
Abstract
Background
The population of older homeless substance-using adults is growing considerably, and we sought to understand how such individuals gain control of problematic substance use amidst other life problems.
Methods
Data were collected in an NIMH-funded study in which four in-depth interviews were conducted over 18 months with formerly homeless adults living in permanent supportive housing. The study subsample was comprised of 15 predominantly African American individuals over age 45 who were in recovery for at least six months. Cross-case analyses used a template approach followed by inductive sub-theme analyses.
Results
Three themes drawn from the literature yielded seven sub-themes as follows. Theme #1: Acute life stressors: (a) “substance use as primary”; (b) “acute life events and substance use”; (c) “incarceration as turning point.” Theme #2: Attributions of recovery: (a) “quitting as personal decision”; (b) “I just got to stay on top of it”; Theme #3: Social relationships: (a) “I have associates, not friends”; (b) “taking a cautious approach.”
Conclusion
Participants viewed substance use as the primary problem in their lives despite other adversity. Recovery was viewed as a personal decision, but maintaining recovery involved positive social relationships. Policies and practices related to recovery should address the complexities of lives-as-lived.
Introduction
The confluence of three life crises–substance use, serious mental illness, and homelessness–in a person's life can entail years of working toward recovery. 1 , 2 The baby boomer generation has contributed to a pronounced aging of the homeless population and many have longstanding experience living on the streets or in shelters. 3 , 4 Considered to be “old” by age 50, these men and women are survivors who have managed to avoid premature mortality from poor health, drug overdoses, and violence. 4 , 5 At the same time, they face an uncertain future given the toll of cumulative adversity. 2
Previous research on this triply disadvantaged population has shown their life trajectories are marked by introduction to substances in early adolescence followed by early-adult onset of mental illnesses such as schizophrenia or bipolar disorder and, ultimately, homelessness. 5 , 6 In this report, we examine a group of older formerly homeless individuals recently admitted to permanent supportive housing, all of whom had struggled with problematic substance use and had achieved a degree of stability and recovery. We were interested in applying in-depth qualitative case study inquiry into how they gained control over their substance use in their own words, including their causal attributions related to substance use treatment and supportive (or non-supportive) social relationships. With the rapid increases in homeless substance users noted in the baby boom generation, 7 , 8 we believe much can be learned from the experiences of older individuals who have achieved substance use recovery despite life-long adversity.
Aging, substance use, and natural recovery
The possibility of natural recovery without detox and rehabilitation treatment has been noted for decades, 9 – 11 an observation reinforced by the fact that most recovered substance users did not receive formal treatment. 11 Despite (or because of) having few encounters with persons who have naturally recovered, treatment providers have embraced clinical treatment modalities dominated by an abstinence-only approach. 11 Twelve-Step advocates also share in this belief that one cannot control substance use without outside help.
For individuals who use formal treatment for substance use, it is not always possible to discern its influence on recovery given the common pattern of alternating periods of abstinence and relapse. 11 Individuals who ultimately recover on their own may or may not give credit to their earlier treatment. 12 Among the many factors leading to natural recovery, “aging out” was raised early on but “maturing out” more closely approximates how recovery can happen at any age and is often linked to a major life transition such as marriage and parenthood. 1 , 10 , 12 Such changes are not necessarily well-defined turning points or epiphanies. 12 More often, they entail gradual reductions in substance use that only in retrospect assumed finality.
Factors that affect stopping substance use often differ from those that help maintain recovery. 13 Moreover, definitions of “recovery” vary depending upon one's treatment philosophy, with abstinent recovery (AR) distinguished from non-abstinent recovery (NR) where low-risk substance use is included as part of a harm reduction approach. 14 In a study of recovering heroin users, Best et al. 15 found that initial desistance was most often attributed to maturation or “tired of the lifestyle” but maintenance was more a matter of replacing negative social relationships with positive ones. Although averaging 2.6 episodes of formal treatment, the study participants did not attribute their recovery to treatment. 15
In addition to continued mild use of substances, NR may entail methadone maintenance or other form of medically-assisted treatment to control opioid cravings. For alcohol dependence, non-abstinent recovery (NR) refers to controlled drinking whether through treatment or naturally. 1
Almost 20 years ago, Sobell et al. 11 noted that much of what is known about recovery is based upon convenience samples of white, middle-aged males. More recently, Lister et al. 16 have noted the scarcity of literature on recovery among African Americans and other populations. In short, studies that feature self-reports of recovery over the life course remain rare among vulnerable populations.
For both currently and formerly homeless older persons, accelerated aging compresses the timing in their lives as they move through adulthood. 3 These individuals have higher rates of substance use than previous generations. 7 , 8 Permanent supportive housing (PSH) has become a key service component in assisting chronically homeless adults who have histories of substance use. 17 In this context, having recovered from problematic substance use is a positive step forward in allowing PSH providers to focus on health and aging problems. 3
Life course perspectives on substance use recovery
Interest in recovery points to the salience of a life course perspective, as problematic substance use tends to be episodic and can take place over a period of years or decades. 18 , 19 An important factor in the onset and cessation of substance use is the quality of social relationships; there is an abundance of literature linking supportive relationships to substance use recovery outcomes and negative social support to poor outcomes. 10 – 13 Similarly, studies have identified social capital and “recovery capital” as central to substance use deceleration and social losses or depleted social networks as contributing to problematic substance use. 9 , 12
A second life course factor from the literature is the exercise of personal agency. 18 Substance use has often been cast as a poor life choice, with the implication that recovery requires making better choices. Indeed, those who use substances are often the first to self-blame. 19 In contextualizing this tendency toward self-blame, Sampson and Laub 20 refer to “situated choice” to indicate the role of environmental and structural constraints on individual decisions. A third life course factor is the confluence of acute traumatic events with substance use. Such events may be seen both as precipitating use or leading to cessation of use. 21 The sudden loss of a loved one, being victimized by a violent crime, or becoming homeless have all been invoked as precipitants of substance use.
These three factors—acute life stressors, personal agency, and social relationships—form the conceptual framework for this qualitative comparative case study analysis of 15 formerly homeless older adults who have achieved recovery from problematic substance use. Our research questions are:
What are the life experiences and contexts of substance use recovery among older formerly homeless persons? Are acute life stressors cited as contributive? How do these individuals attribute their substance use and recovery vis-à-vis the role of formal treatment vs. natural recovery (personal agency)? What role do social relationships play in recovering from substance use?
By having access to multiple in-depth interviews over an 18-month period with study participants, we seek to maximize understanding of how substance use and ultimate recovery takes place.
Methods
Data for this study were collected as part of a larger NIMH-funded study (2010–2015) among 53 formerly homeless individuals residing in two permanent supportive housing (PSH) programs in a large Northeastern city. Admission to the programs was based upon having a serious mental illness diagnosis (schizophrenia, bipolar disorder, or severe depression) and a history of chronic homelessness. Although eligibility for entry into the PSH programs did not require a history of substance use, all but three of the original study participants self-reported having recovered from problematic substance use during their baseline interview (although some relapsed during the study). As clients in their PSH program, all received case management services as well as program referrals to health, mental health, and substance use treatment as needed. While policies regarding abstinence varied in the two programs (one practicing harm reduction), neither program was abstinence-only in practice and case managers had considerable latitude in addressing their client's substance use.
The parent study design was prospective with four in-depth qualitative interviews (0, 6, 12, and 18 months). All study protocols were approved by the authors’ institutional human subjects committee. We add that this report adhered to the guidelines of the COREQ (Consolidated Criteria for Reporting Qualitative Research) recommended by Tong et al. 22
Sampling and recruitment
The parent study did not require all participants to have a history of substance use but the vast majority of participants had this experience (documented through self-report). Recruitment into the parent study entailed approaching all new program entrants for a period of one year to accrue an adequate sample size (program staff distributed flyers with a toll-free phone number for those interested and eligible). All study participants who contacted the study staff agreed to participate. To enhance confidentiality and rapport, we did not ask program staff to report the number of clients who did not volunteer to join the study. Baseline study interviews took place approximately one month after PSH program entry. Participants had to be over age 18 and English-speaking.
For this study, we selected the sub-sample of all study participants who were over age 45, who had been in recovery from substance use (either AR or NR) at least six months prior to baseline, and who participated in all 18 months of interviews without relapse. Problematic substance use was defined (by the participants) as being in a state of heavy dependency (or addiction) that substantially disrupted their lives. This older-age sub-sample was in line with the study's goal of examining recovery among participants who had lived long enough to “mature out” of substance dependence and/or have a life course of sufficient duration to permit reflecting back on one's substance use experiences.
Data collection
In the parent study, in-depth interviews were conducted by social work doctoral students with professional experience in mental health and substance use treatment. Interviewers were trained in qualitative methods and supervised by the first author, a senior methodologist and principal investigator of the parent study. While the baseline interview tended to last longer to include life history, all interviews focused on a few key domains: histories of mental illness, substance use, homelessness, treatment experiences for these problems, social relationships over the life span, health status, current experiences in their housing program, and thoughts about the future. Interviews, which lasted from 45 minutes to two hours, took place in the participant's apartment or study offices per their choice. In both settings, the interviewer made every effort to ensure the privacy of the participants (e.g., interviews were in private, either in a study office or the participant's apartment). Audio recordings were transcribed verbatim and entered into ATLAS/ti for data management and analyses. In addition to transcripts, data for this report included interviewer-recorded notes made afterward in which they described the participant (demeanor, signs of intoxication if relevant, dress, and personal hygiene) and their apartment and neighborhood surroundings. Finally, the parent study involved detailed case summaries for each participant that were entered into a spreadsheet or matrix. Domains included family ties, history of substance use, psychiatric treatment, incarcerations, job history, homelessness history, etc.
Data analyses
We used case study analyses 23 in three stages. First, we conducted content analysis of participants’ multiple transcripts and case summaries to document all aspects of each person's substance use and substance use recovery. Substance use was defined as regular use of illicit drugs or alcohol beyond brief experimentation. Substance use treatment was defined as undergoing detoxification and/or rehabilitation at a hospital, residential treatment center, or outpatient drug counseling program. Recovery was defined as the complete cessation of drug and alcohol use (AR-abstinent recovery) or deceleration to occasional non-disruptive use (NR-non-abstinent recovery). Following guidelines in the literature, 13 methadone maintenance treatment was considered NR.
The second stage of data analyses followed a “template” approach 24 in which previously identified themes from the literature were applied to the substance use case files. For our purposes, three categories previously discussed as conceptual frames for understanding substance abuse recovery–social relationships, attributions of recovery/personal agency, and acute life stressors—were used to organize and retrieve relevant data across the cases. 24 The aggregated data were entered into Dedoose software for further analyses. To accomplish this, two members of the research team read all participants’ interview transcripts and identified portions in which they describe their social relationships and life stressors as related to the onset and cessation of substance use and statements regarding their attributions of recovery (particularly the role, if any, of formal treatment, personal agency—or a combination of both). All excerpts from interviews were identified by the participant's ID number and timing of interview (baseline, 6-month, 12-month or 18-month interview).
Next, three members of the research team (the co-authors) independently read the three large cross-case files (ranging from 45 to 60 pages each) as part of inductive analyses 24 to identify sub-themes for each of the three dimensions. Memo-writing was used to note meaningful patterns and repeated consensual discussions were held to reach agreement on sub-themes. Our over-arching goal was to understand the life course contexts of substance use recovery. While the themes were pre-identified (via a “template approach”), the content and labeling of the sub-themes were inductively guided by the principle of saturation commonly used in qualitative inductive inquiry. 25 Thus, sub-theme development ended when independent readings revealed no new sub-themes.
Results
A total of 15 individuals met the inclusion criteria. The sample was predominantly male (80%), overwhelmingly Black (14 of 15), and ranged in age from 45 to 63. Two-thirds (n = 10) did not finish high school or its equivalent (GED degree) and two-thirds had children, with a range of 1 to 5 offspring. Age of onset of substance use ranged from 7 to 31 years. Alcohol and crack were the most commonly used substances followed by marijuana and powder cocaine (only three individuals abused a single substance).
Almost half (n = 7) had undergone one or more episodes of substance use treatment (see Table 1). Eight participants were in abstinence recovery (AR) and seven in non-abstinence recovery (NR), of whom five were on methadone maintenance (the other NR participants reported sporadic use of marijuana or alcohol). For 13 of the 15 participants, recovery from substance use occurred after age 30. The period of time post-recovery at the baseline interview ranged from 8 months to 32 years.
Substance treatment and recovery status of study participants.
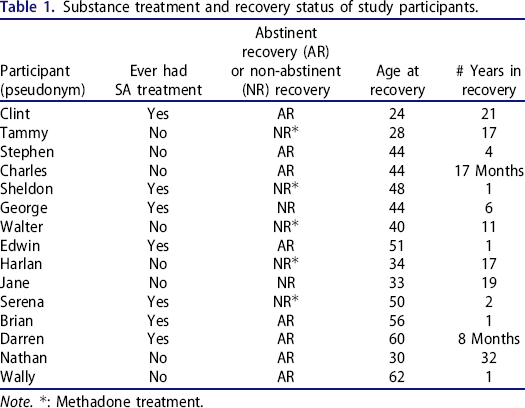
Note.: Methadone treatment.
Themes and sub-themes
Theme #1: Acute life stressors
Inductive cross-case analyses revealed three sub-themes: the primacy of substance use as a life stressor (amidst other stressors), the confluence of acute events related to substance use, and incarceration as a positive turning point.
Substance use as primary
Despite having struggled with serious mental illness, homelessness, and other adversity, participants referred to their substance use as pivotal in negatively affecting their lives. Dropping out of school, incarceration, failed relationships, and absentee parenthood were closely linked to drug and alcohol abuse, to crimes committed to sustain their habit, and to the consequences of being high. Edwin said that before he got involved with drugs, “I basically did the right thing….it [drug use] affected me till this day, as far as me turning my life into what it is now, being homeless, and being an addict.” Edwin left home at age 16 to live with his son's mother …. “and then I started getting into drugs. And …that's what messed everything up, once I started getting into drugs.”
Charles recalls missed opportunities, “I probably would have a good job right now… I wasted a lot of years. I could have finished school. I could have did a lot of things.” Charles spoke of his ex-girlfriend as joining him in letting their drug use take over, “when you be with somebody for so long that's all you did was drugs, drugs, drugs.”
Stephen talks about how “…the drugs took over. Got on welfare. You know, drugs, welfare, drugs, welfare, drugs, welfare. That's how I kept living all that time.” Serena notes that she lost custody of her children, “… because of my drug use, you know what I'm saying?” Clint describes how long his recovery lasted after an intense period of addiction,
The confluence of acute events and substance use
In reviewing participants’ life stories, we were struck by the negative synergy of acute life crises related to substance use. Nathan, for example, was convicted of murdering his wife while high on heroin and she was high on crack. Not long after his release from prison, Nathan pled guilty to the attempted murder of his father during an argument over whether he would be allowed to see his children. Walter was convicted of murder after stabbing someone at an early age, “I started getting high at the age of twelve, my first drink, my first joint, my first murder case.”
Stephen was arrested and later incarcerated for assaulting his girlfriend while both were drunk.
… then I told her, “Get out. I don't want you here.” So she wouldn't leave. And I grabbed her, physically grabbed her and pushed her out, and got a little rough. She called the cops, got me locked up for assault and robbery. So that's what I did three years for.
Brian was sent away by his parents to live with relatives after being blamed for his younger brother's death; the toddler fell off the building's roof while they were playing. Brian blamed himself for not watching the boy as he was instructed and attributed his depression and heavy drinking to this tragic accident. Visiting relatives in the South, he hoped to cut back but found it even harder:
I was drunk every day….And actually I wanted to go down there….I said ‘OK I will go down south, maybe because in New York, I can get out of here and calm down the drinking.’ That was a paradise for an alcoholic. People made their own booze, so, look I drunk everyday up until I left [to return to New York]. Never was sick. But nobody asked me, knew that I was drinking.
Harlan was paralyzed by a severe fall while working on a construction site. While able to recover the use of his legs, he was eventually denied painkillers by his physician and transitioned to heroin use before finally turning to methadone. Marital strife during this period led to his divorce. The downward spiral of the construction accident then addiction was illuminated when he said, “I lost everything. Wife, kids, everything…”
Incarceration as turning point
Several participants were candid in discussing the role of incarceration in their recovery. Serena stated, “I stopped going to jail. I stopped stealing. Cuz I was stealing to support a drug habit. … and I got tired of going to jail.” Wally reported that he got sober in prison and stayed sober upon release to avoid going back. Jane reported that she stopped her heavy use of marijuana while in prison for armed robbery. Wally convinced a judge that he needed drug treatment, not incarceration, saying,
I ended up getting sober because I had enough of it, you know? … I was in jail…parole violation, and the judge he wanted to give me a maximum time,… but I told him that you all keep lockin’ me up but you know I have a drug problem and you know I need help. So, they said they'd find a program for me… but somebody would have to take me because I'm on parole, and they found this program for me.
Prison also afforded positive opportunities—to earn a high school equivalency degree, get job training, and earn college credits. Tammy got her first job while on work release and Serena took college courses in prison, saying “I finished high school…. I took college up state [in prison], I had 12 college credits.”
Sheldon related how repeated jail stays over minor drug offenses took their toll. “Police know you so much they keep locking you up. You ain't got to have nothing on you. Criminal possession in the fifth degree, means that you had some paraphernalia somewhere… like a stem or a piece of plastic… And you just go through the system again.” At the time of the study interview, Sheldon was proud to have this all behind him. “I don't even remember last time I was there [jail]. I know I ain't trying to go back no more. I ain't got nothing open, … I can walk the street with my head up.”
Theme #2: Attributions of recovery and the role of personal agency
Perhaps not surprisingly, participants’ attributions about what led them to quit differed from their strategies for maintaining recovery. Yet the exercise of agency was readily apparent in their stories of quitting as well as in how they maintained their recovery. Below are the two sub-themes that characterize this distinction.
Quitting as personal decision
Whether quitting was a sudden stoppage or a tapering down process (with or without methadone maintenance), this pivotal change was portrayed as a deeply personal decision. Such a decision did not preclude the influence of extant circumstances, e.g., a doctor's warning of cardiac arrest if crack smoking continued. Even if incarcerated, participants believed they had a choice since contraband drugs were frequently available. Stephen explained his thought process:
… when I was in there [prison] I was offered drugs, and I was actually using and all that, but I said, no, I don't wanna use drugs. Not in here, you know, it's not even worth it. You know, ‘cause they take urine test, that's all I need to take a urine test and have more time on my hands. So, I decided, you know, tell them, no, I don't want it.
Similar to Stephen, Serena described that not wanting to return to jail, particularly at her age, was a motivation to stop:
I got tired of the going to jail, losing all my belongings, having to start all over you know?… And that was it. I said, ‘You know what, I am too old for this. I am 50 years old. This is embarrassing’.
As importantly, quitting was not attributed to treatment either directly or indirectly. George stated:
I got tired of going to detox and rehabs and shit, ‘cause I wasn't gonna stop. So, listen, when I stopped this time, I didn't go nowhere. I didn't go to no detox; I didn't go to no rehab. I just took the [crack pipe] stem, wrapped it up in some tissue and I stomped it. And I just fought it. I cold-turkeyed it.
Sheldon said he just “needed to show myself I could do it.” He explained,
I am the biggest change because, I think about the getting high, but I don't do it. You know, I look back at what I used to do, I was bouncing around from this house to that house, my ass would run the street 3 or 4 o'clock in the morning, you know. Sit around hang out on the corner with the guys you know, drink beers and stuff like that…but I don't need to do the things I was doing just to sit on the stoop and stuff like that.
Darren, who had been clean for eight months, noted, “I stopped using and I decided to leave it alone. Because it wasn't helping me, it wasn't helping my psychiatric problems either, so I left it alone.” When asked how he managed to stop, Darren answered:
I just got tired of them, tired of it. And mostly—that's a small world by itself. A lot of people mess with drugs, but there's still a lot of people that's sober. And I liked it that—it feels much better being sober… I don't go back into the same path with the same type of people, so that's what made me stop.
Tammy used heroin and methadone for six years. “I just stopped cold turkey…I first started; I was like 17. I stopped when I was 23… who the fuck wanna be on methadone all they life? Like get outta here, it's not gonna be me.”
“I just got to stay on top of it”
Some participants were years past their heaviest periods of substance use, others were relatively new to their recovery. As mentioned earlier, study participants were almost equally divided between AR and NR (most of the latter on methadone maintenance and not using other drugs or alcohol). Regardless of status (AR or NR), participants expressed cautious optimism about maintaining their recovery. We found three basic strategies used to pursue this: (1) formal supports (e.g., 12-Step groups and religious faith); (2) pro-active avoidance of “people, places, and things”; and, (3) weighing the negative consequences of relapse. Serena stated, “… I went to a couple of NA meetings… helped a lot, but it was basically more up to me and continued prayer and that's what helped me stay positive.”
Charles explained the challenges of keeping clean:
… you know, I was a drug addict at one time, and I got 17 months clean. Cause if you're an addict and you go around the same area you used to get high at, the feelings got to come up. Its gotta come up. You might run into an old buddy of yours you used to get high with. You cannot tell me that feelings not going to come up.
Charles looked to AA and NA to work through tough times, “…now I talk about it. I got to NA, AA, any type of meeting I go to I talk about it. Or I call my sponsor…” Charles also described his intentional avoidance of places where people may be using drugs saying, “So, I don't even go that route. Because over there is like a methadone program, so now the whole area is drug addicts… So, I don't even go that route, I don't even go that way at all.”
Harlan moved to an adjacent state to distance himself from temptation: “AA, NA. You know, one of the things they say that you got to change people, places, and things. That's what basically I did.” Harlan's use of methadone maintenance was a positive step for him:
It's been a long process but, you know, I've been dealing with the methadone maintenance program for quite some time now, and I'm doing real good in there, you know… things starting to look up for me.
Jane stays away from a neighboring borough, saying “I went there, didn't like it. I was a crack head down there.” George spoke about how difficult it was to use certain subway stations where he risked running into the wrong crowd, “It ain't the point about me being scared to get high, ‘cause that's furthest thing from my mind. I just… don't want [to see] them…”
Weighing consequences were also salient through pondering the benefits of sobriety. Darren states, “…it feels much better being sober. You know, I keep more money in my pocket, and I don't go back into the same path with the same type of people.” He added, “… I don't touch that anymore. Because it's not going to help me, it just stressed me out and made my mental problems get worser [sic].” Edwin saw only negative consequences of resuming substance use, “I could have a heart attack, I can get busted buying it. Something might happen where it'll get me into some kind of trouble.” Serena considers the alternative situation by saying, “I won't pick up and use because that's not gonna make the situation better, and it's not good for me.”
Theme #3: Social relationships in drug use and recovery
In general, the use of drugs began in early to late adolescence. This earlier life timing points to the potential influence of relatives and neighbors as well as peers. However, participants focused on their current situation and how social relationships might help or hinder their recovery. In this regard, we identified two sub-themes described below.
“I have associates, not friends”
This sub-theme echoes 12-Step lingo labeling fellow users as associates, not friends. As such it refers to the general absence of trusted relationships in their lives. Serena explained the limitations of her new relationships, saying, “…no I don't have any friends. People I know. Associates. People I know, I speak to.” Nathan said, “No, no friends. Not yet…I'm not letting any new friends in until I'm off parole.” Similarly, Sheldon steered clear of his roommate, saying, “You know, people get too comfortable with you at times. You know, so I'm not trying to get comfortable with nobody no more.” Wally referred to his reliance on service providers, “The friends, I really call ‘em associates… they good to have, to talk to… these are mostly my [case] workers at [program]… and my psychiatrist.”
Darren preferred to avoid people since he was temporarily housed and did not want others to know about his past:
No, I don't talk to the neighbors. That's just living my, life by my own self, you know. I don't want to make friends… I'm not gonna be there that long, so I don't want to really get acquainted with people, you know. Because then they find out my situation, they'll try to make things bad for me maybe.
Taking a cautious approach
This second sub-theme covers the various strategies taken by participants to re-connect with non-using family and friends and forge new relationships with caution given previous negative experiences. Brian describes the challenges of associating with family members who are still using:
I would've left them alone if they were friends. They are relatives…They ain't nothing but a bunch of trouble…They are smoking marijuana… So, that's another reason I haven't been around there for a while. When I see them, on the streets. I can't go to their house ‘cause they use drugs. See, certain people I can't be around—like I got brothers, I know where they are…there's one standing on the corner right now. I don't associate with them because they're using drugs. I can't be around people.
In contrast, Nathan talks about wanting to reconcile with his adult son, but it is “really kind of a delicate situation” because he was convicted of murdering his son's mother. Nathan was still on parole and concentrated on his church activities:
I'm careful who I socialize with… And that's deliberate… People speak to me. They want to be friendly, in the neighborhood. …I just say hello, good morning, good evening, I'll pray for you, they see me going into the church, the [Jehovah's Witness] hall. And ah, I do that intentionally because they, like I said, they drink alcohol or they smoke marijuana at the minimum. It's probably other stuff they do, but those are the two things that I know they do. I cannot be around that.
Charles mentions his hesitation with making friends at NA meetings:
I don't go there to show off and all that. I go there to hear the message and then I leave. You know, I probably made a couple of friends and get a phone number here and there but that's it.
Charles attributes his reluctance to developing friendships as a way to maintain sobriety, explaining, “You know… I am a relapser. It's easy for me to get high, so I try to um, stay away from certain people.” Serena's caution extended to any potential visitors, “… if anybody's using drugs, and they're still stealing, they ain't coming in my house.”
Sheldon was making careful outreach to non-using relatives and friends to let them know he was in recovery and could be trusted:
I am being a little more particular about the people I am around…my daughter is more around. And stuff like that. You know, a lot of people I used to know when I used to get high and stuff, I come around now and there is a big difference to them, you know it's a big difference because they are giving me a little more space than they did before. So they trust you more and things like that. You know, so when it comes like for me to go places with them, they ain't mind, they can lay their bag down stuff like that. They know ain't nothing going to happen to it [the bag].
Serena appreciated the benefits of her recovery but did not take them for granted:
You know, I wasn't happy. I didn't have my children…, but now that they are in my life, and my sister and I have gotten much closer. All of that came good to me from my stop using drugs… So, I'm happy with that part–I pray on picking back up, you know, but so far so good. I'm taking one day at a time. I don't drink or do nothing. I just smoke cigarettes.
Harlan wondered aloud if he had been a bit overly cautious: “I was getting antisocial for a while and alienating myself… my main thing was to change people, places and things, and I did that. You know, maybe too well.”
As can be seen in the inductively derived sub-themes in these findings, the effects of acute life stressors –including problematic drug use– did not prevent participants from exercising personal agency in deciding to quit. Yet their hard-won success was tempered by a cautious reliance on others to assist them in maintaining their recovery.
Discussion
The individuals in this study entered middle age after years of struggling with substance use, mental illness, and homelessness. Yet they were survivors nonetheless and showed resilience in achieving their recovery. Living in permanent supportive housing offered a degree of stability to enhance that trajectory. However, by the time participants achieved recovery, they still had to reckon with an uncertain future including accelerated aging. The literature on recovery has highlighted the significance of human and “recovery” capital. 12 Given their cumulative life adversity, it is all the more remarkable that study participants were able to achieve recovery in relative social isolation and that formal treatment was missing from their accounts of quitting. Although five participants were on methadone maintenance and thus technically “in treatment,” they viewed themselves as in recovery in that their lives were no longer seriously disrupted and their meager income no longer expended on drugs. This is consistent with previous research valuing the significance of subjective appraisals as well as clinical diagnoses. 6 , 19
Motivations for quitting could be specific, e.g., a doctor's warning, or vague, e.g., tired of the negative consequences, but all were couched in terms of a personal decision. Worries about health and aging, combined with the desire to save money to spend on family or leisure, helped tip the balance toward sobriety and abstinence.
In contrast, maintenance of recovery was heavily influenced by social factors, both through positive ties (12-step sponsors, faith-based organizations, non-using friends and family) and avoidance of people and places that might lead to relapse (the latter a common directive of 12-step groups). Similar to research on post-recovery experiences of re-defining a negative identity, 15 , 19 participants acknowledged the challenges even as they sought a more positive sense of self.
This study represents a relatively rare glimpse into the lives of older predominantly African American individuals engaged in overcoming years of adversity and problematic substance use. That all attributed their recovery to personal decision-making and contextual circumstances rather than formal treatment reifies a “natural” aspect to quitting combined with external-support mechanisms for maintenance. Previous studies of African Americans and drug addiction have noted barriers to recovery emanating from proximal factors, e.g., lack of access to treatment. 16 The social and structural contexts of the lives of our participants point to multi-faceted approaches to treatment including assisting in natural recovery while taking into account the likelihood that social support will be limited in availability.
Implications for treatment point to the significance of the interplay of complex problems surrounding substance use. Treatment practices and service systems established for mental illness and substance use continue to lack integration and, despite recognition of “dual diagnoses,” 5 , 6 , 26 philosophies of treatment are frequently at odds. A strict abstinence approach enforced without recognition of psychiatric symptoms or the lingering traumas from living on the street—where there is ready availability of drugs and alcohol—risks failure. While recommending better integration of services and assisting clients with “natural” recovery are suggested by this study's findings, we would also urge greater attention to previous traumatic events that can complicate well-intentioned efforts to assist in recovery.
Limitations and strengths
It is plausible that social desirability skewed participants’ accounts in a positive direction or led them to over- or under-state events in their lives. To this we counter in two ways. First, given the vivid unvarnished accounts offered, it is difficult to imagine that important information was left out or altered to save face. Second, respondent biases tend to fade over time during prolonged engagement, 24 i.e., participants were enrolled in the study for 18 months. In this regard, the sample size of 15 must be placed in the context of the depth of information obtained from multiple interviews with each participant with whom rapport has developed over time. Such depth requires greater immersion to reach saturation but also significantly enhances data adequacy. 25 and trustworthiness. We acknowledge that self-selection in the parent study may have produced some bias as we did not have information on non-participants.
Our qualitative emphasis on subjective portrayals omitted strictly defining substance use and instead relied on participants’ descriptions of their substance use, the damage it caused in their lives, and their personal recovery stories. Future research with larger samples and mixed methods could more closely track a variety of factors proximal to recovery and maintenance.
Strengths of this study include, as mentioned above, the depth and breadth of data available. We also note the use of independent then consensual thematic analyses to minimize bias. Finally, this study examined the recovery trajectories of an understudied group–older predominantly African American men and women.
In conclusion, this study contributes to a broader and deeper understanding of the lives of older formerly homeless individuals who achieved substance use recovery in spite of extreme adversity. For them, recovery was a personal decision made while contending with mental illness, homelessness, incarceration, and resultant losses in social and human capital. As survivors, they nonetheless faced challenges of maintaining their recovery, pursuing positive social ties and the prospect of premature aging. As the number of older homeless Americans rises dramatically in the United States, 3 , 7 , 8 policies and practices related to recovery should address the complexities of their lives-as-lived.
Footnotes
Acknowledgments
The authors wish to express their appreciation to the study participants for sharing their life stories.
Author contributions
Deborah Padgett: Conceptualized the study, conducted data analysis, and wrote the manuscript. Kristen Gurdak and Lynden Bond: Conducted data analysis, produced tables and references, contributed to the study's findings, and edited the manuscript.
Disclosure statement
No potential conflict of interest was reported by the author(s).