
Abstract
Background
In general, research has found that patient-centered substance use disorder treatment is positively correlated with improved patient outcomes. However, little research has examined what factors make intake assessments—the first step in addiction treatment—patient-centered.
Methods
We conducted interviews with 30 Medicaid-enrolled individuals who received addiction treatment in California about their experiences with the intake assessment process.
Results
Participants reported that the intake assessment process evoked strong feelings, both positive and negative. Some participants said that answering detailed questions about their substance use, mental health, and social relationships, for example, was cathartic and gave them helpful insights. Other participants found the questions invasive, exhausting, and anxiety provoking. Participants also emphasized how critical it is for the person conducting the assessment to be supportive, nonjudgmental, and attentive. Participants recommended delaying the comprehensive assessment because they did not feel physically or emotionally ready to complete the intake.
Conclusions and recommendations
Patients’ introduction to addiction treatment is typically the intake assessment. By understanding how patients experience intake assessments, providers can make the process more patient-centered, which may lead to improved patient outcomes.
Keywords
Introduction
Poor treatment retention is a persistent challenge in substance use disorder (SUD) treatment. Patients who remain in treatment longer are more likely to achieve positive treatment outcomes. 1 – 5 Although it typically takes at least 3 months in treatment for patients to significantly reduce or stop their substance use, most patients do not stay in treatment that long. 6 About 30% of patients discontinue treatment within 1 week of program enrollment. 7 For these patients, the intake assessment is one of the only contacts—and perhaps the only contact—they ever have with a program before they stop treatment.
Research has demonstrated that greater patient satisfaction with specialty addiction treatment is associated with reduced substance use, better treatment attendance, and increased retention. 8 Patient-centered treatment is respectful to patients’ values, preferences, and expressed needs; is coordinated and integrated; gives patients information that is trustworthy, responsive, and tailored to their needs; ensures physical comfort; provides emotional support; and involves family and friends. 9 This type of treatment has been shown to improve patient engagement in other types of healthcare. 10 , 11
Patient-centeredness is related to the concept of therapeutic alliance—defined as a positive bond (i.e., personal relationship) between client and therapist and client-therapist agreement and collaboration (i.e., collaborative relationship) on therapeutic goals, tasks, methods, and intensity 12 —and may also be associated with retention in SUD treatment. 13 – 17
Ensuring that the intake assessment, the very beginning of treatment, is as patient-centered as possible and begins to build a therapeutic relationship may be an effective way to improve retention and consequently improve outcomes. While research confirms the importance of a patient-centered approach during SUD treatment, 18 there has been little research conducted on patients’ experiences with intake assessment or their perspectives on how to design intake to promote patient-centeredness and a therapeutic alliance.
Alves and colleagues 19 conducted a focus group with Portuguese clients on intake assessments for alcohol use disorder treatment, finding that clients considered assessments to be helpful for their therapeutic processes but also that they sometimes found intake questions to be difficult to answer or overly invasive. Additionally, these clients preferred for therapists to administer evaluations and they wanted assessments to give them opportunities to self-reflect and discuss challenges other than those directly related to substance use.
Mark and colleagues 20 used survey data collected in the United States to compare client perceptions of assessments that aligned with the American Society of Addiction Medicine (ASAM) criteria, assessments conducted with ASAM ContinuumTM software, and other assessments. The ASAM criteria require that the intake assessment query patients about six biopsychosocial domains: acute intoxication and/or withdrawal potential; biomedical conditions and complications; emotional, behavioral, and cognitive conditions and complications; readiness to change; relapse, continued use, and continued problem potential; and recovery environment. Clients who received ASAM-based assessments and ASAM ContinuumTM assessments were more likely to report that the provider conducting the assessment wanted to learn about their situation and asked good questions, that the provider discussed what they learned about the client's addiction and treatment recommendations with them, that their assessments are comprehensive, that their assessments make them think about their goals for treatment, and that they are more satisfied with their level of care placement. However, clients receiving assessments using ASAM ContinuumTM software were more likely to report that assessments are too long or ask repetitive questions.
This article presents the findings from qualitative interviews with a subset of clients (n = 30) who participated in Mark and colleagues’ study of assessment tools. Our overarching goal is to better understand clients’ experiences with and perceptions about SUD intake assessment and to offer recommendations to improve intake assessments and potentially increase treatment retention and success.
Methods
We conducted telephone interviews with 30 Medicaid-enrolled individuals who received SUD treatment in California from a specialty addiction treatment provider. These individuals were a subset of participants who participated in a survey of their experiences with the intake assessment process that were recruited and consented by addiction treatment facilities (N = 851) (see Mark et al. 20 for detail on the main study). Clients who completed the survey consented to be contacted for a telephone interview.
We stratified the study participants by type of assessment—assessments based on the ASAM Criteria, the ASAM ContinuumTM software, and other assessment tools—and then randomly selected individuals within each category and sent an email invitation. A total of about 45 individuals responded to participate in interviews, and 30 of them, who received treatment from 15 different addiction treatment programs, completed interviews. The interviews occurred between November 2018 and March 2019. Each interview lasted approximately 30 minutes. The research team provided a toll-free number for participants to use for the interview, and participants received a $75 gift card on completion. The study was reviewed and approved by the New England Independent Review Board (IRB) and the UCLA IRB.
We conducted semistructured interviews to elicit participants’ perceptions of the intake assessments, including questions on what they believed was the purpose of assessments, the comprehensiveness of the assessments they received, their perceptions on the logistics of assessments (e.g., length, timing, and format), and how they felt about their relationship with the providers who conducted their assessments. Interviews were conducted by two doctoral-level researchers trained in qualitative interviewing and one master's-level researcher with qualitative research experience who performed interviews under the oversight of the two senior researchers.
All interviews were audio-recorded (with consent), transcribed, and uploaded into Dedoose qualitative software for analysis. The research team analyzed the transcripts using template analysis, a group of techniques for thematically analyzing textual data. 21 The team developed an initial codebook based on the topic areas and key questions in the interview guide, such as understanding the purpose of assessment and perceptions about the comprehensiveness of the assessment. After reviewing 20% of the interview transcripts and discussing emerging themes, the team refined the codebook to capture themes and issues discussed during the interviews. Two master's-level qualitative analysts then double-coded 20% of the interviews to assess initial intercoder reliability and refine the codebook using an iterative process. Intercoder reliability was then tested in double-coding 10% of the transcripts, which established a mean kappa score of 0.76. The remaining interviews were coded independently by the two analysts. On completion of coding, the team reviewed the extracted codes and data, discussed emerging themes, and reached consensus on interpretation. To reach consensus on interpretation, the team discussed the meaning of the excerpts, considered the context, and agreed on themes.
Results
The participants had similar demographic characteristics to all Medicaid beneficiaries receiving addiction treatment in California (Table 1). The mean age of participants was about 33 years and 36 years for the statewide addiction treatment population. Participants were more likely to be female (57% as compared with 41%) and white (73% as compared with 57%) than in the general addiction treatment population in California, and slightly less likely to be Hispanic (28% as compared with 36%). Participants were about equally divided between outpatient (53%) and residential (47%) treatment programs at the time of their intake assessments. Participants were about equally divided among the three types of assessments (37% ASAM-based, 30% ASAM Continuum™ software, and 33% not based on ASAM).
Characteristics of the Qualitative Interview Sample Compared to Statewide Medicaid Population.
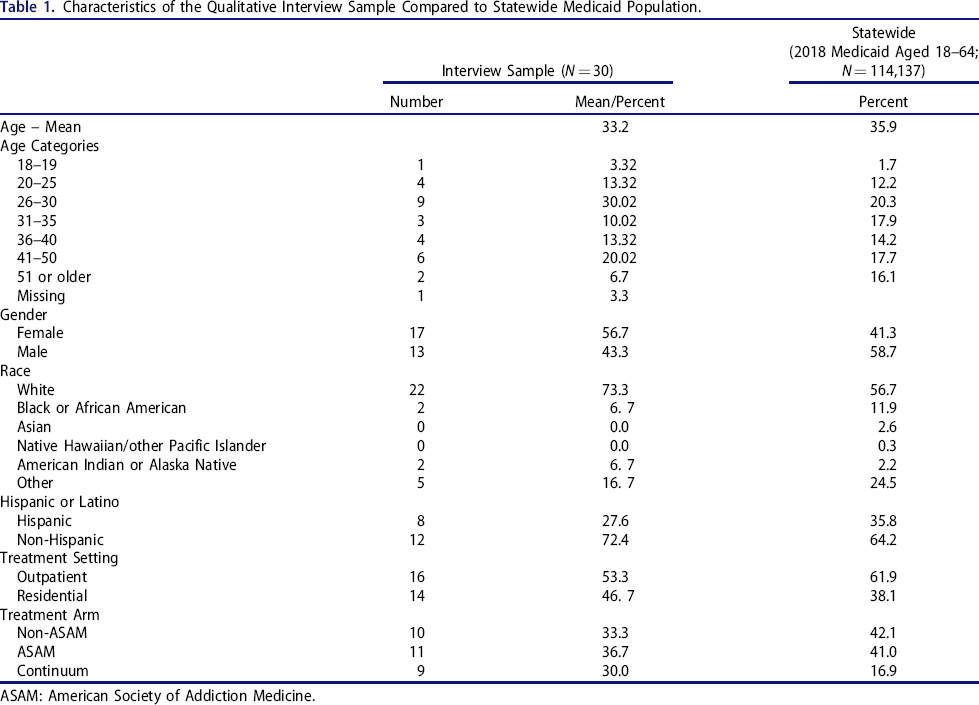
ASAM: American Society of Addiction Medicine.
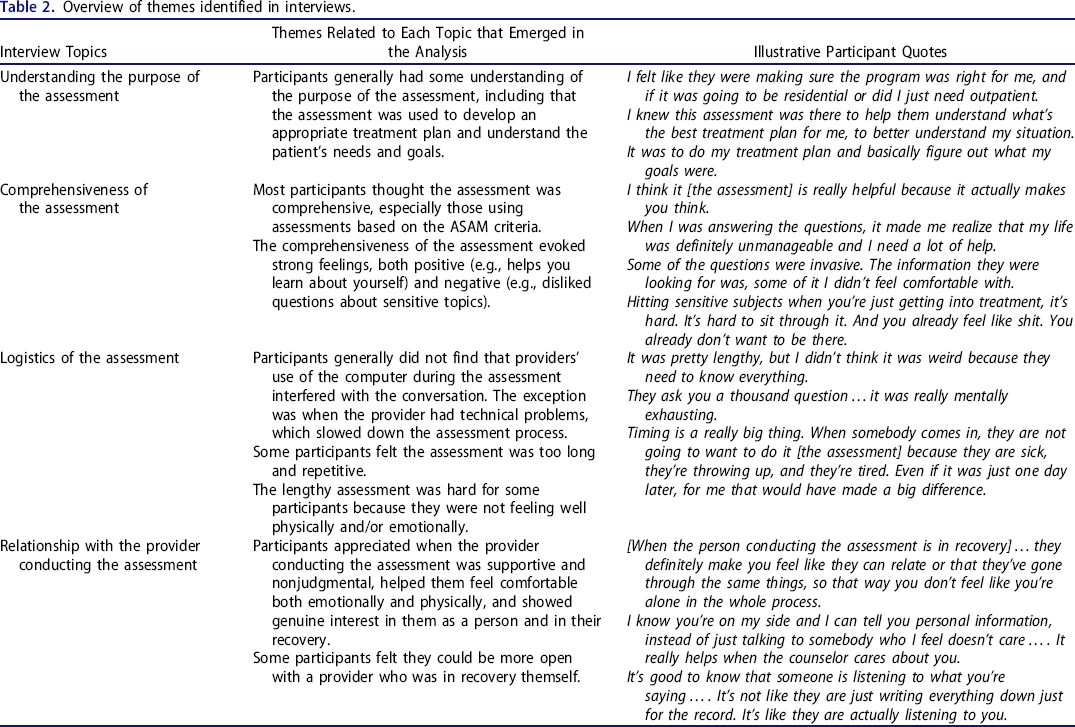
Table 2 provides an overview of themes identified in the interviews, which are discussed in detail below, and presents illustrative participant quotes.
Overview of themes identified in interviews.
Understanding the purpose of intake assessment
We asked participants whether the provider conducting the intake assessment explained the purpose and how the assessment would be used. Participants reported being told that intake assessments would be used to develop an appropriate treatment plan (10 participants), understand the client's goals for treatment (8 participants), determine appropriate level of care (6 participants), determine what their insurance would cover (6 participants), or that they did not remember (5 participants). As one participant reported, the intake assessment “was there to help [providers] understand what's the best treatment plan for me, to better understand my situation.”
However, some participants were unsure about the purpose of the assessment or thought it was “just paperwork,” “just part of the intake process,” or primarily for insurance purposes. One participant had expected the assessment to be “more an evaluation, a little more…personal” and was disappointed that it felt like “just an insurance thing, trying to get it out of the way.”
Comprehensiveness of assessments
We asked participants whether during the intake assessment the provider had asked questions to assess each of the six ASAM domains. Participants reported that the assessments addressed multiple aspects of their life and not just substance use; all 30 participants reported they were asked about physical and mental health. Most participants (22 participants) reported being asked about factors that would cause them to relapse and about factors that might help or get in the way of recovery, such as family, friends, jobs, or school (23 participants). Fewer participants reported being asked about their readiness to change their substance use (16 participants) or about withdrawal symptoms (17 participants).
Overall, participants from sites using the ASAM ContinuumTM or other assessments based on ASAM (referred to as Continuum participants or ASAM participants, respectively) were more likely than other participants to report that the provider asked about withdrawal symptoms, readiness to change, and aspects of their recovery environment that could potentially protect against relapse. All 8 Continuum participants and 6 out of 8 ASAM participants reported being asked about withdrawal symptoms as compared with 3 out of 6 non-ASAM participants. All Continuum participants (10 participants) and ASAM participants (11 participants) reported being asked about their recovery environment, compared with 4 out of 7 participants who received non-ASAM assessments.
Participants reported that the intake assessment process evoked strong feelings, both positive and negative. Some participants (12 out of 30 participants) reported their experience was generally positive and helpful. Specifically, participants explained that questions that “actually make you think” and “help you learn about yourself” were beneficial because they brought into focus how important it was for them to make changes in their lives: “When I was answering questions, it made me realize that my life was definitely unmanageable, and that I needed a lot of help.” Although difficult, discussing challenging aspects of their life could be cathartic: “As much as sometimes it really sucks when you pull that Band-Aid off…you need to let things out…that's why it was good for me. I needed it.” Beyond clarifying their needs, comprehensive assessments also highlighted clients’ assets and left them feeling encouraged: “When you're in addiction, you don't realize how much support you have…. And those questions are asked [and you think]‘Oh, holy crap! I do have support. I do have friends, I have the church. I do have everything they're asking about.’” These participants reported that by laying out challenges and strengths, assessments were a valuable introduction to treatment: “…the assessment really helps you with the first step in recovery.”
Conversely, some participants (8 out of 30 participants) reported their assessments were too “invasive.” These participants questioned the relevance of information concerning their personal life, family life, and painful experiences in the past. For one participant, “just going through the entire thing of hitting all [the areas] where you're messed up” was a difficult introduction to treatment. Specifically, participants reported that questions about past trauma and sexual activity, including sexual abuse, felt unpleasant and unnecessary because it was “bringing up a lot of old stuff that I had already worked past.” One participant reported feeling uncomfortable and fearing discussing sensitive topics because of the potential consequences of disclosure: “…because if I said [something] or [something was] not said—if I worded something incorrectly, someone [would have] mistook it for something else and I would get committed [involuntarily to a mental health facility] or something.” Some participants indicated that the timing of intake assessments and the inclusion of sensitive questions right at the beginning of treatment were the main causes of their discomfort: “…it's like you don't know this person, and you give ‘em a lotta information about yourself.”
Logistics of the assessment
Use of computer
We asked participants if the provider who conducted their intake assessment used a computer and how they felt about the pros and cons of assessments conducted on computers as compared with paper. Of the 30 participants, 9 said the provider conducting the assessment used paper, 13 said the provider used a computer, and 4 said the provider used a combination. A few participants (3 of 30 participants) observed problems with computer assessments, such as the computer freezing and information not saving and the provider having to start again. However, other participants (7 participants) thought computer assessments were fine because it seemed more organized and the provider was still able to pay attention and make the assessment conversational: “…he made it like a conversation. He just kept going so that I answered all the questions thoroughly.”
Length of assessment
We asked participants how long the intake assessment took and whether it was too long or too short (note this question was not asked in one interview). Approximately one-third of participants (9 of 29 participants answering the question) reported their intake assessments took under an hour, and over one-quarter of participants (8 of 29 participants) reported their assessments took over 3 hours. Continuum participants were most likely to report longer assessment times (6 of 8 participants recalled the assessment taking 3 hours or longer as compared with 1 of 11 ASAM participants and none of the non-ASAM participants). Some participants (6 of 29 participants) reported their assessments were too long: “it felt like they asked you a thousand questions” or that the questions repeated “over and over and over again.” However, other participants thought the length of their assessments was appropriate: “It was lengthy, but I was very eager to get the help” or “…this has to be done, and then I can start my treatment plan…. I didn't think it was weird because they need to know everything. I think it was good.” For some participants, lengthy assessments were positive because it gave the provider the information needed to give good care: “To me, it didn't even seem like it was 3 hours” or “…actually it was interesting to me because this [treatment] is something that I want, that I need, [and] I know that they're there to help me out.”
Timing of assessment
A few participants (5 of 30 participants) reported that the timing of the intake assessment—particularly having it when they first present for treatment—was problematic or could be improved. These participants described how they (or patients in general) were “in bad shape,” both physically and mentally, at the time of the intake assessment. Specifically, they described being intoxicated, experiencing withdrawal, being exhausted, or feeling ashamed. These participants wanted time to rest or detoxify before starting the assessment, or even just to have a break during the assessment: “Most people don't even wanna be there at that moment…and you already feel like shit…. Hitting sensitive subjects when you're first getting…treatment is hard.” One participant recalled how being in withdrawal during their intake assessment made it extremely difficult to engage in a meaningful discussion of treatment needs and preferences:
When people come in, they're so irritated they just want to be in that detox room. They're beat up. They just wanna eat…. Timing, I feel like would be a really big thing. When somebody comes in, they're not gonna want to [do it]—they're sick, and they're throwing up, or they're tired. They haven't slept. Even if it was just one day [later]… I think it would have made a big difference where I would have been more coherent to what they were asking me….
Relationship with provider conducting the assessment
Depending on how treatment programs are staffed, the person conducting the intake assessment may be an administrative staff member, a social worker (e.g., with a master's degree in social work), a physician (e.g., with a medical degree), a nurse (e.g., with a registered nurse degree), or a counselor who is certified in addiction treatment (e.g., a Certified Addiction Counselor)—these counselors are often in recovery themselves. 22
We asked participants how they felt about the provider conducting the assessment, particularly if they felt the provider genuinely cared about them and was invested in helping them find the right treatment. Participants shared positive reactions, including that the provider was supportive (18 of 30 participants), nonjudgmental (8 of 30 participants), helped them feel comfortable (8 of 30 participants), made the assessment more personalized and less like a checklist by making the process more conversational (8 of 30 participants), was relatable because they shared their own experiences with addiction and recovery (7 of 30 participants), and was experienced and knowledgeable (5 of 30 participants).
One important factor for participants was that the provider showed genuine interest in them as a person—rather than “just another patient”—and truly cared about their recovery. They were attuned to whether the provider took time to really listen to them during the intake assessment. Eye contact, body language, and active listening helped participants feel the provider was focused on them: “It's…good to know that someone's listening to what you're saying” or “they're not just writing everything down for the record, it's like they are actually listening to you.” Participants also said the provider helped them feel comfortable and supported during the intake assessment; for example, by giving them assurances of confidentiality, being told they could skip questions if they were uncomfortable answering, or being offered breaks during the assessment.
Another important factor for some participants was whether they could relate to the provider. Some participants appreciated when the provider shared their personal experience with addiction and recovery. Participants felt these providers understood what they were going through and consequently they felt less ashamed or concerned about being judged because the provider had “been in their shoes” and providers who are in recovery “…definitely make you feel like they can relate or that they've gone through the same thing. So that way you don't feel like you're alone in the whole process.”
Participants also reported that even if the provider was not in recovery, providers who were professional, open-minded, caring, and did not react negatively to any information they disclosed made them feel at ease and that they were in a “safe place.” In one instance, a participant said the provider did not seem to have personal experience with addiction, but they were very open-minded and nonjudgmental: “I never felt judgement, like not even for one second.”
Feeling that the provider cared about them and was supportive were key aspects of relatability for participants: “It really helps when the counselor really cares about you.” If providers expressed sincere interest in participants’ life stories, participants reported they were more likely to “know you're on my side and I can tell you personal information. Instead of just talking to somebody who I feel doesn't care at all and giving this really, really personal information and [wondering] what are you going to do with that?” Conversely, participants could sense if providers were uncomfortable or more focused on collecting information than listening to them.
Participants also commented on the apparent training and experience of providers conducting the intake assessment. On the positive side, one participant commented, “Obviously, [the provider] is trained in her field. She knew what I was talking about, so there was no judgement or confusion. It was just the facts.” Conversely, another participant shared the experience of a provider who seemed young and inexperienced, saying she was “just asking the questions that are on the paper…that was just it,” rather than having a real conversation.
Some participants (7 of 30 participants) shared a negative experience with the provider conducting the intake assessment. The main reasons were feeling that the provider was distracted, rushed, and just trying to “get through the paperwork.” One participant described feeling very emotional during the intake assessment and the provider was distracted and “didn't even know that I was crying. They didn't realize it.” Another participant explained that “it didn't feel personal. You thought it would be more conversational. It was almost like a checklist type thing.”
For a few participants (4 of 30 participants), the provider who conducted the intake assessment was also a counselor in the treatment program or someone the client already knew from previous treatment experience. These participants noted that they felt more open and comfortable because they already knew the person conducting the assessment: “If it was another counselor, I don't know how freely I would have been about answering some of the questions.” For other participants, the provider who conducted the assessment was not involved beyond the intake process. One participant shared that because this individual was “just an intake coordinator…they don't have to care.”
Discussion
Typically, intake assessments are the first step in SUD treatment. However, little research has been conducted on how patients experience these assessments, which is a missed opportunity to make them more patient-centered. Interviews with 30 individuals who had participated in SUD treatment intake assessment revealed that the assessment often evokes strong emotions. Some interview participants reported the experience as being cathartic and generating new insights, such as the need for treatment, their triggers, and their recovery supports. However, for other participants the assessment experience was emotionally draining at a time when they were highly vulnerable. In some instances, participants indicated they were experiencing physical and mental discomfort or were intoxicated at the time of their intake assessment, which made it difficult to engage in lengthy and personal conversations that are part of comprehensive assessments.
Because of distrust, shame, and fear of being judged, some participants said they were reluctant to be open about sensitive topics with a provider they had just met. Participants emphasized that the person doing the assessment should demonstrate genuine interest in them and their recovery. This suggests that careful consideration should be given to who conducts intake assessments; specifically, individuals with strong communication skills who use a patient-centered approach. Programs may want to consider having clinicians conduct intake assessments rather than administrative staff, and ideally the clinician will remain as part of the patient's treatment team. However, this may be logistically challenging, particularly for programs that offer same-day access. Alternatively, peer-support counselors might be well suited to conduct intake assessments, as some participants reported feeling more comfortable undergoing the assessment with a person who was in recovery themself. Additionally, these counselors may be able to maintain an ongoing relationship with the patient after the intake assessment is completed.
Participants also recommended that intake assessments be delayed or broken up into components so that they were in a better state to answer questions and felt more comfortable discussing difficult topics. Treatment programs could consider conducting a brief intake assessment to ensure that the patient is not in need of medically monitored treatment, for example, and then conduct a more extensive assessment during the first few days of treatment that delves deeply into more sensitive issues. However, this may require insurance plans to pay for a few days of treatment, rather than making a payment authorization decision at treatment initiation.
Generally, participants were not bothered by providers’ use of a computer at intake assessments, as compared with paper assessments, and in fact liked the potential efficiencies of computer assessments. However, consistent with the data from the larger patient survey, 20 patients were more likely to experience the computerized version of the ASAM intake assessment as too long and repetitive. Consequently, developers of the computerized assessment may want to explore the feasibility of using computer adaptive questionnaires, a method to reduce patient burden of traditional questionnaires by letting a computer dynamically select only the items that give new information about the patient. 23
Our findings are similar to some of the results from Alves and colleagues’ 19 small qualitative study of women in a Portuguese inpatient treatment program for alcohol dependence, which examined clients’ experiences with different assessment tools and processes. Clients generally reported that the assessment was a positive experience because it helped them reflect on their situation. We heard a similar view from some clients in the present study; however, others were not ready to be open during the assessment. Alves found that clients preferred the assessment to be conducted by the client's own therapist, making the assessment a meaningful first step in the therapeutic process. Similarly, we found that clients preferred the assessment be conducted by someone who would continue to be involved in their care, rather than “just an intake worker.”
Study limitations
Although in-depth interviews yield rich detail on patient experience, they may be less generalizable than large surveys. Participants were selected from 15 SUD programs in one state (California). Moreover, because the SUD workforce in the United States is composed mostly of counselors, peer support staff, and care managers—rather than professionals with advanced clinical degrees—the findings reported here may be different from other countries where the workforce conducting intake assessments has different levels of training and experience. 22
Participants who agreed to participate in the interviews may have differed from those that did not agree; for example, they may have been generally more or less pleased with their intake experience. Further, although our team assessed that we had reached thematic saturation with the completion of 30 interviews, it is possible that additional interviews may have led to additional insights. 24
Conclusions
We found that the SUD treatment intake assessment process evoked strong feelings, both positive and negative, among study participants. For example, some participants said that answering detailed questions about their substance use history, mental health, and social relationships was cathartic and gave them helpful insights. Other participants found the process exhausting and reacted to some questions as being too personal and invasive. Participants emphasized how critical it is for the person conducting the assessment to be supportive, nonjudgmental, and attentive.
The intake assessment is the first touchpoint for individuals entering SUD treatment. Better understanding patients’ experiences with and perceptions about the assessment can help treatment centers and providers improve the process and potentially increase treatment retention and improve patient outcomes. Our study findings highlight the importance of using a patient-centered approach that balances the need to obtain sufficient information to make appropriate level-of-care decisions with patients’ emotional and physical readiness to engage and share sensitive information.
Recommendations
To improve the intake assessment process, we offer the following recommendations for treatment center leadership, providers who conduct intake assessments, and researchers.
For treatment center leadership, first carefully consider who conducts intake assessments and provide training in patient-centered approaches. Consider counselors who have had personal experience with addiction and recovery and, as far as possible, ensure the individual who conducts the intake assessment continues to play a role in the patient's treatment. Second, design the clinical workflow to allow the intake assessment to occur over more than one session, with the first session covering just the topics needed to make immediate level-of-care decisions. In a follow-up session(s), when patients are likely to feel better both physically and emotionally, assess more sensitive issues and engage patients in self-reflection about their needs and goals. Third, as part of quality monitoring and improvement at SUD treatment centers, routinely assess patients’ experiences with the intake assessments and adjust the process based on the feedback. Also, patient and family advisory groups can provide valuable input on how to make the intake assessment patient-centered.
For providers, when conducting intake assessments use a patient-centered approach to begin building a therapeutic alliance with the patient. Important elements of patient-centeredness that can help develop alliance include respect for the patient's needs, preferences, and values; emotional support; and communication and information that is attentive, responsive, and tailored to the individual patient. 9
Finally, for researchers, examine how different features of the SUD intake assessment process, including who conducts the assessment and the timing of assessment sessions, affect key patient outcomes such as treatment retention.
Footnotes
Disclosure statement
None of the authors report a conflict of interest. The results and conclusions presented in this article are solely the responsibility of the authors and do not necessarily represent the views of the Patient-Centered Outcomes Research Institute® (PCORI®), its Board of Governors, or Methodology Committee.
Funding
The research reported in this study was funded through a Patient-Centered Outcomes Research InstituteVR (PCORIVR) Award (IHS-2017C1-6371). PCORI was not involved in preparation of this manuscript.
Author contributions
Drs. Mark and Padwa are co-PIs on the overall study and developed the research concept and design. Drs. Treiman and Padwa co-led the client interview data collection and analysis, with analytic support from J. Tzeng and M. Gilbert. All authors were involved in interpretation of findings. Dr. Treiman led development of the manuscript with substantial conceptual and writing contributions from Drs. Mark and Padwa. J. Tzeng also contributed to writing the manuscript. All authors reviewed and approved the final manuscript
Data availability statement
Study data are not publicly available because personal health information is included.