
Abstract
Background
Efforts to reduce the risk of opioid misuse are often focused on reducing unnecessary prescriptions for opioid medications or reducing the dose prescribed; however, not all misuse occurs in individuals with a personal prescription. This study examined trends in the proportion of adolescents and young adults (AYAs) who had an opioid-related problem (ORP) and who also had a personal opioid prescription drug claim or had a family member with an opioid prescription drug claim prior to the ORP diagnosis.
Methods
A retrospective cohort design was used to analyze longitudinal claims data. We identified individuals aged 12 to 25 years who had a newly diagnosed ORP in the years 2006 to 2014. Trends over time in personal or family opioid prescription drug claims within 1 year prior to ORP diagnosis were examined.
Results
We identified 53,560 AYAs with an ORP diagnosis. Over the entire study period, 40% of AYAs with an ORP diagnosis had a personal opioid prescription in the year prior to diagnosis, and 48% had a family member with an opioid prescription in the prior year. While the proportion of AYAs with a family prescription remained constant, the proportion with a personal prescription fell from 77.1% in 2006 to 27.3% in 2014.
Conclusions
The number of AYAs with an ORP increased over time, yet the proportion with a personal opioid prescription claim prior to their diagnosis decreased over time. This suggests that providers are paying greater attention to prescribing opioids to AYAs directly, although prescriptions to family members may still remain a point of access.
Introduction
Opioids are frequently prescribed to adolescents and young adults (AYAs), 1 leading to increased risk of misuse. 2 , 3 In 2014, there were an estimated 467,000 adolescents aged 12 to 17 and 978,000 young adults aged 18 to 25 who were nonmedical opioid analgesic users in the US, 4 and many of the AYAs who misuse opioids later switch to heroin. 5 Efforts to reduce the risk of opioid misuse are often focused on reducing unnecessary prescriptions for opioid medications or reducing the dose prescribed 6 ; however, not all misuse occurs in individuals with a personal prescription. 7 While studies have found that family member prescriptions are a risk factor for overdose among AYAs, 8 , 9 and the major source of prescription opioids for AYAs is through friends and relatives for free, 10 no studies to our knowledge have examined how rates of personal and family member opioid prescriptions among AYAs with opioid-related problems (ORPs) have changed over time. This study examines trends in the proportion of privately insured AYAs with an ORP who also had a personal opioid prescription drug claim or had a family member with an opioid prescription drug claim prior to ORP diagnosis. Insights about these trends in opioid access can inform the need for evaluating alternative policies targeting opioid prescribing to youth vs excess prescribing to the population in general, potentially allowing resources to be used more strategically to mitigate the epidemic of opioid misuse.
Methods
A retrospective cohort design was used to analyze longitudinal claims data from the MarketScan® Commercial Claims and Encounters database (MarketScan). MarketScan consists of reimbursed health care claims for employees and their dependents of more than 250 medium and large employers and health plans throughout the United States. The database includes claims information from more than 130 payers and describes the health care service use and expenditures for more than 28 million covered employees and family members per year. The database is divided into subsections, including inpatient claims, outpatient claims, outpatient prescription drug claims, and enrollment information. Claims data in each of the subsections include de-identified information on patient age, sex, geographic location, and type of health plan.
We identified individuals aged 12 to 25 years who had a newly diagnosed ORP in the years 2006 to 2014. An ORP was defined as an International Classification of Diseases, Ninth Revision (ICD-9) diagnosis code for opioid abuse or dependence alone or in combination with other drugs (304.0x, 304.7x, and 305.5x excluding 304.03, 304.73, and 305.53) or external cause of injury codes (E codes) for accidental poisoning by opium, methadone, heroin, opiates, and related narcotics (965.00–965.09; E850.0–E850.2). To identify newly diagnosed problems, we excluded AYAs who had not been continuously enrolled 1 year prior to their earliest identified ORP diagnosis and those who had another diagnosis of an ORP during that 1-year period. The prescription drug claims of these individuals, as well as those of their family members enrolled under the same insurance plan, were examined to determine whether the AYA or family member had at least 1 opioid prescription claim within 1 year prior to a new ORP diagnosis. Opioid prescriptions were identified in the prescription drug claim files using National Drug Code numbers. Individuals were identified using a unique 11-digit patient identifier made up of two sections: The first nine digits identified a unique family, and the last two digits identified individuals within the family. Trends over time in personal or family prescriptions were examined. The Penn State College of Medicine Institutional Review Board approved this study.
Results
We identified 53,560 AYAs aged 12 to 25 with an ORP diagnosis in the 2006–2014 data. Over the entire study period, 40% of AYAs with an ORP diagnosis had a personal opioid prescription in the year prior to diagnosis, and 48% had a family member with an opioid prescription in the prior year. However, we found considerable changes in these percentages over time. From 2006 to 2014, there was a 25–percentage point increase in AYAs without a personal or family opioid prescription prior to ORP diagnosis (Table 1). While the proportion of AYAs with a family prescription remained constant, the proportion with a personal prescription fell dramatically from 77.1% in 2006 to 27.3% in 2014 (Figure 1).
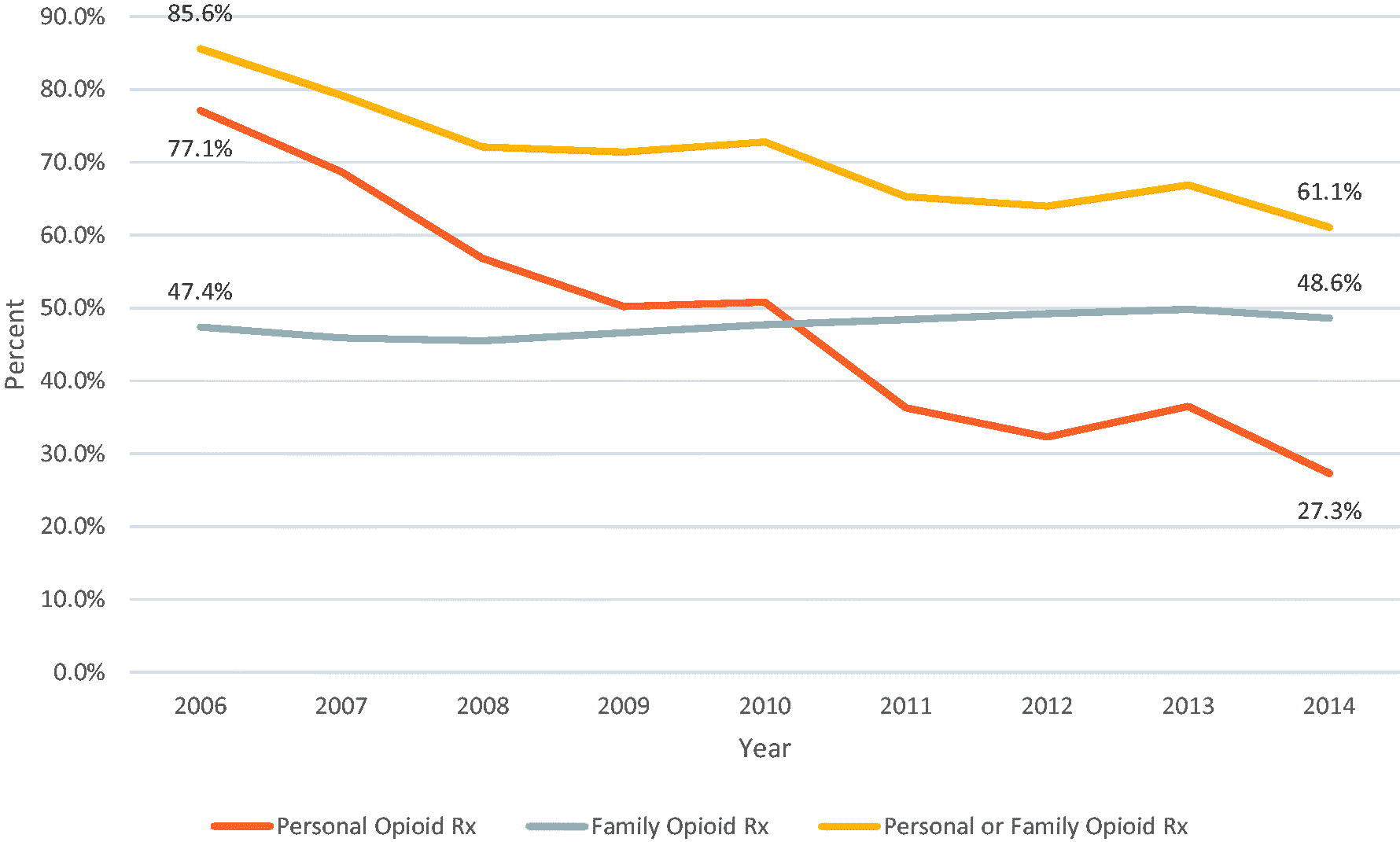
Trends in the percentages of adolescents and young adults with an opioid-related problem who had a personal or family member opioid prescription within a year prior to diagnosis, 2006–2014.
Trends in opioid prescriptions prior to a diagnosis of an opioid-related problem (ORP).

Within the year before initial ORP diagnosis.
Personal: Adolescent had a personal opioid prescription; family: adolescent had at least one family member with an opioid prescription; personal/family: adolescent had a personal opioid prescription or at least one family member with an opioid prescription or both.
Discussion
We found that the number of AYAs with an ORP in MarketScan increased 6-fold between 2006 and 2014, yet the proportion with a personal opioid prescription claim prior to their diagnosis decreased considerably over time. This suggests that providers are paying greater attention to prescribing opioids to AYAs directly, although prescriptions to family members may still remain a point of access. These findings must be considered within the context of the study's limitations, including being limited to privately insured AYAs and family members (no Medicaid or Medicare data are included) and the possibility of missing family prescriptions if a family member is enrolled in a different insurance plan. Furthermore, we were only able to identify incident diagnosis of ORP and not overall incidence. Nonetheless, study results suggest that in-home access to prescription opioids, while still high, is declining and that a growing number of adolescents appear to be obtaining opioids via means other than personal or family prescriptions, even with the rate of family member prescriptions remaining constant. Future research on opioid use among AYAs needs to better understand the alternative sources and types of opioids used as well as the role state policies may have played in these trends.
Footnotes
Disclosure statement
RP reports funding from the National Institute on Drug Abuse, the National Institute of Mental Health, and the Centers for Disease Control. AD reports funding from the National Institute of Mental Health, National Institute on Drug Abuse, and the Agency for Healthcare Research and Quality. BS reports funding from the National Institute on Drug Abuse, National Institute of Mental Health, National Institute of Dental and Craniofacial Research, Substance Abuse and Mental Health Services Administration, Pew Charitable Trusts, Glade Run Lutheran Foundation, and Brookings Institution. DL reports funding from the National Institute of Mental Health, the Agency for Healthcare Research and Quality, Department of Health and Human Services/Substance Abuse and Mental Health Services Administration, Eglet Adams, and Simon Greenstone Panatier. BD and AC has no conflicts to disclose.
Author contributions
AC and DL conceptualized and designed the study, drafted the initial manuscript, and reviewed and revised the manuscript. AC collected data and carried out the initial analyses. DL supervised data collection and analysis. All authors, AC, RP, AD, BS, BD, and DL, assisted with data interpretation, reviewed the manuscript for important intellectual content and approved the final manuscript as submitted.
Funding
All phases of this study were supported by a grant [R01DA047396] from the National Institute on Drug Abuse (NIDA). NIDA had no further role in the study design; in the collection, analysis and interpretation of data; in the writing of the report; or in the decision to submit the paper for publication.