
Abstract
Background
Criminal problem-solving and dependency courts set treatment standards for opioid use disorder (OUD) but sometimes prohibit or limit utilization of medications for OUD (MOUD). Court staff beliefs about MOUD inform court treatment policies. Court staff MOUD policies may also be influenced by social norms, meaning perceptions of opinions of other individuals/entities about MOUD, including opinions of fellow staff in their court, staff in other courts, the state supreme court, other state agencies, the National Association of Drug Court Professionals (NADCP), federal agencies, and local peer support groups. To date no study has examined social norms among court staff with respect to MOUD.
Methods
We distributed an online cross-sectional survey in 2019 to all criminal problem-solving and dependency court staff in Florida. Respondents were asked to identify the extent to which they cared about different entities’/individuals’ opinions about MOUD and the extent to which they perceived each of those entities/individuals as encouraging MOUD. We hypothesized that court role and court type would be associated with responses. We used descriptive statistics, logistic regressions, and difference of proportions tests to analyze data.
Results
20% of the population (n = 119) completed the survey. Respondents cared most about the opinions of external treatment providers with whom they collaborate, fellow staff in their court, and the NADCP regarding MOUD. Fewer than half felt that any of these entities/individuals encourage methadone or oral buprenorphine. Additionally, fewer than 11% of respondents felt that local twelve-step peer support groups encourage the use of any form of MOUD.
Conclusions
MOUD education should target all members of court teams, including collaborating treatment providers. Since court staff care relatively little about the MOUD opinions of staff in other courts, changes in opinions in one court may not affect changes in opinions in a neighboring court. The NADCP should more explicitly state its support for MOUD, and specifically oral buprenorphine and methadone treatment.
Keywords
Introduction
Criminal problem-solving courts and dependency courts have seen increasing rates of clients with opioid use disorder (OUD) in recent years. 1 – 4 Criminal problem-solving courts, such as adult drug courts, juvenile courts, and mental health courts, set treatment requirements for OUD and refer court clients for treatment in lieu of incarceration. 3 , 5 , 6 Similarly, dependency courts set and monitor treatment requirements for reunification of parents with children after loss of custody due to drug use. Within both types of courts, judges lead teams of court staff who collaborate with external treatment providers in referring clients for treatment and monitoring treatment progress. 4 , 7
Even though judges and court staff typically lack medical training, they may set policies or practices restricting client utilization of medications for OUD (MOUD). 8 , 9 Such court policies or practices could harm client health outcomes by limiting utilization of MOUD, which has been demonstrated to decrease risk of opioid overdose by as much as 50%, to prevent OUD relapse, and to decrease the incidence of communicable diseases. 10 – 13 For example, some courts ban client use of certain medications (methadone, buprenorphine, or naltrexone), limit the time period for which medications may be used (e.g., a few months only), or prohibit completion of the court program/reunification with children while MOUD is being utilized. 8 , 9 Furthermore, some courts have formal or informal practices in which they exclusively refer clients to healthcare providers who do not utilize MOUD. 8 One recent study found that court clients (as compared to individuals in jails or prison or on probation/parole) were among those in the criminal justice system least likely to be referred to buprenorphine or methadone treatment. 14
Practices or policies limiting MOUD access may be contrary to best practice standards set by organizations such as the National Association of Drug Court Professionals (NADCP) 5 and, in some cases, by state law. 15 Federal law also prevents courts that ban MOUD from obtaining certain types of funding. 16 Nevertheless, to our knowledge most states do not prohibit courts from limiting MOUD utilization, and NADCP best practice standards are voluntary. When a state does not mandate a uniform policy with respect to MOUD for courts, then individual courts operate autonomously, sometimes resulting in two courts in the same geographic locality differing with respect to MOUD policies. 8 At the individual court level, treatment-related practices and policies are typically made in court teams led by a judge, but also including case managers, administrators, probation/parole officers, defense attorneys, counselors associated with external treatment providers, and/or others. In Florida, these team members (hereinafter “court staff”) typically attend weekly or bi-weekly “staffings” or “team meetings,” during which they set policies, discuss participant progress through the court program (e.g., advancement to new phases), and decide sanctions/incentives. Although all court staff engage in regular information sharing and meetings, they may differ with respect to employer. Judges, court case managers, and administrators are typically employed by the court system, with court case managers assisting with court-related data collection (e.g., urine drug screens), scheduling of court events (e.g., hearings), and tracking progress within the court program (e.g., movement through phases of the court program.) Clinical case managers and counselors are usually directly employed by an outside healthcare organization that partners with the court, with the clinical case manager coordinating treatment appointments and referrals. Likewise, probation/parole officers, defense attorneys, law enforcement officers, and others are not employed directly by the court system. The beliefs about MOUD among court staff inform their practices and policies, 8 , 9 and studies to date suggest that court staff beliefs about the safety and efficacy of methadone and buprenorphine may be negative. 9 , 17
Individual beliefs of court staff about MOUD may be impacted by whether they perceive other individuals (e.g., fellow court staff; the court treatment provider) or other organizations (e.g., the state supreme court; the NADCP) as encouraging MOUD. It is unknown to what extent court staff care about others’ MOUD opinions and whether court staff perceive others as encouraging MOUD. Policymakers could utilize such information to design targeted interventions for changing court staff MOUD beliefs. For example, if researchers find that court staff strongly value the NADCP's opinion about MOUD, then the state could fund court staff to attend NADCP trainings about MOUD. Similarly, if researchers find that court staff strongly value the state supreme court's opinion about MOUD, then the state supreme court could make a proclamation about the importance of MOUD access in courts. Equally importantly, if researchers learn that an organization whose opinion court staff value is perceived as discouraging MOUD, then policymakers could try to facilitate more positive MOUD-messaging by that organization, such as through collaboration in developing trainings for court staff.
To address this gap in the literature, this study examined the extent to which criminal problem-solving and dependency court staff care about certain entities’/individuals’ beliefs about MOUD (e.g., the NADCP, fellow staff in their court, the Substance Abuse & Mental Health Services Administration, external treatment providers), and the extent to which court staff believe specific individuals/entities encourage each type of MOUD (i.e., methadone, oral buprenorphine, and extended-release naltrexone.)
We hypothesized that court role and court type would be associated with the likelihood a respondent cares about a specific entity's/individual's MOUD opinion. Based on previous qualitative research, 8 and since most staff lack medical training, we expected that respondents would be most likely to care about the opinions of healthcare providers, who could fill knowledge gaps. This research is part of a broader project examining court staff MOUD beliefs in Florida.
Methods
Instrument development
As part of a cross-sectional survey exploring MOUD beliefs among criminal problem-solving and dependency court staff in Florida we designed questions examining two dimensions of the social norms construct, described below. To create our social norms survey questions, we consulted a manual for survey development based on the Theory of Reasoned Action and Planned Behavior. 18 Although social norms could be examined through various theories, we believed the Theory of Reasoned Action and Planned Behavior was most appropriate for our study because in the future we hope to examine the relationship of social norms to a specific action – court staff permitting MOUD utilization. This theory posits that social norms, beliefs, and self-efficacy with respect to an action (e.g., permitting MOUD) each affect intention to act, which in turn affects action. 19 , 20 According to this theory, the social norms construct consists of two dimensions: (1) one's beliefs about others’ attitudes toward a behavior (e.g., permitting MOUD) and (2) whether one cares about others’ attitudes toward that behavior. 18 , 19 Questions about social norms for each medication were asked separately with brand names included. See Appendix A for survey questions relevant to this paper. Prior to fielding the survey, we piloted the survey with court staff and then modified it based on feedback.
Dimension 1
We created measures to examine whether the respondent cares about an entity's or an individual's opinion about MOUD. Respondents were asked “To what extent do you care about each of the following entities’/individuals’ opinions about medication-assisted treatment (i.e. formulations of methadone, oral buprenorphine, or extended-release naltrexone) for opioid use disorder?” The entities/individuals included: (1) the NADCP; (2) the Florida Supreme Court; (3) fellow court staff; (4) healthcare provider with whom the court partners; (5) the Substance Abuse & Mental Health Services Administration (SAMHSA); (6) the Florida Office of the State Court Administrator (OSCA); (7) the area managing entity (i.e., the local organization responsible for overseeing Medicaid-funded clinics); (8) the Florida Department of Children and Families (DCF); (9) local twelve-step support groups; and (10) staff in other Florida courts. For each entity/individual, respondents could choose: (1) I do not care at all; (2) I somewhat care; (3) I care a lot; (4) I don't know; or (5) I choose not to answer.
Dimension 2
We created measures to ascertain the extent to which other entities/individuals encourage MOUD. Respondents were instructed to do the following: “Please mark the extent to which each of the following entities/individuals encourage the use of [medication] for opioid use disorder.” Respondents were asked to rate the level of encouragement provided by each entity/individual for methadone, oral buprenorphine, and extended-release naltrexone [hereinafter: ER naltrexone] separately. Respondents could choose: (1) strongly discourage; (2) somewhat discourage; (3) neither encourage nor discourage; (4) somewhat encourage; (5) strongly encourage; (6) I don't know; or (7) I choose not to answer.
We also included questions asking respondents to identify the type of court in which they work, their court staff role, gender, and rurality. For confidentiality reasons, we did not ask respondents to identify their court location, but we asked them to identify in which of nine geographic regions in Florida they work (e.g., northeast Florida, southeast Florida, etc.)
Data collection
In July 2019, we emailed the online Qualtrics survey link to 585 problem-solving and dependency court staff in Florida, which is the entire population of such staff in Florida. Researchers received court staff email addresses from the Florida Office of the State Courts Administrator. Three reminder emails were sent to court staff who had not completed the survey over the course of two weeks. The survey was open for two weeks.
Ethics
This research was approved by the Institutional Review Board at the University of Central Florida. Informed consent was received from all participants prior to taking the survey. Participants were promised confidentiality and did not receive an incentive for participation.
Data analysis
For dimension 1, we created dichotomous outcome measures equal to 1 if the respondent selected “care somewhat” or “care a lot” and 0 otherwise for each of the 10 entities/individuals. For dimension 2, we created dichotomous outcome measures equal to 1 if the respondent selected “somewhat encourage” or “strongly encourage” and 0 otherwise for each of the 10 entities/individuals about each medication (for a total of 30 items).
We measured court type as a dichotomous indicator variable for whether the respondent worked in a court that was a criminal problem-solving or a general dependency court. Criminal problem-solving courts included: (1) adult drug courts; (2) driving under the influence (DUI) courts; (3) juvenile drug courts; (4) veterans court; and 5 other criminal courts (e.g., mental health courts). The reference group, dependency courts, included: (1) early childhood courts; (2) family dependency drug courts; (3) general dependency courts; and (4) other dependency courts (e.g., a combination of two of the dependency courts listed). “Other” was also an option for court type. Some respondents who answered “other” for court type wrote in answers. If the write-in answer fit into one of the previously mentioned court types, they were included in that court type; otherwise, the “other” responses were included in the “other” court type category. Court roles included: (1) court case manager; (2) court administrator; (3) judge; and (4) “other.” “Other” included staff members not employed directly by the court, such as clinical case managers, counselors, law enforcement, and corrections officers. We also included indicator variables for female and urban or mostly urban court location. Finally, we included indicator variables for geographic region.
We estimated descriptive statistics showing the percentage of respondents indicating they “somewhat care” or “care a lot” about the opinion with respect to MOUD for each entity/individual and whether they think the entity/individual “somewhat encourages” or “strongly encourages” the use of methadone, oral buprenorphine, or ER naltrexone. For research question 1, we estimated a series of logistic regressions to explore the relationship between covariates and whether respondents cared about the opinion of each entity/individual (Table 1). In addition to the independent variables described above, we included a control for region in the logistic regressions. We estimated difference of proportions test (using “prtest” in Stata 16) 21 to examine if there were differences in the proportions of respondents who cared about an entity's/individual's opinion of MOUD across organizations. Finally, we tested for differences in proportions of respondents who agreed that one entity/individual encourages MOUD relative to another. All analyses were conducted in Stata 16. 21
Odds Ratios for Caring about Opinion of Organization (Care a lot/Care somewhat).
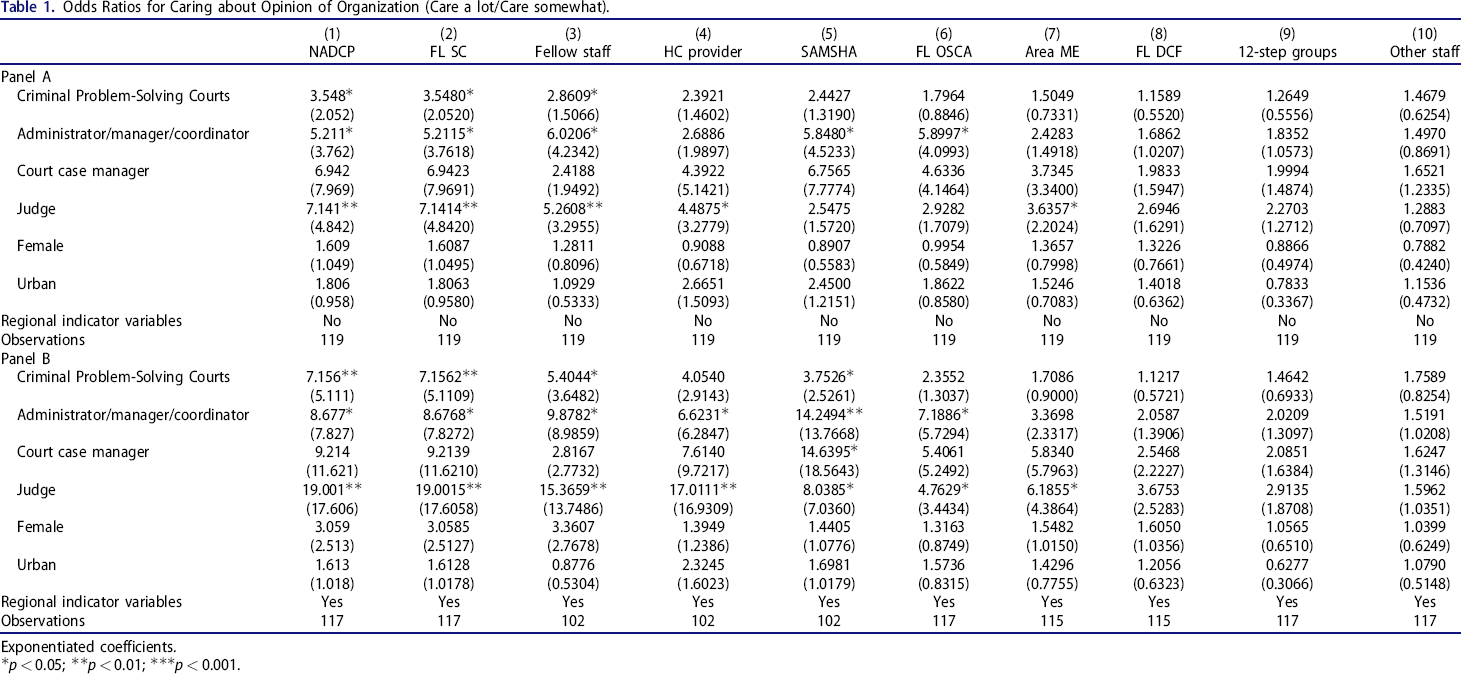
Exponentiated coefficients.
p < 0.05;
p < 0.01;
p < 0.001.
Results
Descriptive statistics
We received a total of 154 survey responses, or 26% of the population of Florida problem-solving and dependency court staff. We excluded those who did not complete the survey (n = 31) and observations with missing data for urban (n = 2), court type (n = 1), and court role (n = 1), which resulted in a sample of 119 observations and a response rate of 20%. Table 2 presents descriptive statistics for the covariates. Most respondents were staff in criminal problem-solving courts (55%). The most common respondent role in the sample was judge (43%), followed by administrators (27%), other roles (18.5%) and court case managers (11.8%). Over 80% of the sample was female, and 64% said their court was in an urban or mostly urban area. In total, six of nine geographic regions accounted for the majority of regions in which respondents worked, with three geographic regions each accounting for fewer than 2% of respondents. No single geographic region was indicated by more than 21% of respondents.
Covariate means.
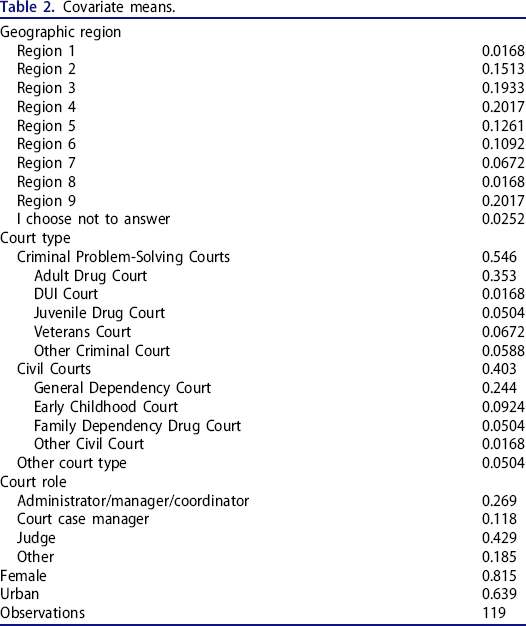
Figure 1 presents the percentage of respondents indicating they cared about the MOUD opinion of each entity/individual. The entities/individuals that respondents most commonly cared about were collaborating healthcare providers (87% of respondents), fellow staff in the court (86%), and the NADCP (82%). Between 75 and 80% of respondents indicated they cared about the opinions of SAMHSA, the Florida Supreme Court, Florida OSCA, the area managing entity, and Florida DCF. The least frequently selected categories were twelve-step groups (68%) and staff in other courts (65%).
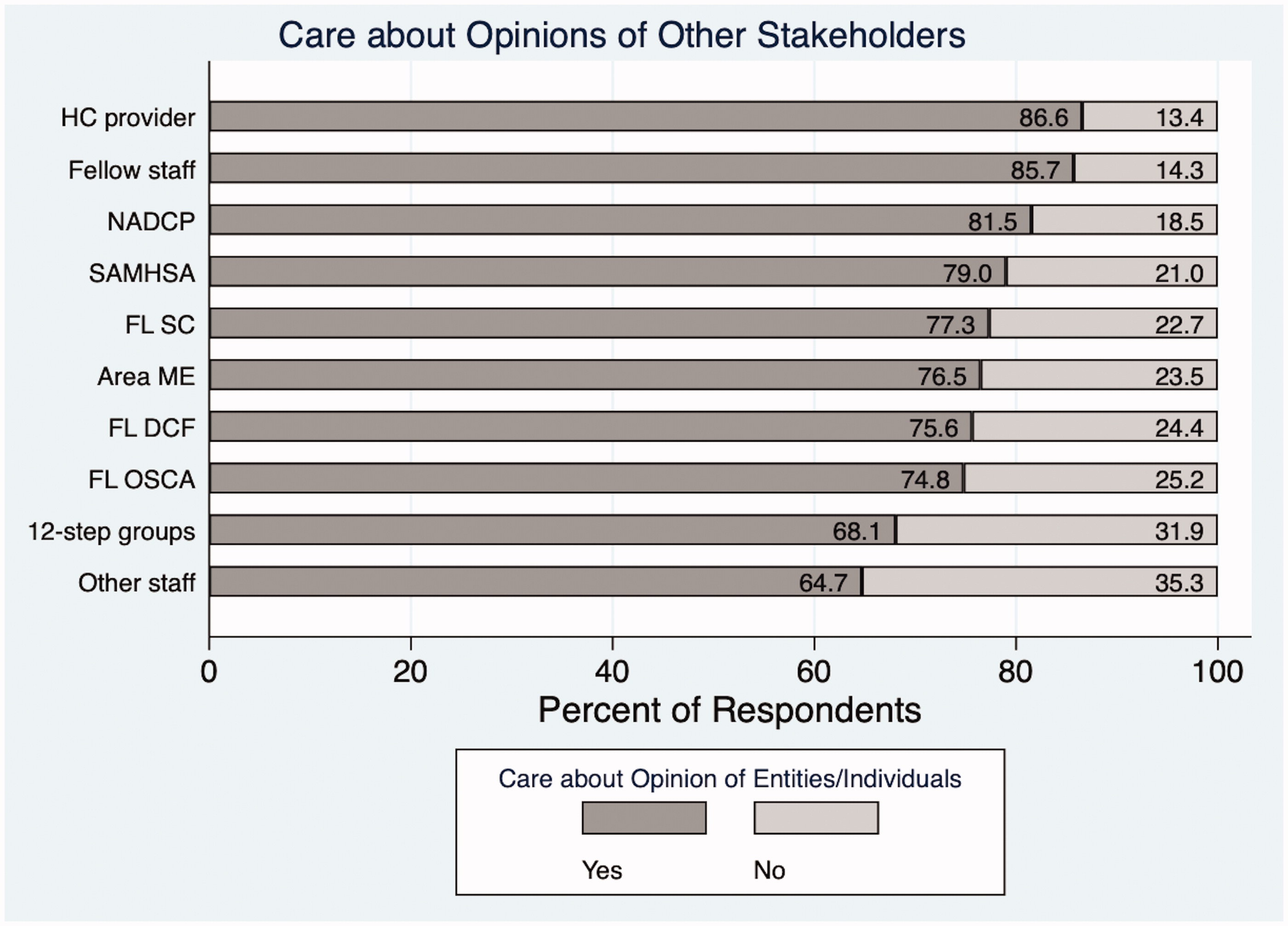
Extent to which respondents care about others’ MOUD opinions.
Figure 2 presents the percentage of respondents agreeing that an entity/individual encourages methadone. Fewer than half of respondents (42%) agreed that the NADCP encourages methadone, while between 30 and 40% of respondents indicated that the area managing entity, fellow court staff, the healthcare provider with whom the court collaborates, SAMHSA, OSCA, and DCF encourage methadone. Fewer than a quarter of respondents agreed that the Florida Supreme Court encourages methadone (22%). Staff in other courts (14%) and twelve-step groups (5%) had the lowest percentages for encouraging methadone.
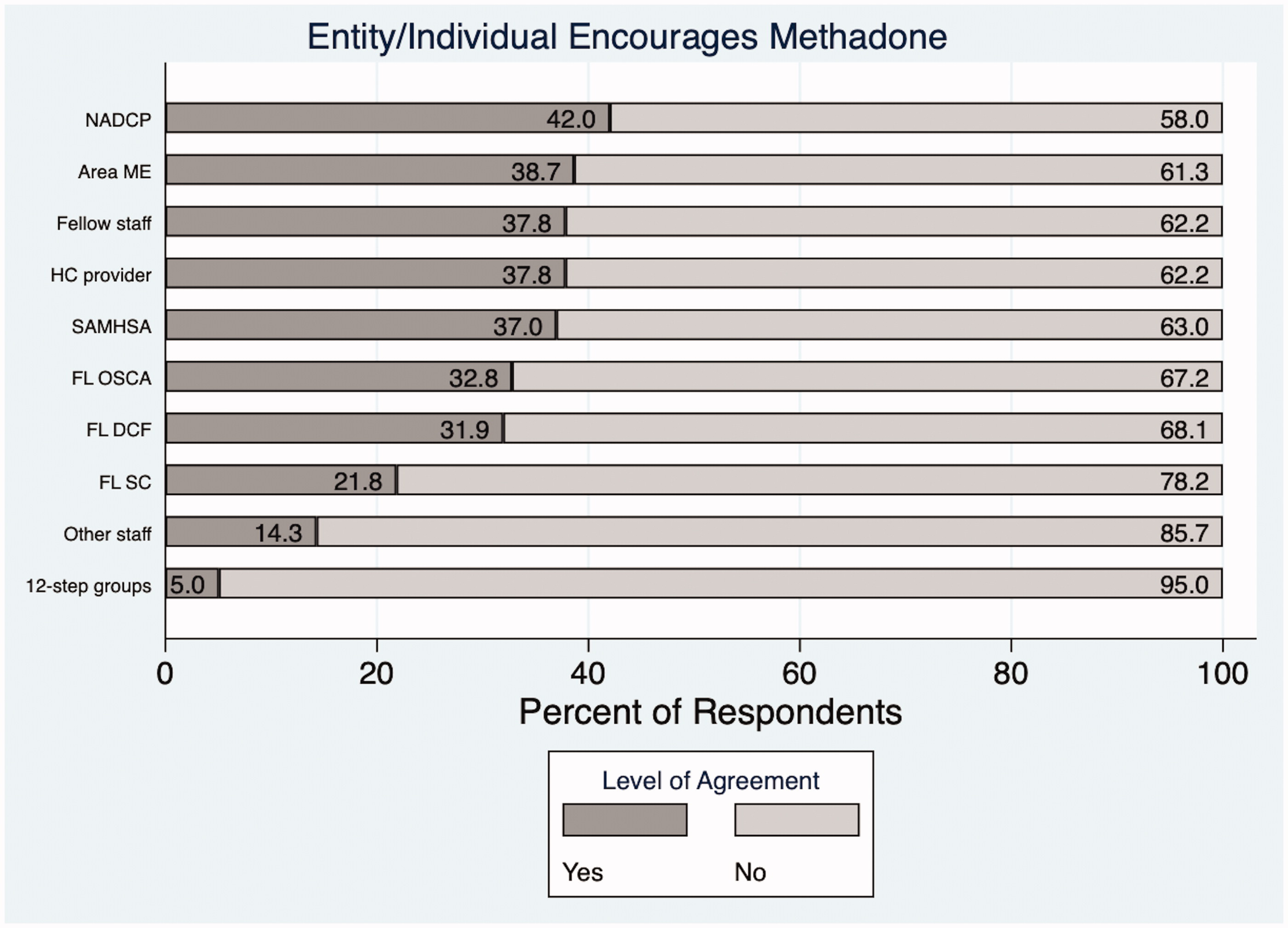
Perceptions that others encourage methadone.
Figure 3 presents the percentage of respondents agreeing that an entity/individual encourages buprenorphine. Almost half of respondents agreed that fellow court staff (49%) and the healthcare provider with whom the court collaborates (49%) encourage oral buprenorphine. A quarter of respondents (24%) believed that the Florida Supreme Court encourages oral buprenorphine. Only 8% believed that twelve-step groups encourage oral buprenorphine.
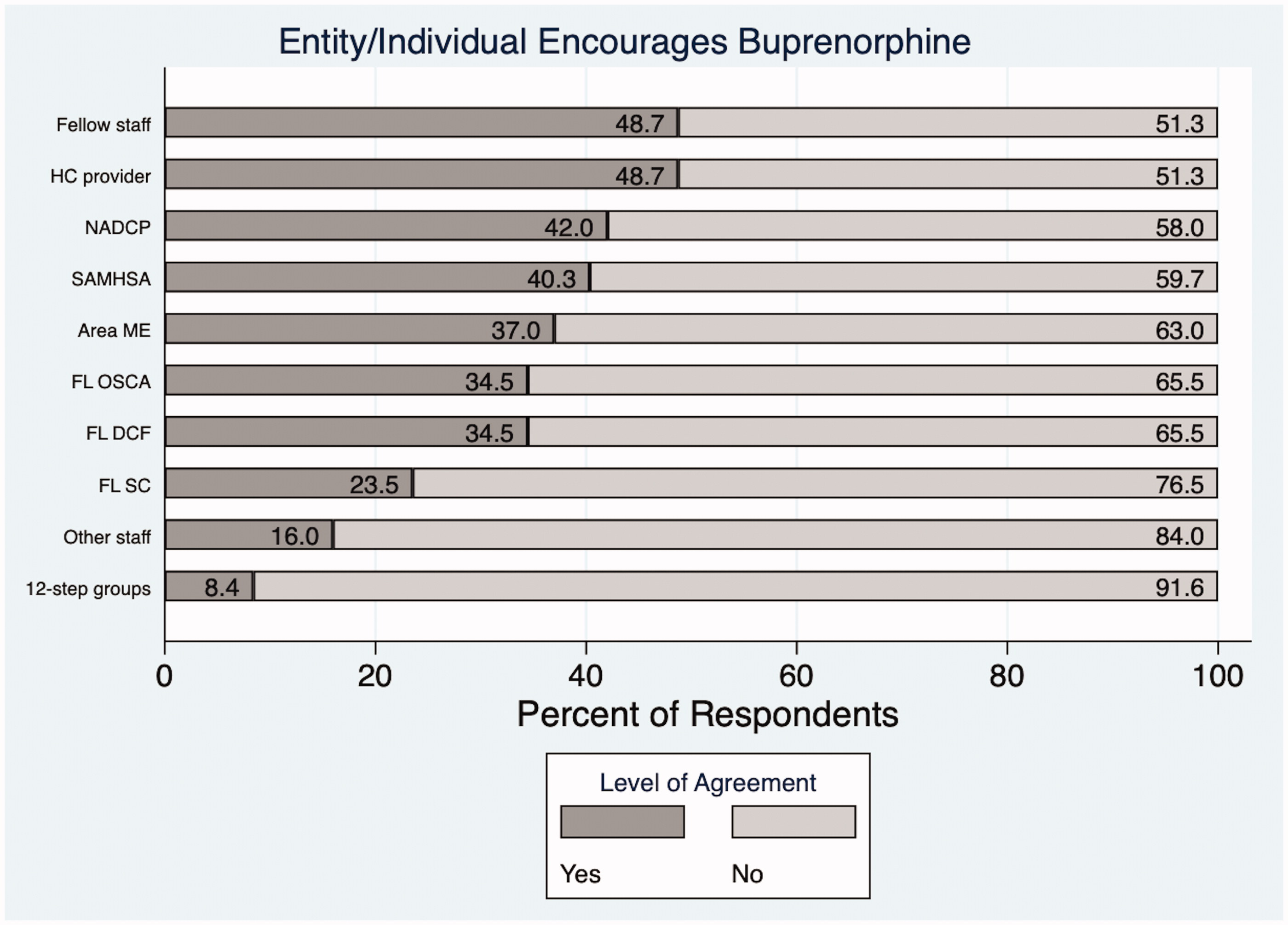
Perceptions that others encourage buprenorphine.
Figure 4 presents the percentage of respondents agreeing that an entity/individual encourages XR naltrexone. The two entities/individuals most commonly perceived as encouraging XR naltrexone were fellow court staff (58%) and collaborating healthcare providers (54%). Between 35 and 50% agreed that the NADCP, the area managing entity, SAMHSA, OSCA, and DCF encouraged XR naltrexone. A quarter thought the Florida Supreme Court encouraged XR naltrexone. The least commonly selected entities/individuals with respect to encouraging XR naltrexone were staff in other courts (18%) and twelve-step groups (11%).
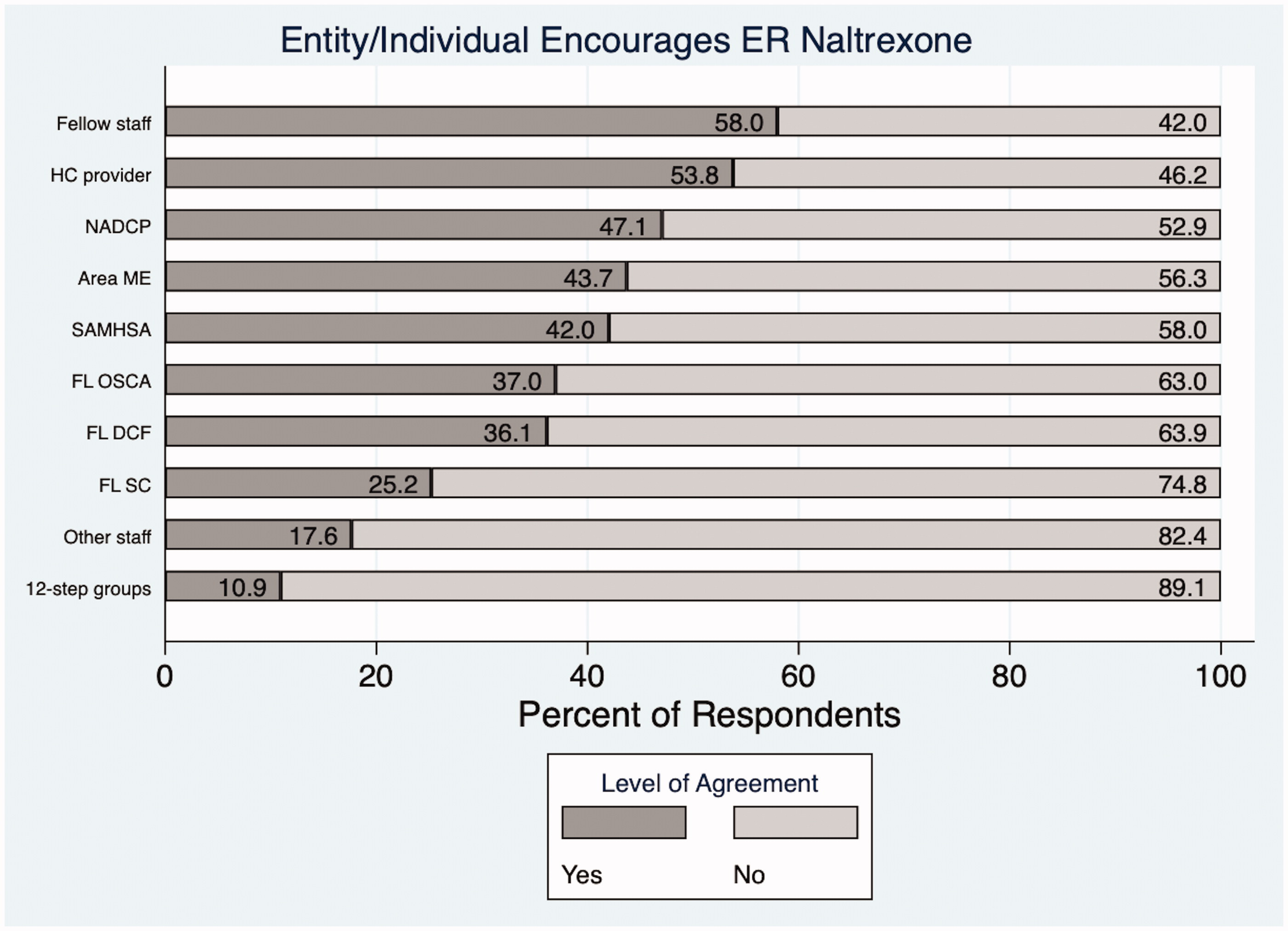
Perceptions that others encourage naltrexone.
Figure 5 shows results comparing perceptions of whether an entity/provider encourages MOUD by specific medication. For each individual/entity, more respondents indicated that XR naltrexone is encouraged than oral buprenorphine or methadone. Except for the NADCP and the area managing entity, more respondents selected that the entity/provider encourages oral buprenorphine than methadone.
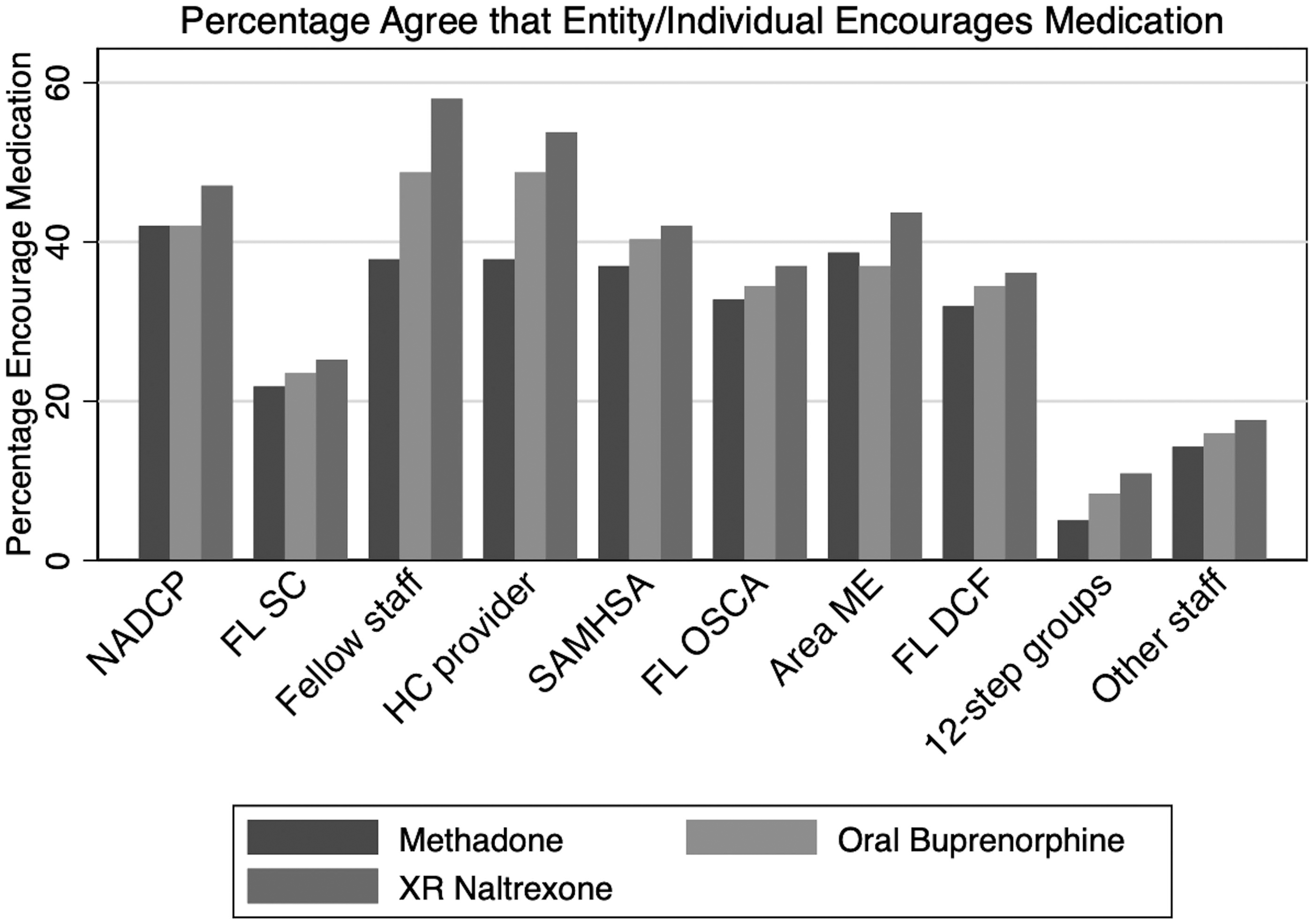
Comparison by medication of perceptions of others’ encouragement.
Logistic regressions
Results from the logistic regressions for whether a respondent cares about the opinion of each entity/individual are presented in Table 1. We hypothesized that court role and court type would be associated with the likelihood a respondent cares about a specific entity's/individual's MOUD opinion. We found some evidence to support this expectation. Specifically, staff in criminal problem-solving courts were more likely than staff in dependency courts to indicate that they care about the opinions of the NADCP (OR 7.156; p < 0.01), the Florida Supreme Court (OR 7.1562; p < 0.01), fellow court staff (OR 5.4044; p < 0.05), and SAMHSA (OR 3.7526; p < 0.05). Administrators were more likely than court staff in the “other” category to care about the opinions of the NADCP (OR 7.156; p < 0.05), the Florida Supreme Court (OR 8.6768; p < 0.05), fellow staff (OR 9.8782; p < 0.05), the healthcare provider with whom the court collaborates (OR 6.6231; p < 0.05), SAMHSA (OR 14.2494; p < 0.01) and OSCA (OR 7.1886; p < 0.05). Court case managers were more likely that other staff to care about the opinions of SAMHSA (OR 14.6395; p < 0.01). Judges were more likely to care about the opinions of the NADCP (OR 19.001; p < 0.01) the Florida Supreme Court (OR 19.0015; p < 0.01), fellow staff (OR 17.0111; p < 0.01), SAMHSA (OR 8.0385; p < 0.05), Florida OSCA (OR 4.7629; p < 0.05), and the area managing entity (OR 6.1855; p < 0.05). Female respondents and staff in courts that are in urban or mostly urban areas were not more or less likely to care about any entity/individual opinions about MOUD. No independent variables were associated with the likelihood that a respondent cared about the opinions of Florida DCF, 12-step groups, or staff in other courts.
Difference of proportions test
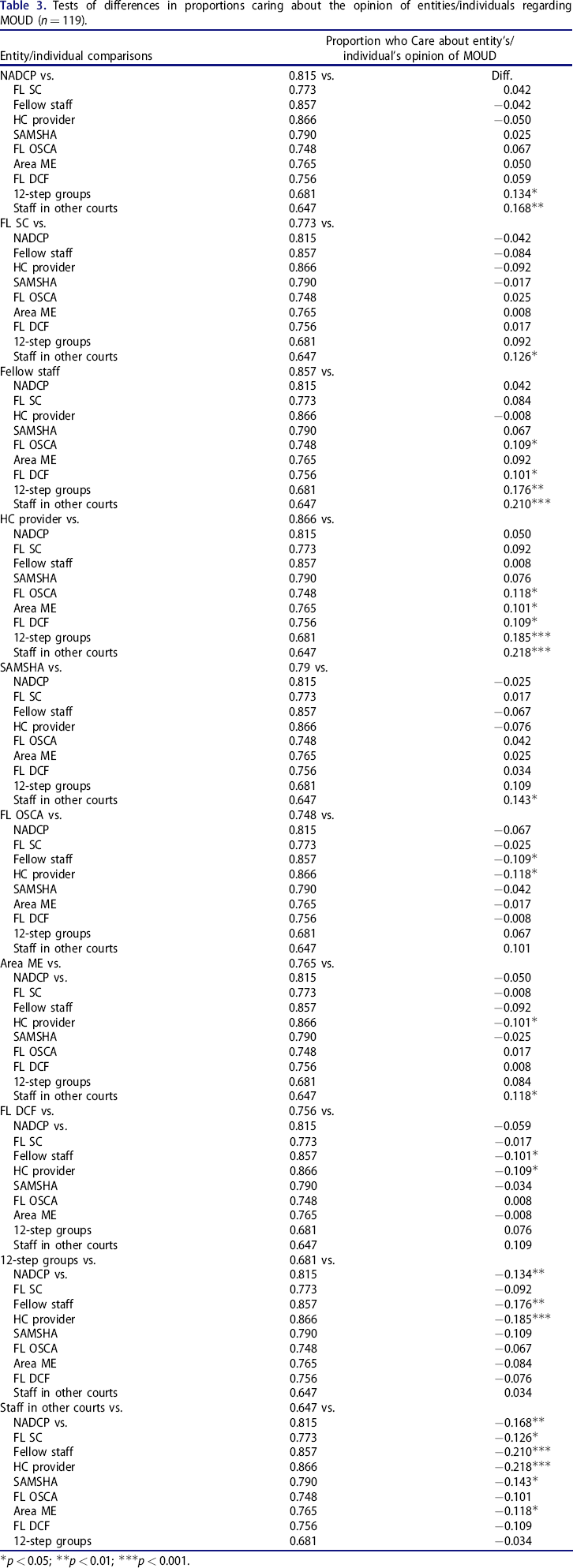
Table 3 presents the results for the difference of proportions tests for whether respondents indicated they cared about each entity's/individual's opinion of MOUD. The proportion of respondents who indicated they cared somewhat/cared a lot about each entity's/individual's opinion about MOUD was compared to this proportion for other entities/individuals.
Tests of differences in proportions caring about the opinion of entities/individuals regarding MOUD (n = 119).
p < 0.05;
p < 0.01;
p < 0.001.
Compared to the NADCP, Florida Supreme Court, fellow staff, the healthcare provider with whom the court collaborates, SAMHSA, and the area managing entity, respondents were less likely to indicate they cared about the MOUD opinion of staff in other courts. Respondents were more likely to care about the opinions of fellow staff and the healthcare provider with whom the court partners than the opinion of OSCA, DCF, twelve-step groups, and staff in other courts. Additionally, a higher proportion of respondents indicated they cared about the opinion of the healthcare provider with whom the court collaborates relative to the opinion of the managing entity about MOUD. More respondents said they cared about the opinions of the NADCP, fellow staff, and the healthcare provider with whom the court collaborates relative to the opinion of twelve-step groups.
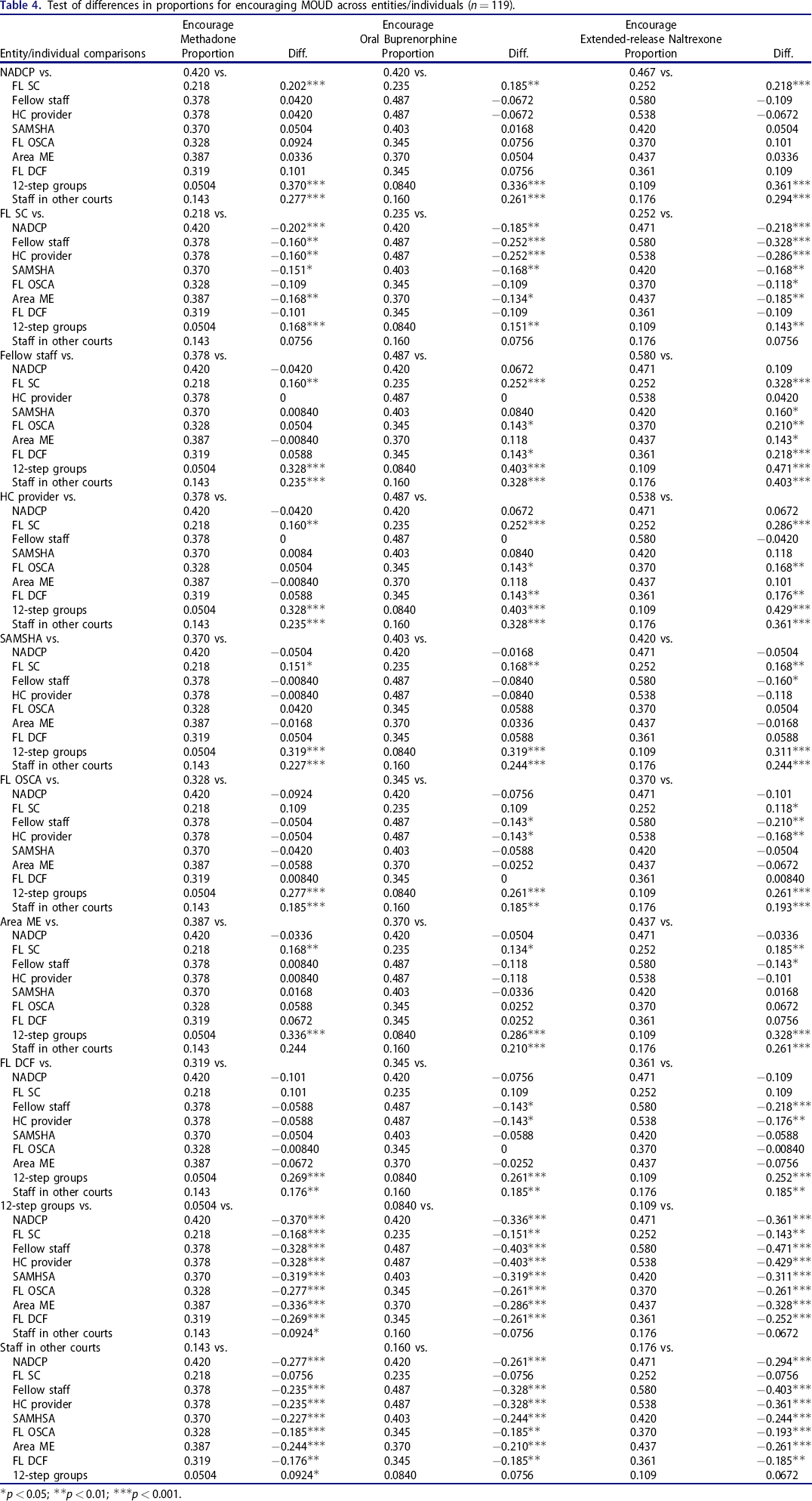
Table 4 presents the results for the difference of proportions tests for encouragement of methadone by the entity/individual. All possible two-way comparisons are shown. In general, as compared to other entities/individuals, respondents were less likely to indicate that the Florida Supreme Court, 12-step groups, and staff in other courts encourage each type of medication. Compared to the NADCP, fellow staff, the healthcare provider, SAMHSA, and the area managing entity, respondents were less likely to think the Florida Supreme Court encourages any type of MOUD. Respondents considered 12-step groups and staff in other courts less likely to encourage methadone than all other entities/individuals. For oral buprenorphine and XR naltrexone, respondents considered 12-step groups less likely to encourage these medications than all the other entities/individuals except for staff in other courts. Respondents also considered staff in other courts to be less likely to encourage oral buprenorphine and XR naltrexone than all other entities/individuals except for 12-step groups.
Test of differences in proportions for encouraging MOUD across entities/individuals (n = 119).
p < 0.05;
p < 0.01;
p < 0.001.
Discussion
To our knowledge, this is the first study to examine criminal problem-solving court and dependency court staff social norms with respect to MOUD, including whose opinion court staff care about and the perceived opinions of those entities/individuals with respect to MOUD. We used a convenience sample of criminal problem-solving and dependency court staff in Florida, with 20% of the population completing the survey. Importantly, we found that court staff care most about the opinions of healthcare providers with whom the court partners (87% of respondents caring), followed closely by the opinions of fellow staff in their court room (86% caring).
Since the survey asked respondents whether they care about “court staff” opinions without distinguishing between court staff roles, it is unclear whether respondents value all team member opinions equally. For example, it is possible that court staff value the judge's opinion more than the court case manager's opinion, or vice versa. Future research should explore these differences. Nevertheless, given that criminal problem-solving court staff and dependency court staff make decisions as teams, 8 , 22 – 24 we recommend that educational interventions about MOUD target all roles. Based on the importance of MOUD opinions of treatment providers, according to our survey results, we also strongly recommend that education target all external treatment providers with whom courts collaborate. Unfortunately, targeting educational initiatives toward all court roles and external treatment providers may be logistically difficult, because in Florida only the contact information for judges and/or court administrators tends to be publicly available. We recommend that state law require each type of court to maintain an up-to-date website with the names of court staff, including external treatment providers with whom the court collaborates.
A previous qualitative study found that court staff defer treatment decisions to collaborating treatment providers, 8 but this is the first quantitative study to find that court staff highly value the opinions of external treatment providers with respect to MOUD. Given that most court staff (i.e., judges, probation/parole officers, court administrators, court case managers, attorneys, prosecutors) lack healthcare backgrounds, we are pleased with this finding. At the same time, fewer than half of respondents perceived the collaborating treatment provider as encouraging methadone (37.8%) or oral buprenorphine (48.7%) treatment, despite decades of efficacy data for both treatments 25 —an important and problematic finding. Courts select treatment providers with whom they collaborate. Therefore, it is possible that courts with policies prohibiting or limiting MOUD choose to collaborate with external treatment providers who do not provide MOUD and/or who have negative beliefs about MOUD. To our knowledge, no formal mechanism in Florida exists to ensure that court staff collaborate with treatment providers who offer MOUD. This problem is further exacerbated by the common practice of courts collaborating with only one or two external treatment agencies 8 (something encouraged by NADCP best practice standards to ease treatment monitoring 5 ) potentially limiting information flow about MOUD from other treatment providers to court staff.
The majority of respondents cared about NADCP opinions with respect to MOUD. Unfortunately, fewer than half felt that the NADCP encourages MOUD. We caution, however, that we have no way of knowing the accuracy of the respondents’ perceptions of the NADCP's encouragement of different medications. Our results suggest that the NADCP should more explicitly voice support for treatment of court clients with MOUD, particularly with methadone and oral buprenorphine. Relative to other court roles, judges were significantly more likely to care about the opinions of the NADCP, the Florida Supreme Court, fellow staff, SAMHSA, and OSCA. The Florida Supreme Court is composed of justices and has the ability to discipline state judges, potentially explaining judges’ perceived importance of the entity's opinions.
Relative to general dependency courts, staff in criminal problem-solving courts were more likely to care about the opinions of the NADCP, the Florida Supreme Court, fellow staff, and SAMHSA. NADCP opinions may be more relevant to criminal problem-solving courts, because the NADCP trainings target adult drug courts, which are the most common type of criminal problem-solving courts in Florida and among our survey respondents.
In light of previous studies of stigma toward MOUD among twelve-step group participants, 26 , 27 we are not surprised to find that fewer than 11 percent of court staff felt local twelve-step groups encourage any kind of MOUD. Only five percent of the sample believed that twelve-step groups encourage methadone. The majority of court staff (68.1%) cared about the opinions of local twelve-step support groups with respect to MOUD. Courts often require peer support group participation for clients. Therefore, even if court staff and treatment providers encourage MOUD, court clients may feel pressure to stop utilizing MOUD from local twelve-step groups.
In general, more respondents indicated that each entity encourages XR naltrexone as compared to buprenorphine, and more respondents indicated that each entity encourages oral buprenorphine as compared to methadone. These perceptions may not reflect actual encouragement of each individual/entity; nevertheless, according to the Theory of Reasoned Action and Planned Behavior, the mere perception of encouragement (or lack thereof) could influence behavior. 19 Our results are problematic in that buprenorphine and methadone have a particularly strong evidence base for preventing opioid overdose and relapse. 10 , 11 It is interesting that these results resemble those found in other studies, which found that court staff have more positive opinions of XR naltrexone than buprenorphine and more positive opinions of buprenorphine than methadone. 8 , 17 , 28
Finally, we found that court staff were least likely to care about the opinions of staff in other courts with respect to MOUD, even though the vast majority of respondents cared about the opinions of fellow staff in their own court. This finding is unsurprising given the autonomous nature of courts, with courts in the same county sometimes setting very different MOUD policies. 8 Although we did not examine the role of social norms in behavior change, this result suggests that merely changing MOUD beliefs or policies in one court could have little effect on neighboring courts.
Our paper has several limitations. First, we utilized a convenience sample of court staff and were unable to match court staff to specific courts; therefore, the representativeness of the opinions in this paper is unknown. For example, we do not know the extent to which respondents came from the same court. Additionally, since we were provided contact email addresses from the Florida Office of the State Courts Administrator without roles associated with each name, we were only able to ascertain the roles of individuals who completed the survey via a question about role, but were not able to ascertain roles of those who did not complete the survey. Second, our sample size was limited, with only 20% of the population completing the survey. We attempted to increase the response rate through reminder emails. Given recent federal case law suggesting that MOUD prohibition in the criminal justice system is a violation of the Americans with Disabilities Act, 29 , 30 we suspect that court staff with more positive views about MOUD would have been more likely to respond to our survey. Third, as discussed previously, we cannot identify whether court staff care about all staff members’ opinions equally, or whether they care about the opinions of certain individuals (e.g., judges) more than others. Additionally, the survey was not validated; however, survey development was guided by the Theory of Reasoned Action and Planned Behavior to conceptualize “social norms” using a survey development manual. Finally, as a cross-sectional study, we were unable to ascertain whether changes in social norms affect beliefs or practices with respect to MOUD, something that a future study should explore. Likewise, a future study should examine the relationship between social norms, individual beliefs about MOUD, and perceived barriers to MOUD.
Footnotes
Disclosure statement
In 2017, Dr. Andraka-Christou received a research grant from Alkermes, Inc. to develop online education about substance use disorder for college students and a mobile health tracking application for college students. The Florida Office of the State Courts Administrator did not have any role in the design, data collection, or analysis of the study, except providing the researchers with the email addresses of all criminal problem-solving court and dependency court staff in Florida.
Authors’ contributions
Dr. Andraka-Christou conceptualized the project, obtained funding for the research, led development of the survey instrument, recruited participants, and led manuscript drafting. Dr. Atkins led analysis of the data and assisted with manuscript drafting and editing.
Funding
This work was supported by the Florida Office of the State Courts Administrator.
Data availability statement
Deidentified survey data, with small cell sizes redacted, is available from the corresponding author by request.
Selected questions from survey instrument
Q1 Among the following types of courts, in which one do you currently spend the MOST time as a staff member or team member? Adult drug court (1) Veterans Court (2) Juvenile drug court (3) Family dependency drug court (4) General dependency court (5) Early Childhood Court (6) DUI court (7) I choose not to answer (8) Other (9) ________________________________________________
Q2 Which of the following Judge (1) Judicial Assistant (18) Court administrator/manager/coordinator (2) Court case manager (3) Clinical case manager (4) Substance use disorder counselor (5) Mental health counselor (6) Physician, nurse practitioner, or physician assistant (7) Veterans Justice Outreach Specialist (8) Department of Children and Families attorney (9) Defense attorney (10) Prosecutor (11) Police Officer (12) Probation or Parole officer (13) Peer support of parent partner (14) Clerk of Court (15) I choose not to answer (16) Other (17) ________________________________________________
Q32 Have you completed a graduate degree program? (e.g. Master's degree, PhD, MD, JD)
Yes (1) No (2) I choose not to answer (3)
Q33 What is your gender? Male (1) Female (2) Other (3)
Q35 How would you best describe the county in which you spend the MOST time as a court staff member? Completely urban (1) Mostly urban (2) Mostly rural (3) Completely rural (4) I choose not to answer (5)