
Abstract
Background: Having prescribers use clinical video teleconferencing (telemedicine) to prescribe buprenorphine to people with opioid use disorder (OUD) has shown promise but its implementation is challenging. We describe barriers, facilitators and lessons learned while implementing a system to remotely prescribe buprenorphine to Veterans in rural settings. Methods: We conducted a quality improvement project aimed at increasing the availability of medications for OUD (MOUD) to Veterans. This project focused on tele-prescribing buprenorphine to rural sites via a hub (centralized prescribers) and spoke (rural clinics) model. After soliciting a wide-range of inputs from site visits, qualitative interviews of key stakeholders at rural sites, and review of preliminary cases, a “how-to” toolkit was developed and iteratively refined to guide tele-prescribing of buprenorphine. After internal and external facilitation strategies were employed, Veterans with OUD at three clinics were transitioned to buprenorphine treatment via telemedicine. Results: Factors impacting adoption of the tele-prescribing intervention were mapped to the Consolidated Framework for Implementation Research (CFIR) constructs. Barriers to adoption included concerns about legality of tele-prescribing a controlled substance, conflicting interests between different stakeholders, and coordination with an existing buprenorphine program requiring more attendance and abstinence from Veterans than the tele-prescribing program required. Factors facilitating adoption included a sense of mission around combating the opioid epidemic, preexisting use of and comfort with tele-prescribing, and rural sites’ control over Veterans referred to tele-prescribers. A total of 12 patients from rural areas were successfully transitioned onto buprenorphine, of whom 9 remained on buprenorphine 6 months after initiation of treatment. Conclusions: Implementing tele-prescribing was negotiated with stakeholders at the target clinics and operationalized in a toolkit to guide future efforts. Implementation issues can be addressed by activities that foster collaboration between hubs (centralized prescribers) and spokes (rural clinics) and by a toolkit that operationalizes tele-prescribing procedures.
Introduction
Buprenorphine is a Medication treatment for people with Opioid Use Disorder (MOUD) that facilitates retention in addiction treatment, 1 abstinence from opioids, 2 and reductions in all-cause and drug-related poisoning mortality. 3 Prescribing buprenorphine via telemedicine (tele-buprenorphine) – primarily with the use of live videoconferencing – has been as effective in maintaining patients in substance abuse treatment as prescribing buprenorphine via face-to face visits in studies with non-randomized designs, although controlled comparisons are lacking. 4 – 6 The use of tele-buprenorphine has been found to be especially promising in rural areas where access to appropriately trained and licensed providers is lacking. 7 Although the requirements for establishing a tele-buprenorphine program have been described, uptake of this life-saving treatment modality lags, reflecting challenges to implementation. 8 , 9 Facilitators in implementing tele-buprenorphine have been previously described as having strong champions in facilities who advocate for the use of this modality, resources for startup costs, established reimbursement pathways for visits, adequately functioning and safe telecommunications equipment, and feasible, operationalized tele-buprenorphine procedures. 10 Barriers to dissemination of tele-buprenorphine according to existing reports include technology-related barriers, reimbursement issues, staff and provider hesitancy, and lack of appropriate implementation models to follow. 11 – 14
Implementation of tele-buprenorphine in the Veterans Health Administration (VHA) is distinct from implementation in other systems because the VHA is an integrated healthcare system with established telemedicine programs and different provider reimbursement issues than in the private sector. Approximately, half of the US Veterans enrolled in VHA care, receive their healthcare at Community Based Outpatient Clinics (CBOCs), with many of these located in rural settings. 15 A number of recent VHA policy changes and initiatives support the adoption of tele-buprenorphine programs. First, a major VHA priority has been to improve rural Veterans’ access to buprenorphine and other Medications for people with Opioid Use Disorder (MOUD). 16 Second, providing tele-buprenorphine is consistent with other VHA initiatives, such as the goal of having 20% of Veterans receive telehealth by the end of fiscal year 2018. 17 Finally, tele-prescribing, especially across state lines, is facilitated by the “Anywhere-to-Anywhere” legislation passed by Congress in 2017. 18
The purpose of this project was (1) to develop materials and procedures for the successful dissemination of tele-prescribing MOUD, and (2) to increase tele-prescribing to Veterans with OUD in three targeted rural Community Based Outpatient Clinics (CBOCs). In this paper, we describe our experience piloting tele-buprenorphine to Veterans, experience of non-Veteran stakeholders, and barriers and facilitators to tele-buprenorphine adoption we encountered.
Methods
This project was funded by the VA's Quality Enhancement Research Initiative (QUERI, PII 18-178) in order to operationalize procedures for prescribing MOUD via telemedicine and then pilot a tele-buprenorphine program to Veterans with OUD in three rural CBOCs in the state of Maine. We described the internal and external facilitation that promoted the adoption of tele-buprenorphine at the targeted CBOCs. The implementation of the tele-MOUD program focused on buprenorphine because of its greater acceptability to patients than naltrexone or methadone. The project generating these findings was conceived and conduced as non-research operations activity involving buprenorphine prescribed via telemedicine. Per VHA Program Guide 1200.21, full VA Institutional Review Board review was not required. The project was started in May 2018 and concluded in April 2019.
Hub and spoke model of prescribing
In order to expand services in rural areas, the VHA has funded regional tele-mental health hubs from which prescribers at better-resourced “hub” sites can treat Veterans at distal “spokes,” such as rural CBOCs where there are no local mental health staff. The three CBOCs participating in this pilot had existing face-to-face primary care services along with established telemedicine clinics for all mental health services. At the time this project started, none of the CBOCs had addiction treatment available to Veterans. We used the existing tele-mental health infrastructure at these CBOCs to expand access to MOUD to Veterans living in these rural areas. As carried out, the hub prescriber was responsible for evaluating the patient for appropriateness of tele-buprenorphine, obtaining consent for tele-buprenorphine, prescribing the medication and providing follow-up management. Staff at the spoke sites were responsible for scheduling the tele-buprenorphine session, conducting toxicology testing and obtaining laboratory tests, measuring vital signs, and providing support as needed.
Implementation strategy
Two psychiatrists with expertise in buprenorphine prescribing (DTM and MIR) served as external facilitators on this project. External facilitators visited the CBOCs to explain the tele-prescribing program to key stakeholders. They met separately with facility leadership responsible for providing mental health care, CBOC care, and pharmacy services. They visited two CBOCs and met with staff there to discuss the existing systems for accessing buprenorphine, and how tele-buprenorphine would complement it. Over the course of the study, these facilitators kept leadership apprized of progress, and collaborated with local providers in the existing buprenorphine program.
A nurse (DLW) also served as an external facilitator. After visiting two CBOCs and meeting with local staff, she worked to help troubleshoot issues with implementation, including identifying potential patients, providing coverage when the prescriber was not immediately available, and problem-solving concerns about medication delivery, refills, and the collection of urine toxicology tests.
A psychiatric clinical pharmacy specialist located in Maine (NB) served as an internal facilitator. The internal facilitator visited each of the three targeted CBOCs for meetings with frontline staff and the CBOC managers and provided education about buprenorphine. She also reported progress to hospital leadership. In total, there were three visits to CBOCs by the internal facilitator and four by the external facilitators. Provider logs and VHA centralized databases were used to identify and characterize Veterans receiving MOUD at the targeted clinics. Eligible Veterans were either started on buprenorphine via in-office or home induction methods or were prescribed buprenorphine elsewhere and had their care transferred to a CBOC closer to their homes. (See Table 1 for each participant's type of induction).
Patient results.
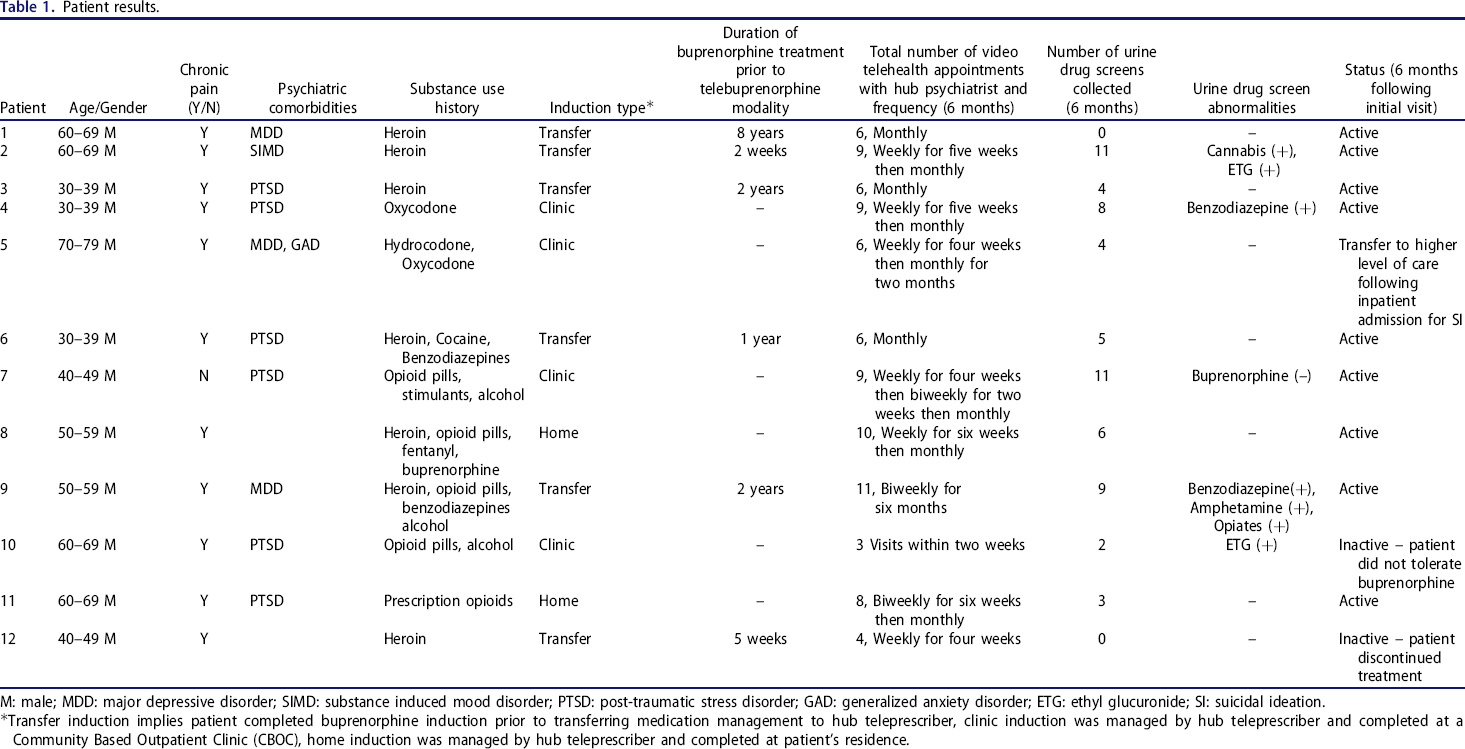
M: male; MDD: major depressive disorder; SIMD: substance induced mood disorder; PTSD: post-traumatic stress disorder; GAD: generalized anxiety disorder; ETG: ethyl glucuronide; SI: suicidal ideation.
Transfer induction implies patient completed buprenorphine induction prior to transferring medication management to hub teleprescriber, clinic induction was managed by hub teleprescriber and completed at a Community Based Outpatient Clinic (CBOC), home induction was managed by hub teleprescriber and completed at patient's residence.
Stakeholder assessment interviews
In order to understand the needs and attitudes of CBOC staff prior to program implementation, qualitative interviews were conducted with physicians, nurses, telemedicine technology technicians, and other CBOC ancillary staff. A semi-structured telephone interview guide was developed by the study team (Supplementary Appendix 1). The interview guide started with general questions about treatment for Veterans with OUD, then transitioned to questions about uses of MOUD, and finally asked about the possibility of tele-buprenorphine. It included inquiries about advantages and disadvantages of having MOUD tele-prescribed. Audio-recordings of all interviews were transcribed and then analyzed using Atlas.ti software. 19 Qualitative data were analyzed using Content Analysis 20 in order to identify barriers and facilitators to tele-prescribing MOUD. Using the constant comparative method, 21 research staff met to discuss and coalesce coding discrepancies, and to compare the variety of perspectives presented by the stakeholders.
Results
Initial phase: Stakeholder interview results – qualitative
A total of 19 interviews were conducted with providers from primary care, psychiatry, nursing, social work, and telemedicine technicians at four separate CBOCs. One of the most significant barriers and negative perceptions about the local, existing MOUD program expressed by staff was the requirement to attend group treatment prior to and after beginning buprenorphine treatment.
Four major themes were identified to describe the barriers and facilitators to a tele-prescribing program: (1) geographic distance, (2) inadequate nursing support, (3) lack of staff buy-in for MOUD, and (4) reservations about tele-health treatment generally. Those barriers and facilitators are briefly described below.
Geographic distance played a major role in Veterans’ ability to access substance abuse treatment in Maine and underscored the importance of establishing a tele-prescribing program. Some Veterans lived more than four hours from the nearest VA facility offering MOUD and found it extremely challenging to attend weekly substance abuse treatment groups. For these Veterans, having the opportunity to receive remote tele-prescribing treatment at a closer CBOC was critical to their ability to continue treatment. One provider explained how challenging it was for Veterans who lived in remote areas to participate in treatment programs: “Some Veterans don't drive, some Veterans have lost their license for one reason or another. Some don't have dependable vehicles. Some travel from, I have Veterans that live off the grid so to speak. They live remotely believe it or not in the woods. So getting here sometimes during the winter is a task in itself for them.”
The second important barrier to establishing a tele-MOUD program was the lack of adequate addiction-treatment-related nursing support and knowledge. Some of the smaller CBOCs had no available staff to monitor a tele-MOUD program. One provider noted: “I think probably just the biggest problem with a Telehealth program like that would be the nursing support and being able to utilize the resources available in the clinic there.” Regarding inadequate MOUD knowledge, another provider said: “I've found that in my position I have to constantly be providing education at different staff meetings, going around the hospital and talking to staff, because of the turnover.”
The third identified major barrier to the implementation of a tele-MOUD program was the lack of staff buy-in and support for offering MOUD treatment to Veterans in the community with OUD (regardless of the delivery method of such a newly proposed service). Many staff members felt ill-prepared regarding their knowledge, experience or ability to care for Veterans with OUD. This suggests ongoing and effective education of the interdisciplinary staff should be made a priority prior to implementing a tele-MOUD program in rural CBOCs.
Lastly, the issue of tele-health more generally was raised. Two providers specifically commented that their patients prefer in-person meeting to remote treatment. One noted: “They don't want to have someone on the screen” and another contrasted tele-health to “real treatment in the community where they can look at each other and have meaningful exchanges and discuss their struggles because they have a lot in common and they don't know it.”
Facilitation efforts–the development of a “how-to” tele-MOUD Toolkit – quantitative
Following qualitative interviews with local staff, the internal and external facilitators outlined a “how to” toolkit to guide the adoption and implementation of tele-prescribing buprenorphine at the targeted CBOCs. The visits conducted by our external facilitators identified issues for inclusion in the toolkit. This tele-MOUD toolkit was further refined by input from subject matter experts, feedback from toolkit users, and review of requests for information about tele-prescribing buprenorphine on the VHA addictions-focused listserv. The toolkit included sample Memoranda of Understanding and Service Use agreements between prescribing hub sites and rural spoke sites, a step-by-step sequence of procedures for beginning tele-buprenorphine prescription, office and home-based buprenorphine induction procedures, progress note templates, resources for other stakeholders and providers (e.g. information for CBOC covering physicians, patients’ family members) and a checklist to delegate who performs what procedure at each site. The toolkit also included extensive sections on legal considerations for tele-prescribing and policies on postal delivery that arose from questions raised on the VHA Addictions listserv.
The most germane information from end-users of the tele-buprenorphine toolkit was about legal issues with tele-buprenorphine. The 2008 Ryan Haight Online Pharmacy Consumer Protection Act, 22 which imposes rules around the prescription of controlled substances like buprenorphine, was not well understood. Other topics requested and covered in the toolkit included guidelines for conducting at-home buprenorphine induction, discipline-specific competencies for tele-prescribing, and regulations for mailing controlled substances. The final product was disseminated to the VA's national substance abuse Sharepoint website and is available for download by users of the VA intranet. (See Supplementary Appendix 2 for a copy of the Toolkit).
Enrollment and retention of veterans into Tele-MOUD
In all, three psychiatrists from the tele-mental health hub were trained and began providing tele-buprenorphine to 12 patients at the three targeted CBOCs in the first 10 months of this project. Veterans diagnosed with OUD were primarily identified for referral for telemedicine mental health and addiction services by local CBOC mental health and primary health care staff.
Table 1 describes the characteristics of the 12 Veterans who received tele-buprenorphine and briefly describes the course of their treatment. Out of the 12, two Veterans were started on buprenorphine via home induction 23 after an evaluation at the local CBOC, four were started via monitored induction at a large central CBOC and six had received MOUD at another facility and were transferred to their local CBOCs after tele-buprenorphine became available. All were males between the ages of 35 and 72, and all struggled with chronic pain conditions. Most had used prescription opioids, over half heroin, and most at least one other substance.
Treatment outcomes are described in the four rightmost columns on Table 1. After induction, four Veterans tested positive for contraindicated substances including stimulants, cannabis, ethyl glucoronide (ethanol metabolite), and benzodiazepines; one tested negative for buprenorphine. By six months after beginning tele-buprenorphine, nine of the twelve Veterans were still receiving tele-buprenorphine. Of the three patients no longer receiving tele-buprenorphine, one discontinued treatment during induction because of nausea, another was transferred to an in-patient facility because he required a higher level of care, and a third discontinued buprenorphine after two weeks.
Mapping of barriers and facilitators to CFIR constructs
The study results were mapped to CFIR constructs 24 as shown in Table 2. Factors that facilitated successful implementation of tele-buprenorphine were its perceived efficacy, customizability, and operationalization in a toolkit. Barriers to tele-buprenorphine included the fact that the program was viewed as a complex intervention and that it was exogenous to the CBOCs core mission. At the outer setting (VHA more broadly), factors that aided the adoption of tele-buprenorphine included VHA including MOUD prescribing as a monitored measure of performance; barriers included CBOC-based personnel feeling separate from outer influence. The inner setting (CBOCs and hubs) facilitated implementation by leveraging existing tele-health structures and relationships; unstable staffing was a substantial barrier and tele-buprenorphine did not bring the CBOCs the more broadly-tasked prescribers they wanted. Regarding the implementation processes, the existence of an implementation plan with QUERI-supported resources facilitated adoption of tele-buprenorphine. 25 , 26
Consolidated framework for implementation research constructs.
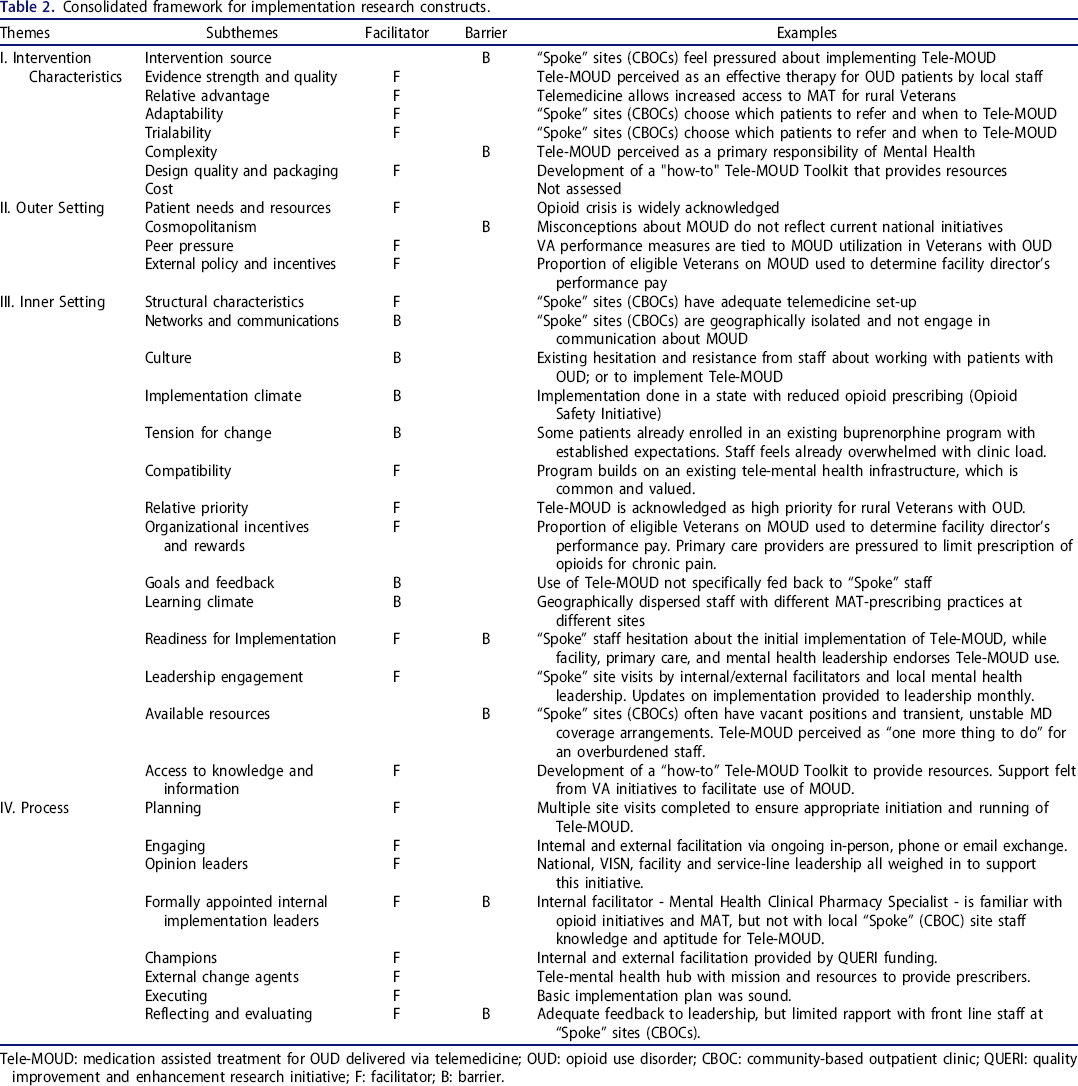
Tele-MOUD: medication assisted treatment for OUD delivered via telemedicine; OUD: opioid use disorder; CBOC: community-based outpatient clinic; QUERI: quality improvement and enhancement research initiative; F: facilitator; B: barrier.
Discussion
In addition to factors that impact telemedicine approaches to addiction treatment more generally, 8 , 10 , 27 we identified factors that were particularly salient for tele-buprenorphine specifically. The opioid crisis, and a near unanimous sense of mission to address the crisis, was a strong motivator for clinic staff. A previous VA-wide initiative to reduce opioid use 28 highlighted the importance of reducing opioid-related morbidity, and tele-prescribing was seen as a continuation of those efforts to reduce opioid misuse by making buprenorphine available. 29
Many of the barriers identified in the CFIR mapping—medical/mental health splits, different incentives in the hub and spokes—can be subsumed under the broad rubric of team integration. These small, primary care-focused CBOCs and centralized hubs serving multiple sites are very different in personnel, staffing, and degree of integration with the rest of the VA healthcare system. Steps to bring these disparate groups together would help with tele-buprenorphine adoption by other hub and spoke pairs. Such steps should include shared programs such as provider education programs 30 and perhaps simply more time for the treaters to become familiar with each other.
The tele-buprenorphine treatment in this project was largely delivered by the prescribers at the hub site, with little of the planning and management by CBOC-based nursing staff that has been described in collaborative care models. 31 The fact that this project was initiated by the hub may have been reflected in many aspects of buprenorphine treatment being delivered by hub-based prescribers. The twelve Veterans treated also reflect the benefits of an integrated treatment system, in that the Veterans were able to move across different CBOC-based tele-buprenorphine services and sites that provide more intensive treatment, depending on the Veterans’ circumstances and location.
The patient enrollment and retention data in this project are consistent with a published report that approximately two thirds of Veterans are on buprenorphine a year after initiation. 32 A review of telemedicine-delivered substance use disorder treatments concluded that such remote treatments are generally well-received and effective. 33 A recent survey of 1294 Veterans given tablets for remotely-delivered care found that 32% preferred video visits, 32% preferred in-person, and 36% said their preference was “about the same.” 34 VA-wide, Veterans treated by prescribers who treat many buprenorphine patients have no worse treatment retention than those treated by low volume prescribers, 35 a finding which also supports the centralized model in our program.
Although data about the extent of tele-prescribing buprenorphine are not available at this time, there have been several initiatives since the completion of this project that have promoted the goals of making care more available to rural Veterans near their homes. 36 The VHA Office of Rural Health funded an initiative to greatly expanded telehealth hubs in each of the 19 administrative regions in the United States in order to improve rural Veterans’ access to care. A large quality improvement project to make MOUD more available to Veterans using implementation/facilitation contains a substantial tele-buprenorphine component with dissemination to other regions of the country.
Expanded telehealth services have gone beyond Clinical Video Teleconferencing at rural VA clinics to VA Video Connect appointments in which a smart-phone or tablet-based app allows Veterans to videoconference with their providers and have virtual visits. 37 VHA mental health providers were mandated to complete at least one such appointment by October 1, 2019. The results of this project elucidate some of the barriers to such an arrangement for prescribing buprenorphine, and how they might be addressed. For example, one important barrier to implementation is the legal requirement for an in-person visit prior to initiating buprenorphine, a requirement that is met by an appointment at a visit between a credential hub provider and a Veteran at a CBOC that has a DEA license. However, there is no guidance suggesting that phone-based appointments qualify and allow for buprenorphine initiation. This project suggests that tele-buprenorphine is facilitated by having a toolkit outlining legal considerations, implementation procedures, and training requirements.
Footnotes
Acknowledgments
The authors acknowledge Jonathan T. Walker, MD, Kevin K. Kruse, MD, Timothy McIntire, MD, Louis Trevisan, MD, Gabriela Garcia Vassallo, MD, Jennifer Bergmann, Psy.D., Staff at the participating CBOCs. The funding organization had no role in the design and conduct of the study; collection; management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication. The views expressed in this article are those of the authors and do not necessarily represent the view of the Department of Veterans Affairs.
Author contributions
Nicole Brunet, PharmD, BCPP. internal facilitator, collection of data, interpretation of results, writing and revisions.
David T. Moore, MD, PhD. external facilitator, provided telemedicine services/buprenorphine to Veterans at spoke sites, project conception and design, interpretation of results, writing, revisions.
Dora Lendvai Wischik, RN, MSN. external facilitator, literature search, writing and revisions.
Kristin M. Mattocks, PhD, MPH. collection, interpretation and analysis of interview data; writing of interview portion of manuscript.
Marc I. Rosen, MD. external facilitator, project coordinator, project conception and design, interpretation of results, analysis, writing, revision.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.