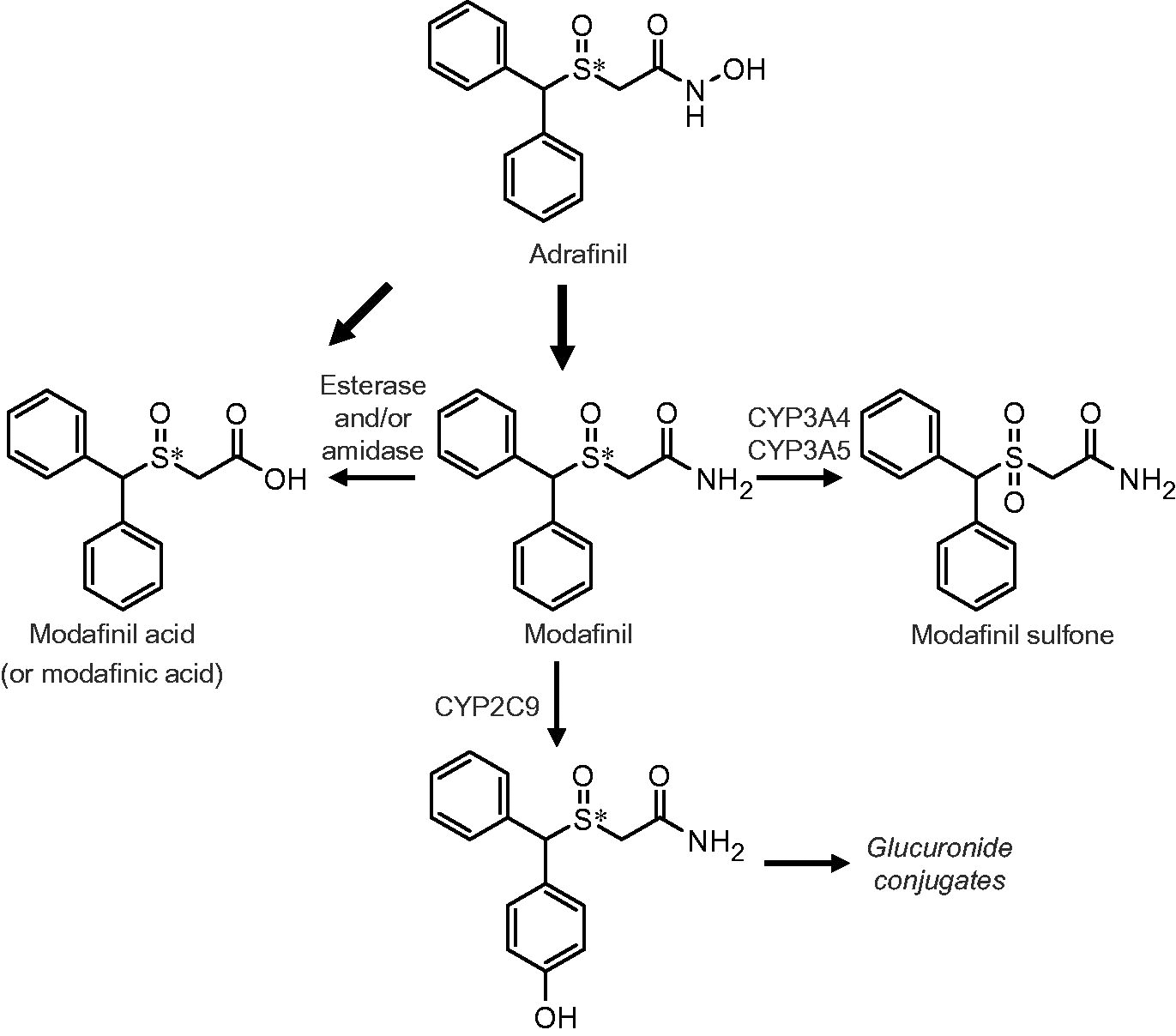
Metabolic pathway of modafinil and adrafinil. Asterisk (*) denotes the stereogenic center.
When evaluated in pooled human liver microsomes, modafinil had in vitro capacity to competitively and reversibly inhibit CYP2C19 in a dose that corresponds, approximately, to human plasma maximal concentration at a dosage of 400 mg/day. 36 It also produced a small, but concentration-dependent suppression of CYP2C9 activity in primary cultures of human hepatocytes. Besides that, it exhibited minimal capacity to inhibit other CYP enzymes, and no irreversible inhibition of any CYP enzyme was observed. 36 On the other hand, modafinil increased, up to 2-fold, the mean activities of microsomal CYP1A2, CYP2B6, and CYP3A4 (the later involved in the formation of modafinil sulfone), compared to solvent-treated controls, an effect less than that produced by reference inducers of these enzymes. 27 ,36
Modafinil is frequently administered concomitantly with other medicines, thus, its potential for metabolic drug-drug interactions is important. Evidences suggest that there is a potential for pharmacokinetic interactions between modafinil and substrates for CYP2C19, such as S-mephenytoin, omeprazole, lansoprazole, proguanil, diazepam, and propranolol, but this seems to be clinical irrelevant. 26 , 36 Additionally, although modafinil shows no interaction in vitro with CYP2D6, levels of CYP2D6 substrates (i.e., tricyclic antidepressants and selective serotonin reuptake inhibitors) may be increased with concomitant use of modafinil in poor metabolizers for CYP2D6, since CYP2C19 provides an additional pathway for their metabolic elimination. 34 ,35
The distinct pharmacokinetic of the R-enantiomer results, predominantly, in a different duration of action between modafinil and armodafinil, and they cannot be safely made equivalent by dose increment of the racemate. 34 , 35 Armodafinil does not seem to induce CYP1A2 but is a moderate inducer of CYP3A4 and a moderate inhibitor of CYP2C19. 42 Several drugs have been proved to have reduced Cmax when used after pretreatment with armodafinil, primarily related to CY3A4 induction. These include the atypical antipsychotics aripiprazole, 43 quetiapine, 44 and risperidone, 45 and the mood stabilizer carbamazepine. 46 Therefore, concomitant use of armodafinil with other drugs on psychiatric disorders treatment may necessitate dosage adjustment, particularly when starting or stopping coadministration of the two drugs. 42 , 45 Dosage adjustments may also be required for other drugs that are substrates of CYP3A4 (e.g., ciclosporin, triazolam, steroidal contraceptives) and CYP2C19 enzymes (e.g., diazepam, phenytoin) when administered with armodafinil. 35 , 42 Although chronic treatment with modafinil and armodafinil does not seem to exert significant effect on the pharmacokinetics of warfarin, more frequent international normalized ratio (INR) monitoring is advisable. 26 , 35 The lack of apparent effect of modafinil on the pharmacokinetics of R-warfarin 47 suggests that the hepatic CYP inductive activity observed in vivo may be less than the proposed by in vitro results.26
Pharmacodynamics
Major implicated mechanisms
Modafinil mechanism of action is not yet assertively explained, but it does not appear to act as a monoamine releaser, as do amphetamine-like stimulants. 35 , 48 The pharmacodynamic properties of modafinil are complex as it interacts with a variety of central pathways, including the catecholaminergic system. 27 Both the R- and S-enantiomers bind to DAT 35 and increase DA levels in different brain areas, including prefrontal cortex (PCF), improving executive functions like attention, impulse control and memory processes. 49 Genetic ablation of DAT eliminates modafinil wake promoting effect in mice. However, since DAT-knockout mice also have downregulation of DA receptors D1 and D2, the possibility of modafinil also binding to D1 and D2 receptors cannot be ruled out. 23 , 50 – 52 Indeed, the R-enantiomer (and not the S-enantiomer) of modafinil, was also found to act as a D2 receptor partial agonist in rat striatal tissue53
Drugs that increase DA levels by blocking its reuptake are dependent on neuronal firing because they can only act after a physiological exocytose of the neurotransmitter. On the other hand, DA releasers like amphetamines can increase DA levels under firing blockage. 54 Since the DA increase, on striatal areas in response to modafinil, is blocked by in the presence of the tetrodotoxin, 55 , 56 supports the fact that modafinil effects are associated with blockage of DA reuptake and not by direct action on D1 and D2 receptors. However, modafinil is weak and has a much lower affinity for the DAT comparing to other psychostimulants, such as cocaine. 23 , 57 – 59 Modafinil and armodafinil seem to display a unique pharmacological profile, binding to a conformation of the DAT different from the cocaine-bound conformation, and more like “atypical” DAT inhibitors. 60 Modafinil and its enantiomers bind preferentially to an extracellular occluded conformation of the DAT and induce an inward-facing conformation of this transporter. 25 , 61 Moreover, the R enantiomer has a 3-fold higher affinity for the DAT than S-modafinil. 25 ,59
Brain areas stimulated by modafinil seem to be distinct from those stimulated by other psychostimulants, namely the striatum and cortex. 62 , 63 Indeed, modafinil induces neuronal activation in areas more directed to wakefulness compared to amphetamine. 62 Particularly, modafinil induced the expression of the biomarker of neuronal excitation c-Fos in cells of the anterior hypothalamus, paraventricular and suprachiasmatic nuclei, amygdala and tuberomammillary nucleus. 64 – 66 In vivo modafinil and armodafinil have shown to significantly increase DA levels in nucleus accumbens and in frontal cortex, 25 , 67 and significantly increased activation in the right middle frontal gyrus, superior/inferior parietal lobule, 68 locus coeruleus and prefrontal cortex 69 on functional magnetic resonance studies in healthy humans. Modafinil also regulates gene expression via epigenetic modifications and increases prefrontal cortex function. 35 Reports suggest that although methamphetamine and modafinil can both increase DA neurotransmission in the medial PFC in mouse, there are similar and contrasting epigenetic and transcriptional consequences that may explain their divergent clinical effect.49
Studies with modafinil and other psychoactive substances that also modulate DA activity (e.g., methylphenidate or d-amphetamine) have been conducted in vivo due to the potential for sequential or concurrent therapy of patients with modafinil and either of the two other substances. 26 Comparing simultaneously and separated single-dose administration of modafinil and methylphenidate or d-amphetamine, there was no statistically significant differences on the pharmacokinetics. 32 , 70 When methylphenidate and d-amphetamine were administrated to patients already receiving modafinil at a steady state dose, statistically significant changes in the pharmacokinetics of modafinil were not observed, comparing to patients receiving only modafinil. 71 , 72 Thus, evidence suggest a low probability of clinically significant drug-drug interaction between modafinil and methylphenidate or d-amphetamine.26
Previous tests in rat brain tissue showed that neither modafinil enantiomer has measurable binding to SERT or NAT. 23 , 25 Moreover, as modafinil is unable to treat cataplexy in narcoleptic humans, 73 it is unlikely to be a NAT inhibitor in vivo because those are characteristically effective as anti-cataplectic agents, unlike DAT inhibitors. 23 , 74 However, modafinil can increase NA levels in both rat prefrontal cortex and medial hypothalamus area.67
Recently, Kalaba et al. 24 generated a novel series of modafinil analogs by substituting the amide moiety with five- and six-membered aromatic heterocycles. These components showed significant DA-reuptake inhibition in vitro, but not caused an amphetamine-like efflux of DA. Several substitutions of the amide moiety resulted on a decreased DAT inhibition compared to modafinil. However, when the amide group was replaced with 2-methylpyrimidine-4-ol, 2-thiophenyl, 3-thiophenyl groups, analogs with higher DAT inhibition activity were obtained. Analogs with 2-methylpyrimidine-4-ol and 2-thiophenyl groups had docked ligand positions to DAT very similar to each other, and both resembled the binding site of cocaine. No general neurotoxicity was observed in male rats with 2-thiophenyl group analog, which may render it suitable for further preclinical development.
Other claimed mechanisms
Besides the primary action of modafinil, generally considered to be on DA and/or NA signaling, influence in other mechanisms have been described. 75 Indeed, R- and S-modafinil demonstrate to interfere with γ-aminobutyric acid (GABA), glutamate, 5-hydroxytryptamine (5-HT), histamine and orexin/hypocretin circuits. 63 , 76 , 77 GABA-releasing parafacial zone neurons represent a cellular substrate underlying sleep drive 78 and their activation completely blocks the behavioral and electrocortical wake-promoting action of armodafinil. This opens the possibility for a shared circuit for the mechanism of action of armodafinil and GABA-releasing parafacial zone neurons. 79 Furthermore, perfusion with 1 mM modafinil in rats enhanced the frequency and amplitude of spontaneous excitatory postsynaptic currents and inhibited the frequency and amplitude of spontaneous inhibitory postsynaptic ones in CA1 pyramidal neurons in hippocampal slices, supporting that modafinil enhances glutamatergic excitatory and inhibits GABAergic inhibitory synaptic transmission. 80 Modafinil has also been shown to elevate extracellular levels of glutamate in dorsal striatum, hippocampus and diencephalon in rats. 81 – 83 Also in rats, it increased 5-HT release in the prefrontal cortex, amygdala and dorsal raphe, 67 , 84 without interfering with 5-HT reuptake process. 85 In the hypothalamus, 5-HT release did not change significantly. 67 Modafinil was found to promote activation of tuberomammillary nucleus and orexin neurons, both implicated on normal wakefulness. 66 Since the tuberomammillary nucleus is the sole source of histaminergic neurons, both the histaminergic and the orexinergic systems seem to be pharmacological targets of modafinil. 63 Stimulation of the wake-promoting system of the brain might occur by removing GABAergic inhibitory input and, consequentially, indirectly activating the histaminergic system.86
Additionally, recent studies suggest that modafinil might increase electrotonic coupling among cortical neurons via of gap junctions and connexins 87 and that its awakening effect depends on integral interconnections between the rostral brain and lower brainstem. 88 Electrical coupling in the reticular activating system synchronizes the activity across populations of cells and because modafinil increases this coupling, it induces arousal. 87 They also support that brain targets for modafinil are in the locus coeruleus, dorsal pontine tegmentum, substantia nigra, tuberomammillary nucleus and dorsolateral hypothalamic area. 88 The presence of many existing hypotheses simply reflects the complexity of the mode of action of modafinil. Still, modafinil differs from other classical psychostimulants, namely amphetamine, methylphenidate and caffeine, because it inducts soft waking without sleep rebound and has a limited addiction, tolerance and neuronal and behavioral excitation potential. 23 , 88 – 90 Armodafinil and modafinil are pharmacologically similar both in animal and in vitro studies, independently of all the questions about their mechanism of action.91
Regarding the evidence of modafinil noradrenergic α1 action, although modafinil wake-promoting effects were blocked by an α1b-antagonist in cats 92 and mice and it was shown to increase phosphorylation of mitogen-activated protein kinase in an α1B-dependent mode in cultured mouse cells, 93 modafinil inefficacy in treating cataplexy in dogs 94 argues against a strong modafinil α1-agonism.
Recently, modafinil administered to young male rats demonstrated an increase of type 1 pro-collagen N-terminal protein (P1NP), collagen type 1 cross-linked C-telopeptide (CTX-1) and augmentation of receptor activator of nuclear factor-κB ligand (RANKL) to osteoprotegerin (OPG) ratio in serum, which are likely related to the increased osteoclast number and trabecular and cortical bone loss.95
Therapeutic applications
Due of its wake-promoting and psychotropic effects, modafinil is prescribed to improve wakefulness in adults who have excessive day sleepiness due to one of the following diagnosed sleep disorders: 96 – 98 i) narcolepsy, as first-line treatment; ii) obstructive sleep apnea (OSA), as an adjunct to continuous positive airway pressure (CPAP); and iii) shift work disorder sleep (SWSD), as first-line treatment. The usual starting dose is 200 mg per day (100 mg twice daily). Nonetheless, it can be gradually increased to 400 mg per day (200 mg twice daily) in case of insufficient response. 99 Modafinil is also approved for Air Force missions in the U.S. as an alternative to amphetamines for military usage and has also been shown to reduce jet lag symptomatology. 24 In 2007, the longer-acting form of modafinil, armodafinil, was also approved for the treatment of excessive sleepiness associated with narcolepsy, OSA and SWSD, 100 , 101 taken in a single dose (varying from 100 to 250 mg) in the morning. 99 , 102 In narcoleptic patients previously treated unsatisfactorily with psychostimulants like d-amphetamine, methylphenidate, or pemoline, modafinil seems to be an effective and well-tolerated treatment for improving daytime wakefulness, regardless of which psychostimulant was taken formerly.103
Modafinil off-label use in psychiatric practice is observed for attention deficit hyperactivity disorder (ADHD), affective disorders, including major depressive disorder and bipolar disorder, schizophrenia and cocaine and amphetamines addiction. 35 Modafinil was shown to improve episodic memory and working memory performance in patients with remitted depression 104 and may be effective in combating the cognitive impairments often seen in major depressive disorder. 105 , 106 In bipolar disease, evidence suggest that modafinil may improve treatment outcomes when used with antidepressant therapy in depressed bipolar patients, particularly in those with problematic sleepiness or fatigue, and it seems a relatively safe and tolerable option. 58 , 107 – 109 Currently, international World Federation of Societies of Biological Psychiatry (WFSBP) guidelines and the Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) already support the adjunctive use of modafinil as the second-line choice for bipolar depression. 58 In schizophrenic patients, both armodafinil and modafinil do not worsen positive symptoms or total psychopathology ratings and cause no significant adverse effects. 110 – 114 They seem to be possibly useful if introduced during the acute phase of illness 110 and when baseline prefrontal cortex function is worse. 115 However, based on current evidence, despite theoretical and preclinical considerations, it is difficult to draw firm conclusions regarding the inclusion of modafinil or armodafinil to an antipsychotic therapy. Indeed, contradictory results exist, trials were performed with small sample sizes and methodological differences failed to demonstrate a benefit of these substances on fatigue, negative symptoms or cognitive function in patients with schizophrenia. 116 , 117 Additionally, due to the CYP3A4 induction by modafinil and armodafinil, physicians must be aware that augmented psychotropic drug metabolism might result in a delayed drug interaction that manifests as a late relapse of the disease. Therefore, it is necessary to monitor and adjust the dose of the maintenance psychotropic to preserve its efficacy.110
The clinical spectrum of effects for modafinil and armodafinil offers a distinct pharmacological profile compared to other catecholaminergic agents such as amphetamines and cocaine. 75 , 118 Indeed, modafinil seems to have low abuse potential, produces wakefulness with an attenuated subsequently compensatory sleep recovery. 23 , 89 One of the main neurobiological mechanisms implicated in cocaine or d-amphetamine dependence is the dopamine dysfunction. 119 , 120 Therefore, psychostimulants with lower abuse potential such as modafinil and armodafinil have been investigated as a possible replacement therapy. 25 , 121 Overall, modafinil revealed promising results in promoting cocaine abstinence in cocaine-depended patients without co-morbid alcohol dependence, 121 , 122 because it reduces withdrawal symptoms 120 , 123 and craving frequency and intensity. 124 , 125 Additionally, modafinil promotes a healthy sleep architecture if administered early in the morning, 126 , 127 which may help reducing lethargy and hypersomnia observed in abstinent patients. Further research on modafinil safety profile may be helpful in establishing a well-tolerated, but still efficient treatment dose. 121 The JJC8-016 (i.e., modafinil analog), which has a higher affinity for DAT then modafinil and armodafinil, and comparable to that of cocaine, appears to be more potent in attenuating cocaine self-administration and to have a superior potential therapeutic utility in the treatment of cocaine abuse in comparison to armodafinil, at the same doses. 128 On the other hand, psychostimulants in general do not significantly reduce amphetamine use or amphetamine craving and do not increase sustained abstinence, and also modafinil replacement therapy does not seem to be useful for treating amphetamine dependence.119
Furthermore, modafinil reduced hypersomnia and improved wakefulness with a reasonable safety and tolerability profile in patients with Lewy body dementia. 129 , 130 Nevertheless, in two patients with Lewy body dementia, the administration of modafinil exacerbated agitation and hallucinations; the psychotic symptoms emerged concomitantly with modafinil administration, and remitted following its discontinuation. As an adjunctive treatment of cognitive impairments in the first episode of psychosis, modafinil improved the ability to analyze emotional face expressions and enhanced working memory, which could have effects on patients social and occupational functioning, though it had no effect on impulsivity, attentional and learning measures. 131 ,132
Improved speed reaction times, self-report ratings of energy and attention, attenuated self-report ratings of “drug effects” in response to a 2 mg nicotine lozenge, 133 reduction of appetite and food intake, and decreased self-report ratings of sleepiness 134 , 135 were observed after treatment with modafinil. As weight gain, lack of energy and attention deficit are related to tobacco smoking relapse, 135 modafinil might be a useful adjunct to smoking cessation treatment. However, modafinil also increased negative affect, without affecting nicotine withdrawal and craving symptoms,133 additionally inhibiting, in some cases, the reduction in cigarette consumption among smokers trying to quit smoking. 136 Therefore, further research is needed to evaluate the response to co-administration of nicotine and modafinil in abstinent smokers.
Fatigue and cognitive impairment are frequently observed in cancer patients, associated to both chemotherapy neurotoxicity and the disease negative experience. 137 – 139 Evidence suggest that modafinil may have a role in the population of patients with cancer suffering from severe fatigue, 140 , 141 due to improvement in sleep, memory, attention, general activity, mood, walking and work ability, relation with other people, enjoyment of life and less drowsiness. 142 – 144 On the other hand, patients with mild or moderate fatigue did not benefited from modafinil treatment and no significant effect of modafinil was found on cancer patients with depression. 141 Armodafinil did not demonstrate significant effect on insomnia or sleep quality, 145 , 146 daytime sleepiness, 147 fatigue 148 or overall quality of life 146 , 147 and was associated to a strong placebo effect. 137 Modafinil is also widely used in clinical practice to treat multiple sclerosis related fatigue, 149 one of the most common symptoms in this group of patients. It seems to be an effective, safe and relatively well-tolerated pharmacologic therapy. 149 , 150 It has also been hypothesized as a potential pro-cognitive adjunct, particularly on processing speed and working memory. 151 Nevertheless, some authors still recommend modafinil use with “caution” advocating a need for larger clinical studies to support its benefits. 152 , 153 Additional research on more precise fatigue parameters in MS and determination of the optimal dosing and treatment schedules are still needed.150
Adverse effects
Although not common reported, modafinil may cause serious side effects, including rash or serious allergic reaction, psychiatric symptoms including depression, hallucinations, mania, suicidal ideation and aggressive behavior, and thoracalgia, tachycardia and dyspnea. 154 – 156 More frequent side effects include headache, diarrhea, back pain, anxiety, nausea, sleep disturbance, dizziness, stuffy nose and gastric discomfort. Modafinil is not approved for use in children for any medical condition since it can cause Tourette's syndrome, hostile behavior, loss of muscle tone and severe muscle weakness, hallucinations, suicidal thoughts, low white blood count and painful menstrual periods. 157 , 158 Armodafinil, in its turn, might also cause life-threatening rash or allergic reaction involving the liver or blood cells. 159 It is also not approved in children and adolescents younger than 16 years of age because neither its efficacy nor its safety has been established. 158 Although modafinil has been proven effective in children and adolescents with ADHD, 156 , 160 the compound has not been approved by the FDA due to the risk of Stevens-Johnson syndrome and potential fatal multiorgan hypersensitivity reactions. 35 , 156 ,161
Taneja et al. 162 tested the effects of modafinil (i.e., 400 mg per day), on the autonomic nervous system of healthy subjects and concluded that it significantly increases heart rate and blood pressure, suggesting caution when prescribing modafinil in patients with cardiovascular disease. Accordingly, other trials have reported a significant increase in heart rate and/or systolic blood pressure as adverse effects in patients taking modafinil at 200 mg 133 , 163 or 400 mg daily dose. 133 , 163 , 164 Additionally, there is also one case report of increase in blood pressure and resistance to antihypertensive medication related with daily 300 mg modafinil or 900 mg adrafinil treatment. 165 Clinically relevant increases from baseline were also observed, at least once, for standing systolic and diastolic blood pressure, supine and standing pulse rate in healthy patients taking 600 mg of modafinil. 37 In the same trial, 800 mg dose panel was discontinued after 3 days of treatment due to clinically relevant cardiovascular alterations, including hypertension and tachycardia. Modafinil doses of 200, 400 and 600 mg were well tolerated. 37 At 200 mg and 400 mg doses, modafinil also caused a significant increase in standing pulse rate, and 400 mg additionally increased standing diastolic blood pressure and supine pulse rate. 37 This suggests that the effects of modafinil on cardiovascular system might be dose dependent and that its maximum tolerable single daily oral dose may be 600 mg. In another study evaluating the tolerability and efficacy of armodafinil, taken for at least 12 months, in OSA or SWSD patients, modest, but not clinically significant increase in blood pressure and heart rate were observed, with the majority of the changes occurring within 3 months of treatment. 166 Furthermore, Kinslow et al. 167 reported the first case of a patient treated simultaneously with armodafinil and tranylcypromine, who developed an acute hypertensive crisis with severe headache, nausea, blurry vision, and neck stiffness. Additionally, there is a case report of a 54 years-old man without prior cardiovascular disease which developed premature ventricular contractions after 2,5 months taking 200 mg of modafinil daily to treat fatigue and lack of concentration. Premature ventricular contractions remitted after 20 days without modafinil administration, returned after 10 days in a challenge with the same dose of the drug and subsided again in 2 weeks after new discontinuation. 168 One the other hand, many other studies demonstrated no significant change in heart rate, blood pressure or electrocardiographic registration associated to the administration of modafinil in doses from 85 mg to 425 mg, either compared to placebo, 156 , 157 , 160 , 169 , 170 or after cocaine, 171 methamphetamine 172 or nicotine lozenge 133 exposure. Data on cardiovascular effects of modafinil and armodafinil suggests that, although not seen in all treated patients, alterations in blood pressure and heart rate may occur in a significant number of patients. 37 , 162 Additionally, the risk of drug synergism with acute hypertensive episodes imposes that modafinil and armodafinil must not be used simultaneously with monoamine oxidase inhibitors.167
A recent trial compared acute subjective, emotional, autonomic, and endocrine effects of MDMA, methylphenidate and modafinil (600 mg) in healthy subjects. 173 All three psychoactive substances produced significant and comparable acute adverse effects compared with placebo, most frequently anorexia, xerostomia, and headache. Modafinil was the only substance producing these adverse effects significantly for up to 24 h and severe adverse effects were not reported. Furthermore, modafinil increased misclassifications of emotions as “angry” on the Facial Emotion Recognition Task and produced a small significant increase in pupil size in the dark, however it was significantly lower than the alteration produced by MDMA. Modafinil had no significant subjective drug effects when using visual analog scales records and it had no effect on cortisol, vasopressin, prolactin or oxytocin plasma concentrations. This is in line with a previous study that reported 100% incidence of at least one adverse event in subjects taking 600 or 800 mg of modafinil, most frequently headache, insomnia, anxiety, and palpitations. With 200 or 400 mg dose of modafinil, this incidence decreased to 50% and 83%, respectively. 37 In patients with major depressive disorder, significant adverse events with adjunctive armodafinil, compared to placebo, were headache and nausea (on 150 mg/day dose) or diarrhea and xerostomia (on 200 mg/day dose). 174 Black et al., 166 in a 12 month study evaluating the tolerability and efficacy of armodafinil, reported mild-to-moderate intensity adverse events, of which headache, nasopharyngitis and insomnia were, by frequency order, the most common. Furthermore, increased brain activation, within a limbic-cortical-striatal-pallidal-thalamic circuit, recorded by functional magnetic resonance imaging was observed during fearful face processing in healthy subjects taking 600 mg of modafinil, suggesting a potential adverse effects on emotion processing. 175 In a systematic safety analysis on squizophrenia patients, total drop and drop out due to adverse events did not significantly differed between modafinil/armodafinil and placebo groups. Dizziness, headache, sexual dysfunction, depression, fatigue and nausea were reported in at least two randomized clinical trials included in the analyses. 110
In recommended doses, modafinil and armodafinil seem to be safe, well tolerated and associated with fewer adverse effects when compared to traditional psychostimulants such as amphetamine or cocaine. 22 , 103 , 157 Indeed, low incidence of adverse drug effects among military aircrew members was recently reported. 176 Nevertheless, medications that increase arousal, including modafinil and armodafinil, might have effect on mood scales due to their excitatory profile that can give raise to distress, hostility, irritability, feeling scared, nervous or jittery. 133 ,136
Among children and adolescents, several trials reported insomnia, headache, decreased appetite, abdominal pain, fever and anxiety 156 , 157 as adverse events that lead to discontinuation of the treatment in some cases. There are also reported cases of maculopapular and morbilliform rash, erythema multiforme and Stevens-Johnson Syndrome possibly related to modafinil, 157 which resolved without sequelae. 156 From 1999 to 2007, five reports of post-marketing severe cutaneous adverse reactions have been reported, during which time approximately 673000 adults have taken modafinil worldwide. United States Food and Drug Administration requires additional evaluation on the relationship between the skin rashes and modafinil and armodafinil.156
Abuse potential, dependence and withdrawal
Modafinil and armodafinil are a federally controlled substance in the USA (C-IV) because they are considered to have, theoretically, some abuse and dependence potential. 55 , 91 , 96 In countries other than the USA, modafinil and armodafinil are not classified as controlled substances, 177 and evidence suggests that their abuse and dependence potential is limited at therapeutic doses. 118 There are some practical features associated to modafinil that appear to decrease its abuse liability in comparison to other CNS stimulants. 178 , 179 Modafinil has low potency, requiring high doses to produce prominent stimulant effects, and slow onset of effects, observed only 60–100 min after administration. 180 It is insoluble in water, making its parenteral administration uneasy, 22 and it is very sensitive to heat, eliminating the possibility of smoking the compound. 181 An alternative to produce solutions that can be delivered parenterally is the use of potentially noxious vehicles in which solubility is also limited to relatively low concentrations, eventually requiring high injection volumes. 180 Cost and availability are other factors that might also contribute to a low abuse potential. 181 From the pharmacodynamic point, both modafinil and R-modafinil bind to a conformation of DAT different from that observer for cocaine and closer to the one of JHW007, an atypical DAT inhibitor. 25 In vitro, besides the need of doses of modafinil and its enantiomers 10 to 15 times higher than those effective for cocaine to obtain DA elevations, lower maximal effects on DA levels where observed for modafinil and its enantiomers, comparing to those of cocaine. This supports that, although they block DAT, they do so differently than cocaine. 25 , 59 Evaluation of discriminative stimulus effects in rats and reinforcing effects in rhesus monkeys showed that modafinil was over 200 times less potent than d-amphetamine and was also less potent than ephedrine inducing reinforcing and discriminative stimulus. 182 Additionally, limited self-reported effects, like euphoria and hyperactivity, at daily doses between 200 and 600 mg 183 , 184 and absence of reinforcing or rewarding effects in naive rats 185 suggested a low addictive potential for modafinil and its enantiomers.
However, it remains possible that at high doses and especially if given via a rapid route of administration, modafinil could be addictive. 75 , 182 Modafinil dependence might be related to the DAT blockade, leading to increased DA concentrations in the brain areas linked with reward pathways, observed in both rats and humans. 163 , 186 In agreement with this view, modafinil at high doses (75 mg/kg) produces a conditioned place preference in mice, 187 although a lower dose did not produce that effect. In mouse, priming injection of a high dose of modafinil (64 mg/kg) quickly induced behavioral sensitization to challenge injections of modafinil administered 4 h later. 188 Modafinil also produced conditioned place preference in mice, that became cross-sensitized in a bidirectional and addictive way with cocaine, both with repeated or a single administration of moderate or high doses (64 to 300 mg/kg). 188 , 189 Increase in experiences of a “high”, similar to the one provided by methylphenidate, has been reported in polysubstance abusers administered with 800 mg daily of modafinil, 190 also a higher dose than at which it seems to have a dose-independent pharmacokinetic.
There are 4 case-reports of modafinil dependence syndrome 191 – 194 according to DSM-IV/V criteria including self-initiated increase in dose, psychological craving, unwillingness to cease and development of risky use, continued attempts to obtain modafinil and social and occupational impairment. Three of the patients involved in those cases suffered from psychiatric disorders, namely schizoaffective disorder 191 , 192 and bipolar disease, 194 and one had a history of methamphetamine dependence. 193 Any case-report of abuse or dependence was found on patients taking modafinil to treat a medical condition to which it is currently approved. A first case of modafinil dependence was reported in 2012 involving a 53-year-old man diagnosed with schizoaffective disorder and tobacco and benzodiazepine dependence. After being prescribed modafinil 100 mg per day, along with sertraline and amisulpride for symptoms of fluctuating sadness, lethargy and sedation, he started to self-increase modafinil dose to overcome his boredom and fatigue, reaching a maximum dose of 1500 to 2000 mg per day. With this dose, the patient started to have slurring of speech and poor attention and concentration and continued to take modafinil against the advice of family and psychiatrists. 191 Another patient with schizoaffective disorder in partial remission was prescribed modafinil 200 mg, along with the risperidone and amisulpride. He gradually increased the dose of modafinil to overcome the drowsiness to a total of 1200 mg/day. After six months taking the a supratherapeutic dosage of 1200 mg/day, whenever he skipped modafinil, he claimed to have symptoms of lethargy, weakness, tremors, anxiety, irritability, erratic sleep hours and difficulty in concentrating at work, and reported a sense of well-being only when taking the drug at that dose. 192 A patient with bipolar disease in remission taking 400 to 600 mg of modafinil per day to overcome fatigue, increase energy and improve concentration reported strong craving, aches and pains in body, low mood, lethargy and had decreased confidence and concentration at work whenever he skipped one take. To overcome the fear of relapsing into depression he self-escalated the daily dose of modafinil to a supratherapeutic dosage of 1000 mg/day and started having side effects in areas of psychic, autonomic and other with global interference in life, including hypersexual behavior. Hypersexuality as a side effect of modafinil overuse is not commonly seen. Upsurge of dopamine in the mesolimbic pathway after a supratherapeutic dosage of modafinil might explain for the development of hypersexuality in this case, although the exact pathophysiological mechanism is unknown. 194 Lastly, a 23-year old man with methamphetamine dependence history was prescribed modafinil 200 mg as an adjunctive treatment for daytime hypersomnolence and fatigue associated to methamphetamine withdrawal. The patient was admitted 6 months later with a methamphetamine induced psychosis and he had also been using modafinil at a self-increased dose of 400 mg per day. After psychosis resolution the patient became extremely agitated regarding the planned modafinil cessation because he stated that he was more concentrated, feeling energized and becoming more productive and that his chronic methamphetamine use decreased significantly since he was using it. However, his parents attributed recent difficulties in social and occupational functioning to his daily modafinil use.193
Additionally, there is a case report of both modafinil and armodafinil abuse in a patient with a heavy substance use history, including mixed amphetamine salts, crack cocaine and benzodiazepine. He abused modafinil for 2 years (obtained via the internet) and declared that it made him feel good like smoking crack cocaine. Despite only being prescribed 250 mg per day, he started taking 1200 mg of armodafinil daily. In the emergency department, where he went complaining of anxiety, he was diagnosed with psychosis, anxiety, paranoia, and hyponatremia.195
In all case-reports the patients ended up accepting modafinil intaking cessation. The 23-year old patient consuming the reasonable dose of 400 mg per day agreed to cease modafinil and did not experience any withdrawal symptoms. 193 In the other cases, with the modafinil doses consumed ranging from 1000 to 2000 mg per day, the dose was tapered slowly and benzodiazepines were used to manage withdrawal symptoms. 191 , 192 , 194 , 195 Olanzapine was also used in the last case to manage psychosis and manic behavior. 195 Reported symptoms associated to modafinil withdrawal were sleep disturbance, increased sense of body warmth, lethargy, low mood, 192 and manic behavior, including flight of ideas, inappropriate sexual comments to female, pressured speech and incessant talking, delusions regarding his neighbor, extreme drowsiness and insomnia.195
Withdrawal symptoms associated to substance dependence might range from physical symptoms like lethargy, tremors, anxiety and erratic sleep hours, to more severe psychological consequences. 194 In a study involving ADHD children, a 7-week fixed-dose treatment with modafinil (doses ranging from 340 to 425 mg per day) was followed by an abrupt discontinuation of the medication, with a 2-week withdrawal observation period. Any withdrawal symptom was reported in association with the abrupt discontinuation of modafinil, neither was rebound hypersomnolence nor exacerbation of ADHD. 160 In rhesus monkeys, intake of modafinil up to 36 mg/kg was also associated with no observable withdrawal manifestations after an abrupt intake cessation. 182 , 196 Moreover, modafinil and armodafinil seem to show a certain selectivity for the brain regions involved in wakefulness and the interaction with nucleus accumbens would be less relevant, suggesting reduced addictive potential. 58 ,59
Apparently, at high doses modafinil might have a pattern of use characterized by craving, tolerance, escalating doses use and withdrawal. The withdrawal symptoms are mostly nonspecific and subsided when the dose is decreased in a controlled environment. 191 , 192 , 194 On the other hand, at recommended doses it has not shown the propensity to produce dependence, tolerance and withdrawal like those associated with chronic amphetamine and cocaine use. 62 , 118 Modafinil should be prescribed cautiously, and clinicians should be aware of its possible abuse potential if used incorrectly, especially in patients with psychiatric disorders or with a history of drug abuse. 91 , 191 , 193 There is a need for further systematic studies to evaluate the extent of its abuse and dependence potential when given in different doses.191
From a different forensic perspective, modafinil was added to the stimulant-drug list prohibited (i.e., classified as a “non-specified stimulant”) by the WADA in 2004, after its first report as doping in 2003 at the World Track and Field Championship; adrafinil was also added to the prohibited list. 197 – 199 In sports, modafinil and adrafinil are currently considered to increase alertness without the addictive potential of traditional stimulants, becoming substances with important doping potential. 200 Moreover, modafinil has been shown to prolong exercise time to exhaustion while performing at 85% of VO2max and also reduces the perception of effort required to maintain this threshold. 201 The minimum required performance limit for both modafinil and adrafinil is 500 ng/mL. 202 A liquid chromatography tandem mass spectrometry (LC-MS) method followed by gas chromatography-mass spectrometry (GC-MS) for the screening and confirmation of adrafinil, modafinil and modafinil acid, in human urine has been developed and validated. 40 The limits of detection for the three compounds were lower than the minimum required performance limit for stimulants at the concentration of 500 ng/mL established by WADA. This method has been successfully applied to routine analyses and the WADA Proficiency Test for doping control purposes.40
Cognitive enhancement in students
In addition to its approved use for treating excessive somnolence, modafinil has become increasingly popular among healthy people for cognitive enhancement, namely as academic doping. 203 – 205 The expectations when using neuroenhancement are associated with addressing the challenges of everyday academic life. Students use stimulants as modafinil to: i) overcome tiredness and sleepiness; ii) increase concentration and vigilance; iii) improve their memory and cognitive potential; iv) cope with stress, anxiety and pressure to succeed; and v) be able to work longer hours before a deadline. 20 , 206 , 207 Less commonly, curiosity and the will to have fun are also referred as motives for stimulants consumption. 206 The competition element is frequently referred as a trigger factor, 207 although pharmacologic cognitive enhancement in academia is commonly compared by the students to doping in sports, with an unfair connotation. 208 The use of cognitive enhancers is also frequently advised by friends, family, physician or pharmacist.20
Although the long-term effects in healthy individuals are unknown, modafinil is easily available online with limited information about the use of and potential harms related to the drug. 20 , 209 Other possibilities available from online shops and other retail outlets include adrafinil, CRL-40,940, CRL-40,941 and modafiendz. 30 Alternatively to online purchase, students also report to obtain stimulants from a pharmacy with or without prescription, from colleagues, friends or family, or from an herbalist.20
As mentioned above, in vivo modafinil and armodafinil have shown to significantly increase DA levels in nucleus accumbens and in frontal cortex, 25 , 67 and activates the right middle frontal gyrus, superior/inferior parietal lobule, 68 locus coeruleus and prefrontal cortex 69 on functional magnetic resonance studies in healthy humans. Evidence on the role of DA in frontal lobe functions, as working memory, suggests a close and possibly direct role of stimulants like modafinil in cognition. Additionally, considering that distinct behavioral functions are inter-related, the role of DA in motor function, reinforcement and higher order cognition – classically attributed to DA modulation in mesostriatal, mesolimbic and mesocortical systems, respectively – might be at some extent associated with learning, memory and decision-making functions (Robbins 2005). However, studies relying on attention tests in healthy subjects did not find consistent benefits of modafinil intake, 210 – 213 although few studies showed increased alertness 214 – 217 that is possibly inversely correlated with the IQ. 218 Modafinil appears to exert a relevant effect on executive functions, 203 with more prominent effects in higher executive functions such as planning, decision making, and fluid intelligence. 211 , 219 , 220 Measurable, though limited benefits were also observed in inhibitory control 204 , 211 , 221 and working memory. 211 , 215 ,216
Recent evidence suggests that modafinil does not seem to have positive effects on mental processes that sustain studying tasks in students under normal conditions. 222 In healthy non-sleep-deprived adults, modafinil also did not display a significant tendency toward ‘overconfidence’ for task-level assessments of performance. 214 On the other hand, modafinil seems to have a more notable effect when used in disadvantageous conditions, including illness or sleep deprivation, facilitating the nervous system to achieve full arousal levels. 218 , 222 Nevertheless, when modafinil is administered to already sleep-deprived individuals, the marked improvement in subjective sleepiness and increased vigor caused participants to overestimate their cognitive abilities. 223 Considering that sleep-deprivation is not rare among students, especially nearly exams or deadlines, 206 the true extent of academic neuroenhancement is possibly smaller than the perceived in those circumstances. Furthermore, comparing to non-neuroenhancement users – who are more likely to believe in neuroenhancers negative side effects – students using neuroenhancer medications tend to have a stronger confidence on the positive impact of those substances on their cognitive performance.206
There is no consensus on the extent and nature of modafinil neuroenhancement in healthy subjects, with discrepancies in methodology and outcomes within studies impeding a better definition of modafinil effects on cognition. 224 A more comprehensive understanding of the subjective and effective enhancing properties using more uniform methodological approaches focused on the principles of sensitivity, reproducibility and ecological validity is recommended to detect valid, robust and consistent effects in healthy populations. 203 Potential adverse effects on emotion processing 175 and possible detrimental effect on decisions in everyday life – associated to a choice bias in favor of previously rewarded choices – have also been reported among healthy subjects taking modafinil. 225 Additionally, all other possible adverse effects and the not totally refutable abuse potential must not be forgotten when considering modafinil as a recommended neuroenhancer.
Intoxications
Overdose by modafinil is uncommon and life-threatening toxicity (even with reported ingestions of doses up to 12 g) is rare, and deaths were not yet reported. 226 , 227 Overdose of modafinil is usually associated with insomnia, agitation, dizziness, tremors, tachycardia and rise in blood pressure. 194 A retrospective multi-poison center study in 11 USA states found 137 cases of single-substance overdose with modafinil between 2000 and 2007. 228 Effects of modafinil overdose were generally mild with predominantly tachycardia and CNS toxicity, including insomnia, agitation, dizziness and anxiety. Most patients were managed in a health-care setting, although 45 patients were able to be managed at home. Only 23 required a medical admission and specific medical therapy was warranted in a minority of patients. 228 In another review of single-substance ingestion of modafinil, 87 cases were reported between 1998 and 2008 to the California Poison Control System database, of which 33 were intentional overdoses. 227 Described adverse effects were, in a descending order, tachycardia, agitation, anxiety, headache, hypertension, dystonia, tremor and dizziness. Twenty tow patients had no symptoms, and the majority had minor effects and were managed at home. 227 Between 2004 and 2014, the New South Wales Poisons Information Center (NSWPIC) received 1735 calls about intentional exposures to ADHD medications and modafinil was involved only in 18 cases. 229 Furthermore, 2 h following ingestion of 5 g of modafinil, in a suicide attempt, a 15-year-old adolescent developed headache, nausea, abdominal pain and prolonged QTc interval on electrocardiogram. Additionally, she was unable to fall asleep for 24 h and developed tachycardia and dyskinesia. Kidney and liver functions, complete blood count and blood pressure remained within normal values. 230 One case of suicidal ideation due to multiple drug overdose was reported in a trial testing modafinil for methamphetamine dependence treatment. 231 More recently, a suicide attempt case of a 17-year-old girl was reported with 12 g of modafinil. The patient was studying for the university entrance exams and due to various anxiety and stress, she ingested 12 blister packs of 10 tablets each containing 100 mg modafinil. The patient stayed in intensive care unit for a month and was later presented to a psychiatrist due to persistent psychosis.232
The treatment of intoxications is primarily supportive, associated with sedation, control of dyskinesias and blood pressure. 226 ,228
Conclusions and future perspectives
Several organic, functional and psychiatric disorders can result in sleep disturbances, mood alterations and symptoms like fatigue, lethargy and daily sleepiness that impair diverse executive functions and decreased cognitive abilities. 35 , 233 Mental health and cognitive abilities are important subjects in general public health, and in specific, in the academic world due to the everyday cognitive challenges and the high competition level between students. 20 , 206 Consequently, substances that improve cognition without relevant adverse effects and with low abuse and dependence potential might be extremely attractive in a variety medical and non-medical areas. This work aimed to fully review pharmacokinetic and pharmacodynamic, clinical and forensic aspects of modafinil, adrafinil and armodafinil (Figure 3).
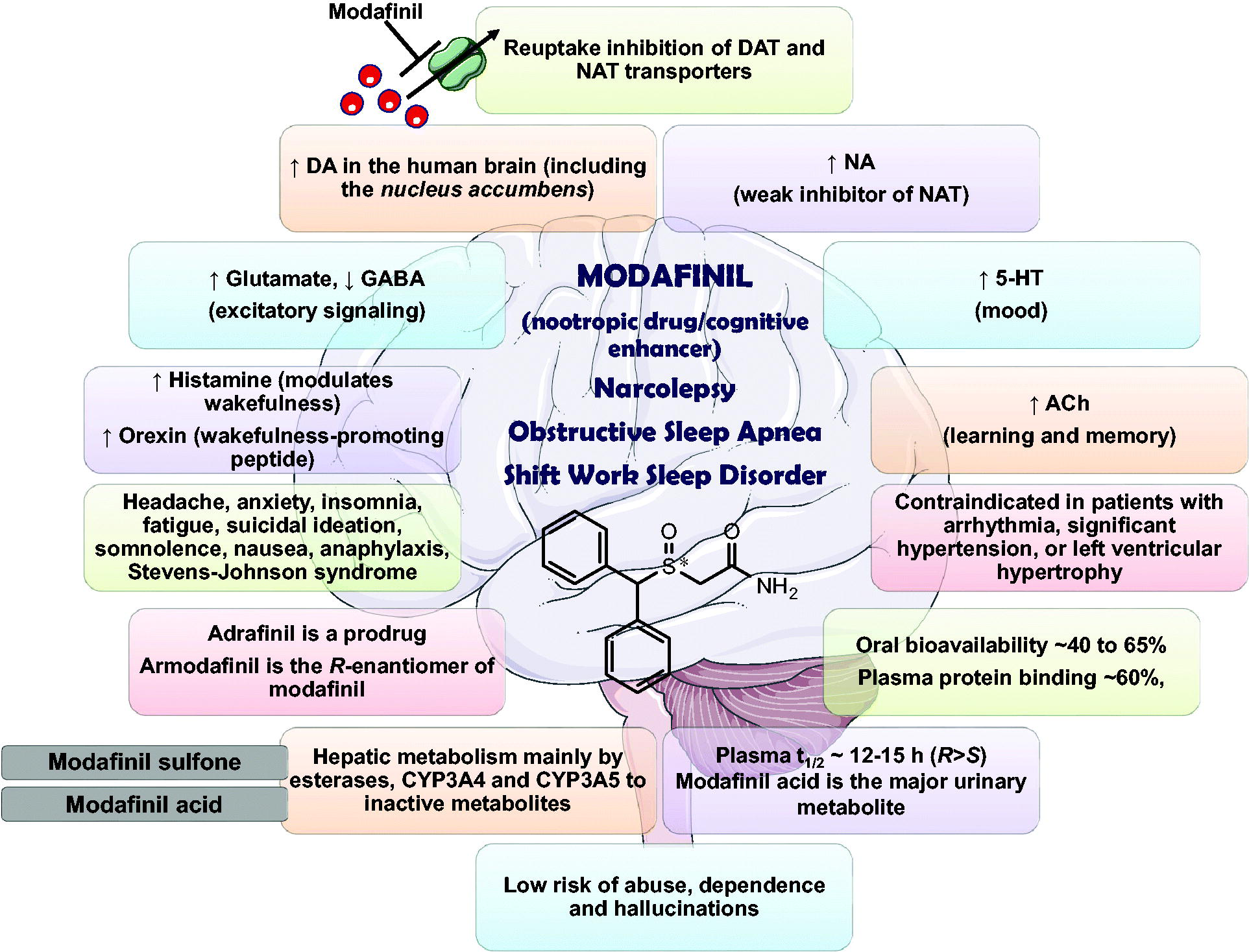
Pharmacokinetic and pharmacodynamic aspects of modafinil. DA, dopamine; NA, noradrenaline; 5-HT, serotonin; GABA, γ-aminobutyric acid; ACh, acetylcholine; CYP, cytochrome P450; NAT, noradrenaline reuptake transporter; DAT, dopamine reuptake transporter.
Modafinil is a wake-promoting agent with a complex profile of neurochemical and behavioral effects, already approved by FDA for the treatment of excessive day sleepiness in the setting of narcolepsy, OSA and SWSD. 97 , 99 Modafinil acts as a weak DAT inhibitor, with the concomitant ability to modulate noradrenergic, serotoninergic, GABAergic, glutamatergic, histaminergic and orexinergic systems. 234 As a generally well-tolerated substance, with less abuse potential than amphetamines, modafinil is increasingly being used in several off-label situations. Although still requiring additional and better evidence on its efficacy, adverse effects and abuse liability, modafinil has several promising off-label applications in psychiatry and other medical areas in which cognitive impairment or fatigue are observed among ill patients. 35 , 49 , 163 The risk-benefit of modafinil must be weighted and therapeutic monitoring is recommended since self-escalation of dose by the patient might be possible and it is more frequently associated to adverse effects and abuse potential. 37 , 190 Although several analytical methods have been developed for quantification, it should be highlighted that there is evidence on the thermal degradation of modafinil, adrafinil, modafinil acid, CRL-40,940 and CRL-40,941 in the GC-MS injector with formation of common degradation products (1,1,2,2-tetraphenylethane and its fluoro analog) when acetonitrile, dichloromethane or ethanol are used as solvents. 30 This might be particularly challenging in forensic diagnosis if a straightforward implementation of GC-MS is made in routine toxicological analysis. Moreover, adrafinil, modafinil and modafinil acid were detected as a single artefact, with no possible differentiation between them, under electron impact ionization in gas chromatograph–mass spectrometer (EI-GC-MS) analysis of urine samples. 202 Nevertheless, using electrospray ionization-liquid chromatography/tandem mass spectrometry (ESI-LC/MS/MS) adrafinil, modafinil and modafinil acid drugs could be detected and differentiated with no artefact in human urine samples.202
Finally, it is steel needed to stablish if modafinil has a true cognitive enhancing potential in healthy subjects, or if it is predominantly associated to a placebo effect. 206 , 223 Additionally, effective doses must be defined with regard of modafinil potential adverse effects. Indeed, among students, not only health but also moral issues might raise with the use of substances like modafinil for cognitive enhancement. 235 , 236 Besides the possible adverse effects and abuse potential, cognitive enhancing drugs, including modafinil, may undermine education as a practice-oriented activity, directed to stimulation of critical thinking, by functioning as a procrastination support. 235 , 237 , 238 If modafinil and its analogs have some proven enhancing effect, truly enlightening information should be available on the pros and cons of their use, 235 and an appropriate system of regulation is recommended to avoid cases of students taking an absolute control of their own learning experience and to refrain the dangers of these drugs misusing.
Footnotes
Disclosure statement
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending or royalties. No writing assistance was utilized in the production of this manuscript.
Funding
This work was supported by grants from CESPU [TramTap-CESPU-2016, Chronic-TramTap_CESPU_2017 and TraTapMDMA-CESPU-2018].