
Abstract
Background
Hub and spoke systems (HSS) are increasingly promoted as a systems-level intervention to expand access to medication for opioid use disorders (MOUD), particularly in rural areas with limited treatment options. The HSS model consists of sub-systems in which “hubs” deliver specialized expertise to a regional network of office-based opioid treatment (OBOT) providers in “spokes,” who together create a continuum of acute and chronic care. Yet, little is known about system-level factors (e.g., system structure, financing) that influence HSS implementation and sustainability in rural areas.
Methods
For this case study, we conducted semi-structured interviews with substance use disorder treatment providers (N = 26) and system-level stakeholders (N = 16) in five rural HSS sub-systems throughout one state. We undertook iterative textual analysis of interview transcripts, identifying and coding themes related to key implementation constructs associated with the Exploration, Preparation, Implementation and Sustainability (EPIS) framework.
Results
California policy-makers adopted HSS to expand rural access to opioid treatment programs (OTPs, i.e., providers of methadone and other medications for opioid use disorder). However, stakeholders questioned the model's fit for rural regions featuring few established OTPs that could function as hubs and critiqued its treatment-focused approach, felt to sideline harm reduction service providers. Contracts to serve rural regions were awarded entirely to for-profit methadone providers, contributing to stigma and distrust among many buprenorphine providers whose organizations were later recruited as spokes. While hubs offered financial resources enabling some spokes to expand MOUD, the needs of spokes varied considerably. Relationships between hubs and spokes to facilitate the care continuum under HSS were restricted by limited behavioral health resources and the large distances characterizing rural California.
Conclusions
This case study reveals how rural contextual factors such as geography and behavioral healthcare resource availability can dramatically influence differential HSS implementation.
Keywords
Introduction
An estimated 2 million Americans suffer from opioid use disorders (OUD). 1 While some studies show equal prevalence of OUDs in rural and urban areas, rural residents face unique challenges in accessing treatment and support. 2 Rural residents must travel longer distances to access medication for OUD (MOUD)—whether buprenorphine or methadone—and face fewer options for care. 3 – 6 Since prescribing buprenorphine requires a waiver from the federal Drug Enforcement Administration (“X-waiver”), recent initiatives to increase the availability of waivered providers have exerted dramatic impacts in non-metropolitan areas. 7 Yet logistical barriers often stymie rural providers from offering MOUD. 8
Hub and spoke systems (HSS) to deliver MOUD are widely celebrated as an integrated, systemic approach to combat the opioid epidemic particularly in rural areas hard hit by OUD but lacking treatment options. 9 – 11 Policy-makers in the U.S. state of Vermont developed HSS to enhance support for community-based primary care providers offering MOUD. 9 HSS are premised on a stepped-care approach, employing assessments to place patients in hubs for acute care or spokes for less complex addiction issues, and facilitating movement to locations more proximal to a patient's residence when needs change. As shown in Figure 1, hubs in Vermont consist of a opioid treatment program (OTP) with capacity to provide methadone and buprenorphine treatment, assess patient needs, and determine a plan for care, including transfer of patients to chronic care in spokes providing MOUD likely closer to their homes. 9 Hubs employ interdisciplinary “MAT teams” to support spokes in establishing the clinical, and logistical tasks necessary to establish primary care-based MOUD, particularly in rural practices with less capacity. 9 HSS consist of smaller “sub-systems” in which a given hub is connected to multiple spokes.
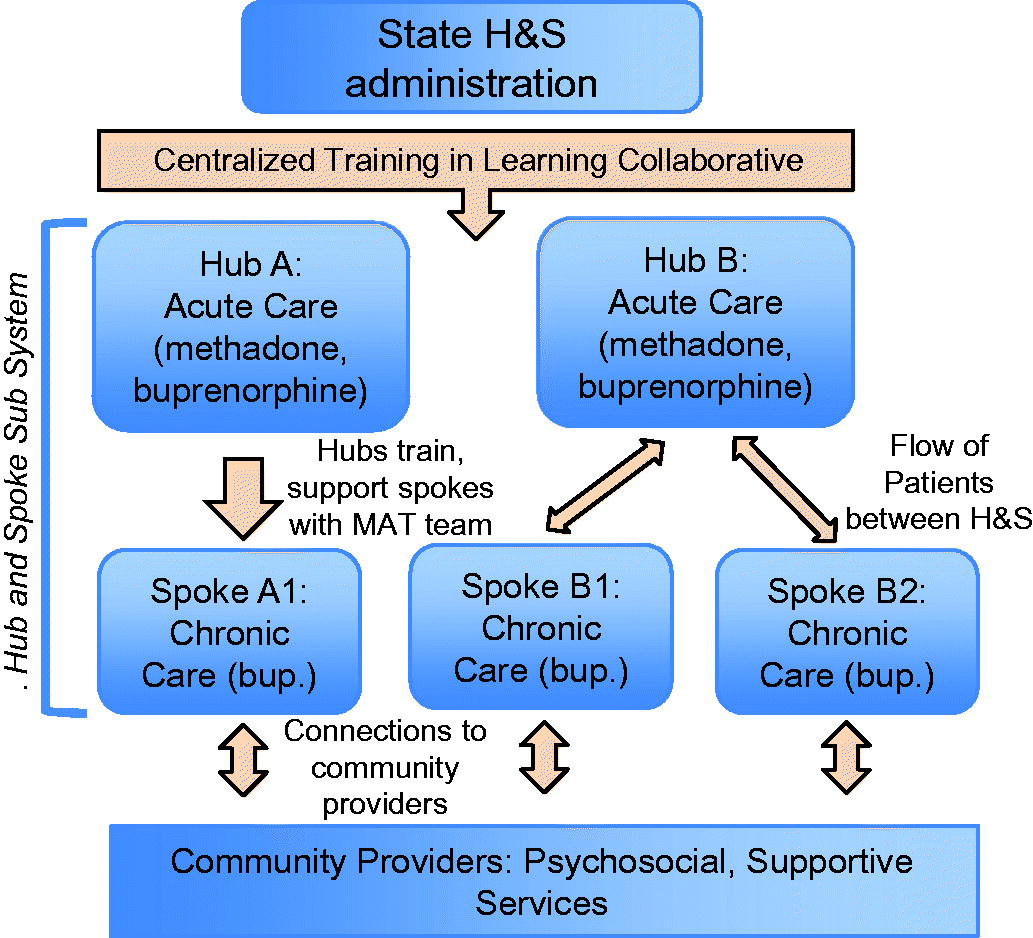
The Hub and Spoke intervention consists of inter-connected hub and spoke sub-systems. Peach colored arrows represent H&S components. Adapted from Rawson 2017:22.
In Vermont, implementation of HSS led to reductions in patients’ opioid use, days of injection, other substance use, overdose, and ED visits. 9 , 12 , 13 HSS improved access to MOUD by expanding treatment capacity, increasing waivered MOUD providers, and decreasing wait lists at hubs. 9 , 12 , 13 Still, evidence from the Vermont HSS shows varied access to sub-systems, inadequate linkages to mental health services, and insufficient procedures to place patients on the care continuum. 12 , 13 As the model has been adopted in five other U.S. states with new federal funding opportunities, components have been adapted, changing the composition of hub and spoke networks, mechanisms to coordinate care, and delivery of technical assistance. 14 – 17
The present study examined implementation factors making treatment more accessible and sustainable for participating rural organizations in California's HSS. The study contributes more evidence of how states have implemented this system-wide intervention to expand MOUD capacity. The accelerated adoption of HSS was instigated in part by the Substance Abuse and Mental Health Services Administration's Opioid State Targeted Response (STR) Grants program, created through the 21st Century Cures Act. Of all states implementing HSS through this program, California's is the largest in terms of financial investment ($90 million compared to $4–24 million in other states). Ongoing research on statewide implementation of HSS focuses primarily on patient outcomes and adoption of MOUD. 9 , 14 , 18 , 19 Studies have yet to assess system-level factors vital to implementing and sustaining HSS, including financing, system design, and contracting. The implementation science literature demonstrates that such factors are critical to the accessibility of evidence-based interventions. 20 , 21 Our study examines how system-level factors impacted stages of planning, implementation, and future sustainment of HSS in California, a large state system encompassing diverse rural settings.
Methods
We employed an explanatory case study design to examine how the contextual conditions and processes of HSS implementation impact the program's effects. 22 We defined the case as the state-wide implementation of HSS in California and compared sub-systems within (see Figure 1) that included at least two rural spokes. We employ the Exploration Preparation Implementation and Sustainment Model (EPIS) 23 from implementation science to guide our exploration of the system-level factors influencing the implementation process in the rural portions of the California HSS, with attention to how HSS was adapted in each sub-system. Our Appendix describes how data was collected in accordance with the Consolidated Criteria for Reporting Qualitative Research. 24
Study site
Seven of California's 19 sub-systems at the time of study included at least two spokes serving predominantly rural populations across coastal and inland Northern California and in the rural agricultural Central Valley. We define as rural those sites labeled with United States Department of Agriculture “non-metro” rural-urban continuum codes four to ten. 25 California has a relatively low statewide prevalence of OUD and fatal overdose, though several of its rural regions have prevalence estimates comparable to the highest need areas in the U.S. 26
Recruitment and sample
Halfway through the two-year funding period of the HSS roll-out, we recruited two groups of participants across five rural sub-systems: (1) treatment providers (N = 26) from five sub-systems in California serving predominantly rural populations and (2) system-level stakeholders (N = 16) including administrators from providing sites, harm reduction advocates and service providers in rural communities, and public health officials. Table 1 illustrates the range of providers involved in care for MOUD patients in rural spokes that we sampled, consistent with sampling techniques in implementation science focused on breadth. 27 While hub providers were contacted repeatedly, we faced challenges in recruiting them. However, we increased credibility by including multiple sub-systems 22 and purposively sampling within each. We identified potential participants using public data on hubs and spokes, employing snowball recruitment to identify additional participants in each sub-system. All participants provided written informed consent and were offered $50 gift cards for taking part. The University of California, Berkeley Institutional Review Board approved this study.
Participant characteristics.
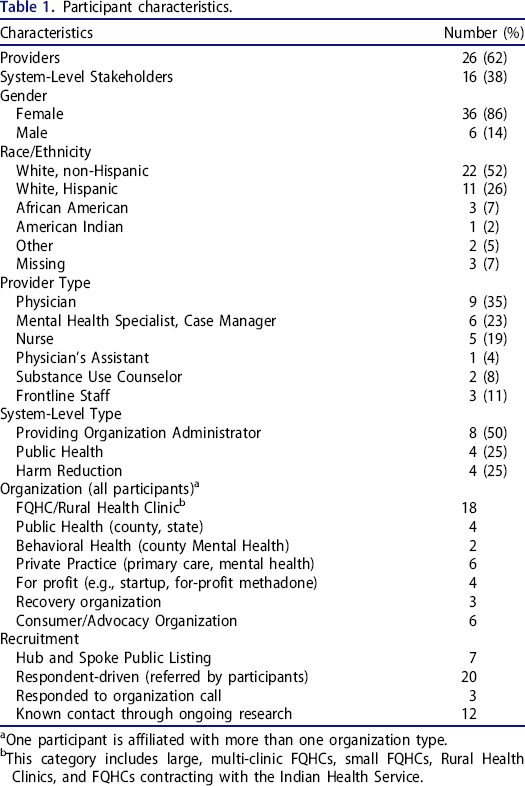
One participant is affiliated with more than one organization type.
This category includes large, multi-clinic FQHCs, small FQHCs, Rural Health Clinics, and FQHCs contracting with the Indian Health Service.
Data collection
Our interview guide included questions to examine HSS implementation in rural California and rural treatment options. Semi-structured interviews between July 2018 and January 2019 focused on (a) outreach and retention challenges for rural patients; (b) implementation strategies–systematic processes, activities, and resources for integrating innovations into care settings–to meet patient needs; (c) factors affecting provision of MOUD unique to rural settings; and (d) anticipated barriers and facilitators to sustainment.
Data analysis
All interviews were audio-recorded, transcribed, and entered into Dedoose qualitative data analysis software. 28 Guided by thematic analysis methodology, 29 in the first reading of the transcripts, the first author identified preliminary analytic categories from our implementation science framework (e.g., inter-organizational relationships) and inductive constructs emerging from the data (e.g., patient-provider interaction in rural settings). The research team defined codes with exemplars and exceptions and affixed codes to the text through line-by-line coding. Throughout coding, memos were used to refine code definitions and reflect on code relationships.
Results
We have organized our findings around the system-level factors relevant to different stages of implementation, as laid out in the EPIS framework. 23 In Figure 2, we summarize our overall findings.
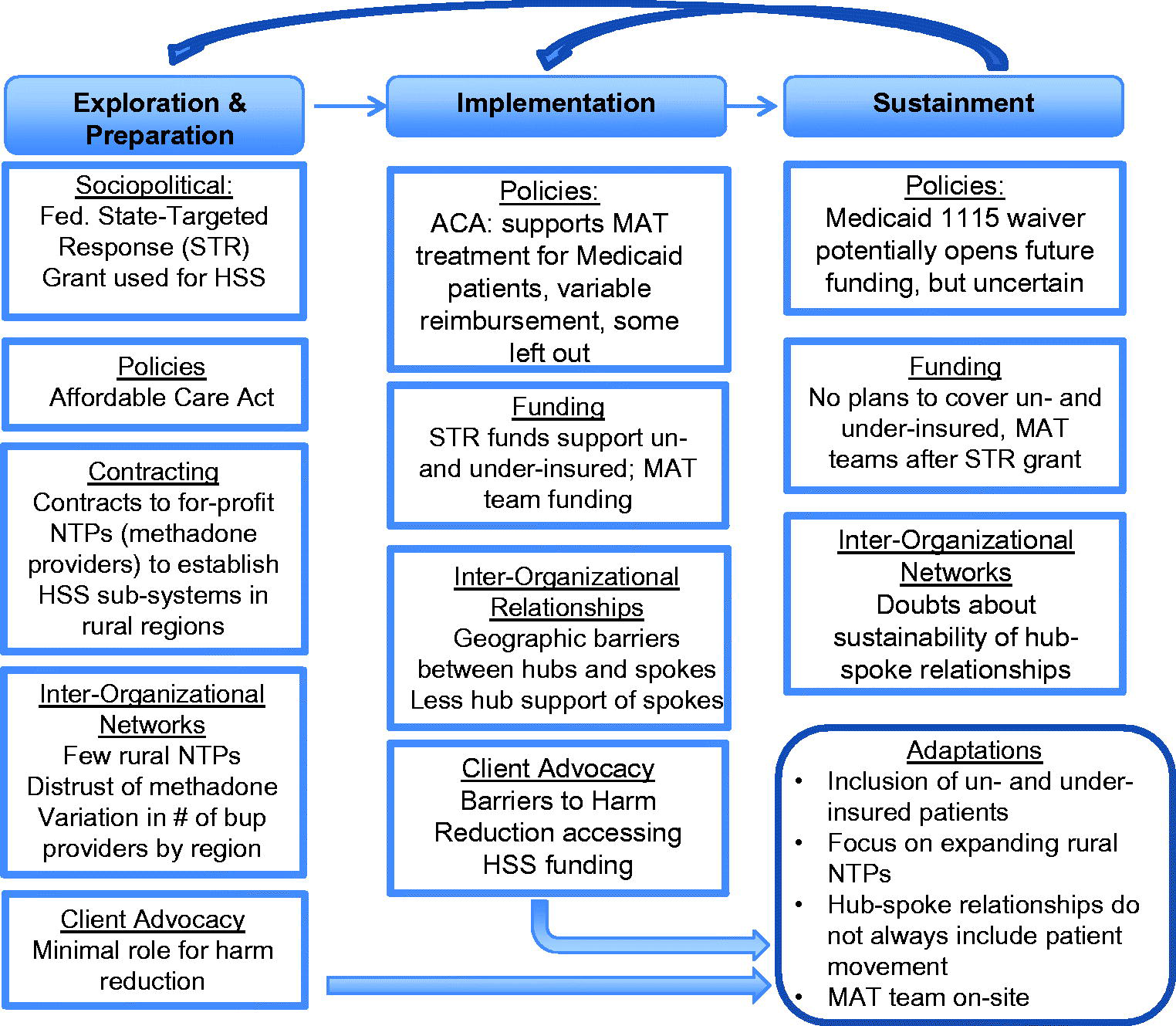
Summary of Results. Systems-level factors during the exploration & preparation phase that impacted the implementation and sustainment of California's HSS in rural regions led to a number of adaptations to the initial HSS from Vermont. Adapted from Aarons et al. 2012.
Exploration and preparation
Sociopolitical
A state policy-maker explained that when funding through STR grants became available, they opted for HSS because of its capacity to build support for spokes and to address rural disparities in access to OTPs, considering that none of the rural counties with the highest opioid overdose death rates had an OTP. From the outset, there was an understanding that inter-organizational HSS relationships would be adapted to California's unique context. California policy-makers anticipated that hubs would offer expertise to spoke providers and manage the most complex patients regionally, while spoke providers would offer buprenorphine-based treatment to less complex patients in primary care settings.
While several providers affirmed the model, they questioned its fit for California's diverse geographic mix of mountains, forests, plains, and deserts, and its varied practitioner landscape. One program coordinator commented, “[HSS] was a great idea…But when you compare the size of the states that we pulled from, it makes no sense.” Harm reduction advocates pointed to the distance between spokes and the populations they serve, many of whom are, out of necessity, served indirectly through peer networks (e.g., for syringe access and disposal services) due to physical and social barriers. These extremely high-need populations, argued advocates, were not well-served by a model that concentrated resources in larger towns.
Policies
Participants explained that California required all HSS providers to be Medicaid eligible to cover treatment costs. However, policy-makers elected to apply STR funding to also cover patients who were uninsured (including persons who were undocumented or not eligible for Medicaid) and individuals who were under-insured with high co-pays. Many providers estimated this was a minority of their patients—10–30%—but for some, it was still a meaningful group.
Contracting
When planning for HSS began, the state pursued a contracting process enabling organizations to submit bids to establish hub and spoke sub-systems. A state policy-maker described a “very open” process, though the state “didn't have a lot of folks outside of OTPs really apply.” Other participants characterized the bidding process as opaque. Participants described how larger organizations were better positioned to apply, even if they were less favorably positioned to understand the specifics of rural care delivery. Of seven sub-systems with at least two rural spokes, six contracts were awarded to a single organization operating for-profit OTPs exclusively, using the OTPs as hubs to create six distinct hub and spoke systems. Several providers and administrators of established MOUD programs in rural regions only learned about the state's HSS initiative after contracts had been finalized. Several providers expressed concern that a company with little footprint in the rural counties most impacted by opioid use had received multiple contracts despite the presence of well-established organizations locally that possessed capacity to deliver relevant services. One participant observed their disappointment after the contracts had been awarded that, “It looked like all this money that was being given to the state by the federal government was going to be funneled through corporations…and we didn't like that.”
In contrast, a state policy-maker clarified that contracts awarded to the OTPs were intended to overcome inertia that long limited treatment options in rural areas: “Because of local stigma [against methadone], they've had a really hard time opening clinics and then also, because of what it costs, because you have to have a certain amount of volume to start up the OTP.” Yet participant perspectives indicated that holding state HSS contracts did not necessarily remove the stigma against OTPs, with participants stating their discomfort with methadone itself as well as the for-profit nature of the OTP organization. By the end of STR funding, one new OTP site had been built as a limited-service medication unit for stable patients; another contracted hub was only finally about to open after lengthy deliberations with county supervisors.
Inter-organizational networks
Several participants who were aware of the Vermont model distinguished its MOUD landscape from that in California, suggesting that the “hubs [in Vermont] were very mature and very well developed.” In contrast, while participants acknowledged that several rural California counties had buprenorphine providers, strong hubs were lacking, making it challenging to build the inter-organizational relationships at the heart of HSS that facilitate technical assistance for new providers and a continuum of stepped care for patients. Across several regions, established providers described forging their own informal networks to share expertise and help organizations establish their own MOUD programs. “We had already been talking to most of the groups that [hub contractors] went and established as spokes,” noted one provider who had played a large leadership role in the region, arguing that “we were the hub, and we still are the [de facto] hub, I think.” In other rural communities, buprenorphine providers were few and far between—and disconnected from one another.
Many spoke providers and leaders were clear about their distrust of hub contractors, given the opaque nature of the contracting process and their own skepticism regarding methadone therapy and the for-profit nature of the hub OTPs. These buprenorphine providers commented that, though methadone was an option some patients needed, they felt that for-profit OTPs tended to maintain patients on methadone without advancing their recovery for their own economic gain. This distrust challenged the formation of inter-organizational relationships between hubs and spokes. Knowing this stigma, one hub sub-system coordinator made sure that their spoke recruitment efforts downplayed their affiliation with the methadone provider to avoid this stigma.
Client/consumer advocacy
Likewise, harm reduction service providers lamented their exclusion from the effort to design HSS given their expertise regarding the needs of people actively using drugs in their communities. In their view, existing treatment systems were falling short in addressing these needs. Considering the pattern of gradual divestment in the rural behavioral health landscape in California over the past two decades, one harm reduction service provider admitted that they were “all excited to hear that there was going to be help for rural counties” once HSS funding was announced, but then realized that “the help has been chosen by someone in some committee about where it would be best spent and it has gone to the [methadone] clinics.” Some providers also were critical of centering HSS investments on clinical treatment: “You get the feeling that these people believe if we get enough MAT provider doctors and nurse practitioners out here prescribing, the problem's going to vanish. It's craziness.” A treatment-focused approach was premised on people who use drugs reaching and sustaining treatment when there are considerable barriers to doing so. “It's very ‘if they come, they come,’” described one provider who had hoped for more resources for intensive outreach to facilitate engagement and retention in care.
In contrast, harm reduction organizations offered a range of creative, accessible, and evidence-based services that were driven by demands from people who use drugs, including distribution of syringes and other drug use equipment based on need; peer-based “secondary” syringe distribution to people unable to reach formal service sites; free and confidential distribution of naloxone; and important ancillary health services for people using drugs and experiencing homelessness such as foot care. Harm reduction groups invested substantially in non-judgmental outreach tailored to address co-occurring needs and diverse groups, especially those in remote rural areas. One harm reduction advocate was wary that new funds would support healthcare outreach not sensitive to the needs of people using drugs amid severe isolation and poverty: “I don't want somebody trained by healthcare workers and know[ing] nothing about street outreach…and how difficult it is to engage somebody at a level where they're only worried about whether they could eat today.”
The philosophy driving harm reduction services was conceptually distinct from the clinical MOUD model driving HSS. Both models of care were grounded in respecting the needs of people who use drugs, but the harm reduction model drew attention to exclusionary aspects of MOUD programs, such as prioritizing abstinence, mandating in-person office appointments and psychosocial counseling, restricting take-home doses, and dismissing the expertise of people who use drugs. Including the perspectives of harm reduction advocates in the design of HSS, these participants argued, would have led to a system that included more relevant strategies to serve the diverse needs of people who use drugs.
Implementation
At the start of implementation, hub contractors began recruiting a network of regional spokes of private practitioners, FQHCs, and Rural Health Clinics. Some sub-systems included a number of new X-waivered providers; others included established providers with little need for support. Policy-makers and spoke providers alike agreed that hubs engaged in intensive work to create these sub-systems. Yet spoke leaders and providers were split on the implementation of HSS. Overall, participants who were part of existing, larger MOUD programs in rural areas felt little impact when they signed on as spokes in the HSS. However, participants in regions with few MOUD providers and participants with smaller practices—particularly private practices—gained critical resources to expand access to care as they signed on to HSS. The funding restrictions and large geographic distances between hubs and spokes led to significant adaptations to the initial HSS intervention, including little patient movement between hubs and rural spokes and an alternative model of MAT teams that were hired ad-hoc by spokes.
Policies
The California HSS built on new coverage afforded through the ACA's Medicaid expansion and STR funding. However, because many providers predominantly served patients already enrolled in Medicaid, taking part in HSS did not guarantee financial resources to expand their patient base: “I just don't see it being a big implication for us if we move forward with the [spoke] contract. Except for capturing those people that don't have any insurance.” Despite appreciating the possibility of treating new patients through STR funding, many providers described shortcomings of this financial model for Medicaid, uninsured, and under-insured patients. While some patients qualified for treatment through Medicaid, in some counties administrative backlogs resulted in those patients still having to pay out-of-pocket for up to 3 months if deemed ineligible for STR funding. Providers described the challenge of watching stable patients move in and out of the window of eligibility for Medicaid income limits due to social security payments, temporary jobs, or increasing income during recovery. Finally, while the bundled Medicaid rate given to FQHCs was financially sustainable, the low Medicaid reimbursement rate for private practitioners made it financially unviable to provide MOUD to Medicaid patients. One hub coordinator explained this low rate posed a big challenge to recruiting spokes: “Why should they take on this extra responsibility, this extra liability, just to make a tiny bit more money?”
Inter-organizational relationships
One goal of HSS is to establish strong relationships in which hubs provide technical assistance to spokes and facilitate patient flow between hubs and spokes as treatment needs change from acute to chronic. A state policy-maker stressed the effort rural hub contractors invested in building relationships with spokes during the initial grant period, explaining that their current work is “really focusing on training up those spokes and assisting them.” However, many spoke providers described ephemeral relationships with their hubs, even if they had been characterized by positive interactions with hub personnel concerning eligibility for services and support with grant-funding documentation.
Distance and the burden of building new facilities restricted the degree to which hubs supported spokes. Two of four HSS sub-systems in the North lacked full OTPs as hubs halfway through the two-year grant period. While many participants understood and even sympathized with the local opposition that hub contractors encountered in their efforts to establish these programs, several noted that the lack of a physical site undermined hubs’ efforts to support spokes. “It seems really difficult to be a hub,” reasoned one participant, “if you're cutting the ribbon [on a new clinic] right then and there too, to be able to provide support.” Even for established hubs, challenges remained for supporting spokes equally. Noted one hub provider, “We're listed as ‘these are our spokes’ and yes, we're serving them, but it's not always all of the services… I've answered questions or linked them with other resources through email, but it's not like a …well-oiled machine yet.”
The majority of spoke providers indicated that distances between their sites and hubs restricted patient flow. “We're not sending anybody to [the hub] because why would we do that?” reasoned one provider. “It's difficult to get patients from our rural area [to come to our clinic]. [The hub is] a two-hour drive…You are not going to be able to get buy in from patients to go that frequently.” In contrast, providers in the few spokes that were geographically close to hubs welcomed the opportunity to offer another treatment option.
Participants observed that hub providers often had less expertise to support buprenorphine treatment in the spokes. Many providers felt comfortable with their own expertise in serving patients, including those with conditions that HSS guidelines marked as too acute to be treated in an outpatient setting. Echoing sentiments expressed by others, one provider stated, “I have a lot more experience [than the hub providers] and we have challenging patients.” However, a few providers that had successfully established MOUD practices expressed relief that financial support to pursue X-waivers and to take part in MOUD-related continuing education events was provided by the state HSS administration.
Advocacy/consumer organizations
Hub contractors had some flexibility in funding to spend on broader goals related to prevention (e.g., school programs, outreach, harm reduction programs such as syringe services) and recovery (e.g., housing), in addition to treatment. However, harm reduction advocates described how state rules required hubs to allocate such money through formally-organized coalitions focused on opioid use prevention and intervention. 30 While coalitions varied across regions, some were reportedly dominated by advocates who were explicitly against harm reduction, neglectful of the perspectives of people who use drugs, or unaware of the needs of remote populations with the highest need. This had the tendency of funneling funding more toward sobriety-focused organizations rather than ones that included broader visions of health for people who use drugs, “however that looks for them.”
Sustainment
While we collected our data halfway through the implementation period of HSS, many participants expressed concerns about the proposed plans for sustainment.
Funding
While the ACA would continue to cover most treatment costs for patients treated in the HSS during the sustainment period, many participants were concerned that there were no plans to cover gaps left by the withdrawal of federal STR funding for un- and under-insured patients. Considering these conditions, established providers found it challenging to understand the benefits of becoming part of a sub-system: “I personally don't see anything they could bring to this program other than money, which would be temporary money, to make something and then leave.” These concerns about sustainability made some spoke administrators reticent to rely on HSS funding, particularly to hire new personnel. Many providers also reported that private insurers rarely were willing to cover the full costs of MOUD outside of medication, expressing fear that the high costs would force patients to abandon treatment without the grant subsidy under HSS.
Inter-organizational relationships
The purpose of HSS was to create an enduring system of inter-organizational relationships between hubs and spokes to improve and expand treatment. Yet several participants expressed doubts about sustaining these relationships long-term, particularly those that were newly-formed during the implementation period. Some participants expressed vague enthusiasm about possibly strengthening their relationships—without knowing exactly how they could be strengthened. Others shared doubts that hubs would be motivated to continue relationships with spokes after grant period. “They're a private company,” posed one systems-level stakeholder who pointed out the divergent funding models of hub OTPs and the public clinics serving as spokes: “Why would they?”
Discussion
This study provides insight into system-level factors that shape the implementation and sustainment of HSS as an intervention to expand access to MOUD and address the needs of people with OUD, particularly as the system is scaled up to larger states and regions. We found that the implementation of core HSS components changed considerably to account for contextual differences in healthcare resources and geography. The system-level factors we explored from the EPIS model across the planning, implementation, and sustainment periods—policies, funding, inter-organizational relationships, and advocacy—indicate key challenges in adapting the HSS for different rural contexts.
Policy and funding
Our findings demonstrate both the potential and limitations of HSS under the ACA. Medicaid expansion vastly increased the number of people eligible for OUD treatment and has led to improved outcomes for people with OUD. 31 , 32 However, our findings underscore challenges for patients at the edge of eligibility. Our results echo literature on the system-level barriers faced by providers in smaller rural organizations seeking to deliver MOUD, 8 including limited rates for Medicaid reimbursement and lack of coverage for core components of MOUD, like testing and the option for substance use counseling. STR funding addressed these obstacles during the implementation period through implementation strategies (e.g., increasing reimbursement rates for some spokes), yet it was unclear how these obstacles would be overcome after STR funding ended. While California's HSS helped address these obstacles in the immediate term for many rural providers, our study indicates the need for long-term funding to manage the administrative burden and expand financial support of MOUD. Furthermore, our findings indicate that the preeminent focus of HSS design on MOUD access failed to address larger deficits at the root of rural healthcare disparities. This focus on MOUD left inadequate resources to expand outreach, respond to healthcare provider shortages, extend space, and increase resources for mental health.
Inter-organizational relationships
The large geographic areas of rural California necessitated adaptation of two core components of HSS—mobile MAT teams to support spokes and the movement of patients in a care continuum between hubs and spokes. California's practitioner landscape in rural regions—including well developed buprenorphine practices in some regions and less developed OTPs—challenged the leading role for hubs in the HSS model. 12 In California's adaptation, spokes often drew on their own expertise, that of regional providers, and only occasionally the hubs. Rural areas across the U.S. face barriers to establishing accessible OTPs, including geographic distance and maintaining resource-intensive organizations in areas with less demand. 7 Like the stigma against buprenorphine that has served as a barrier to expanding MOUD in rural areas, 8 , 33 skepticism of methadone can also undermine relationships between hubs and spokes. Yet this study indicates the structural factors that can exacerbate this stigma, including an opaque contracting process that appeared to privilege for-profit OTPs over others, barriers to building trust across organizations with different business models (e.g., for-profit OTP hubs, nonprofit FQHCs), and the fact that many hubs were perceived to be unable to provide necessary technical support.
Advocacy
Harm reduction service providers commented that HSS—as designed and adapted for California—held potential yet was inadequate to address the immense and unique range of needs of rural residents. These providers underscored that rural people who use drugs face immense struggles in their daily lives, outside of the intensive demands of treatment 34 – 36 and that including evidence-based practices in harm reduction not only was necessary to accommodate this vulnerability, but was in accordance with best practices for delivering MOUD. 37 , 38 In Vermont and California, HSS was designed to include harm reduction providers, 12 , 19 yet implementation strategies to include such advocates in planning and implementation were not detailed. Without intentional implementation strategies to include harm reduction service providers, hub and spoke networks will struggle to reach the vulnerable and geographically remote rural people they are intended to serve. At the same time, leaving out harm reduction service providers from system-level interventions will inadvertently further the exclusion of their organizations, which have had the least reliable funding and have persisted in the face of intense local opposition. 36 , 39 – 41
Limitations
This study centered on provider and system-level stakeholder perspectives to investigate the overall design and implementation of HSS in a single state. Future research will prioritize the perspectives of people using drugs to understand how the design of California's HSS impacts its reach and their ability to engage with care. Our study was limited by challenges faced in recruiting stakeholders from hubs, restricting our ability to illuminate barriers and facilitators to implementation among hub providers.
Conclusion
Our findings hold important implications for other system-level efforts to expand MOUD access, whether HSS or other initiatives to build inter-organizational relationships that support care for people who use drugs. Opening and publicizing contracting processes broadly are critical to establishing trusting relationships between organizations. Doing so would invite a more diverse group of service providers, particularly in harm reduction, to build on existing MOUD expertise, expand care options, and generate awareness of local needs. Enabling sub-systems to define the roles of hubs and spokes according to regional resources and to articulate specific supports needed from HSS central administrators could result in more robust inter-organizational relationships. More equitable Medicaid reimbursement for different organizational types could ensure that a broader range of rural practitioners have the flexibility necessary to cover a range of services through MOUD that were subsidized through HSS funding. Finally, investments to combat the opioid epidemic must include resources to strengthen the broader behavioral healthcare infrastructure and workforce upon which rural MOUD access depends and expand the harm reduction services upon which rural people who use drugs rely.
Footnotes
Acknowledgments
greatly appreciate the perspectives shared by all of our participants. Research assistant Ben Chen played an important role in laying the groundwork for this study. All authors have read and approved of the final version of the manuscript.
Author contributions
CSR conceptualized the study, led data collection, analysis and write-up of the results. CW and RP assisted with conceptualization, framing, and editing of the manuscript. DS assisted with data collection and editing the manuscript. HP assisted with the data analysis.