
Abstract
Background
The Centers for Disease Control and Prevention's Prevention for States (PfS) program funded 29 state health departments to prevent opioid overdose by implementing evidence-based prevention strategies. The objectives of this analysis were to describe the scope of activities implemented across the four PfS strategies and identify implementation challenges.
Methods
PfS recipients submitted annual progress reports (APRs) to state support staff at CDC from 2015 to 2017. APR data were used to calculate the number of required and optional activities implemented under each PfS strategy. APR data were qualitatively analyzed using a systematic content analysis approach to identify key implementation challenges.
Results
From 2015 to 2017, PfS recipients implemented 177 activities across four strategies from 2015 to 2017. Cross-cutting implementation challenges were (1) multi-sector collaboration, (2) lack of knowledge and misperceptions about opioid used disorder (OUD) among some partners and local communities and; (3) management and access to opioid data among PfS recipients.
Conclusions
PfS recipients implemented an array of prevention interventions to address the opioid overdose crisis and encountered several cross-cutting implementation challenges. Challenges and state driven solutions over the course of implementing PfS led to several lessons learned and actions that CDC enacted to continue to support and expand overdose prevention.
Introduction
Opioid overdose is a major public health crisis requiring action at the federal, state and community levels. In 2018, approximately 10.3 million individuals misused an opioid and an additional 2.0 million had opioid use disorder (OUD). 1 Additionally in 2018, 67, 367 individuals died from a prescription opioid overdose. 2 Although deaths involving prescription opioids were stable at a rate of 5.2 per 100,000 at the national level, they remained high. 2 Prevention programs are imperative to decreasing opioid misuse and overdose.
At the federal level, the US Department of Health and Human Services implemented numerous initiatives to address the US opioid crisis. 3 , 4 The Substance Abuse and Mental Health Services Administration (SAMHSA) State Targeted Response (STR) and State Opioid Response (SOR) are federal programs that provided state and local level funding to increase access to medication-assisted treatment and recovery activities for opioid use disorder. 5 , 6 The CDC's Prevention for States (PfS) program (https://www.cdc.gov/drugoverdose/states/state_prevention.html) provided state-level funding to health departments (recipients) with support and technical assistance needed to advance interventions for preventing opioid overdoses. 4 , 7 The PfS program built upon evidence gathered from CDC's: Prescription Drug Overdose: Boost for State Prevention, which funded five states in 2014 that had the highest burden of opioid morbidity and mortality. Lessons learned from Boost for State Prevention emphasized the importance of investing in prescription drug monitoring programs (PDMPs) and engaging local communities. Thus, these lessons learned from Boost for State Prevention were required activities in the subsequent PfS funding for opioid prevention.
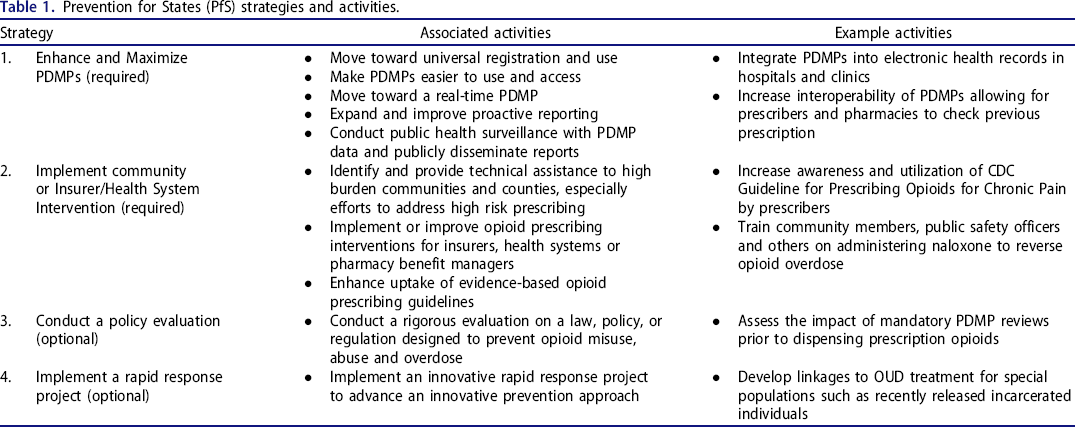
The PfS program provided funding for opioid overdose prevention strategies for states most impacted with the goal of expanding the scope and reach of opioid overdose prevention activities beyond the five state health departments from the previous Boost for State Prevention. PfS was a 4-year cooperative agreement initially funding 16 state health departments in 2015 and an additional 13 state health departments in 2016. The goals of PfS were to (1) decrease rates of opioid misuse and abuse; (2) increase OUD treatment; (3) decrease rates of emergency department visits related to opioids; (4) decrease opioid overdose death rates and; (5) improve health outcomes in state “hot spots.” To achieve these goals, PfS funded state health departments to implement two required prevention strategies: to enhance and maximize PDMPs (Strategy 1) and to implement community or insurer/health system interventions (Strategy 2). There were also two optional strategies: to conduct policy evaluations to assess the impact of state laws, regulations, policies and practices on overdose prevention outcomes (Strategy 3) and to conduct rapid response projects to advance innovative prevention approaches (Strategy 4). These strategies were chosen based on evidence learned through implementing the BOOST program and a systematic review that identified promising interventions to improve opioid overdose.
More comprehensive descriptions and dissemination of state experiences implementing opioid overdose programs and their impact are needed to inform the prevention and response initiatives of other states and federal agencies and prevent replication of prevention efforts with minimal impact. 8 State health departments funded by CDC through PfS implemented a variety of prevention activities that they could select from an evidence-based menu to address opioid overdoses within the unique context of their state. For example, states used PfS funding: to evaluate the effectiveness of a state-level policy mandate for clinicians to review the PDMP before prescribing opioids; to assess barriers to naloxone use; to measure community readiness to address opioid overdoses; and to develop linkages of individuals to substance use disorder treatment facilities for OUD. 9 – 11 The objectives of this analysis were to describe the scope of activities implemented across all PfS funded states to address the opioid overdose crisis, identify shared implementation challenges across the four PfS prevention strategies, discuss state-based solutions to challenges and conclude with lessons learned from the challenges that CDC acted upon.
Methods
The PfS program funded a total of 29 state health departments or their bona fide agents (recipients) to address opioid overdose through four strategies and associated activities (Table 1). PfS recipients submitted annual progress reports (APRs) to CDC from 2015 to 2017, which captured data from the previous year related to specific performance measures, start and end dates of activities, successes, challenges and other administrative milestones for each budget period. Recipients submitted their APR data to CDC, who then compiled these data into a single database. The APR database was used to create an activities inventory, which qualitatively describes common elements across the reported activities, allowing comparisons across recipients. The activities inventory captured data from 2015 to 2017. Table 1 lists the four major strategies and example activities for each major strategy. To tally the scope of activities implemented under each strategy, CDC scientists reviewed the activities inventory.
Prevention for States (PfS) strategies and activities.
Using the APR database, this analysis also qualitatively analyzed implementation challenges reported by recipients. The APR data captured implementation challenges from September 2017 to November 2018, when PfS recipients submitted the APR data to CDC. Specifically, PfS recipients could provide narrative responses in their APRs to the following question: What challenges, if any, did you encounter with Strategy #1 PDMPs? If applicable, please provide detail regarding administrative impediments, staffing impediments, or any other impediments to program implementation. This question about challenges and request for additional details was asked for each of the four PfS strategies. Of the 29 PfS recipients that submitted APRs in November 2018 reporting challenges going back to September 2017, 28 reported challenges related to implementing programmatic activities. The implementation challenges for each of the 28 recipients were extracted from the APR database and compiled in a Microsoft Excel spreadsheet.
Using the Microsoft Excel spreadsheet with implementation challenges data, the team conducted systematic content analysis, using an iterative thematic approach to code and identify key implementation challenges. 12 Four team members independently reviewed and coded all of the implementation challenges, followed by regular team discussions to identify issues, clarify themes, and develop an agreed upon coding framework through an analytic and iterative process. 12 After finalizing the coding framework, team members recoded the data by segmenting text and assigning appropriate codes to a segment. Coding was cross-checked by other team members and discrepancies were resolved through discussion and consensus. 12 The resulting codes provide insight about key implementation challenges across recipients. Quotations are included to characterize shared sentiments and issues among recipients. The authors removed identifying information such as the names of recipients, specific coalitions or partners to protect the identity of recipients. The CDC determined this project was except from institutional review board approval and informed consent was not needed.
Results
PfS implemented activities
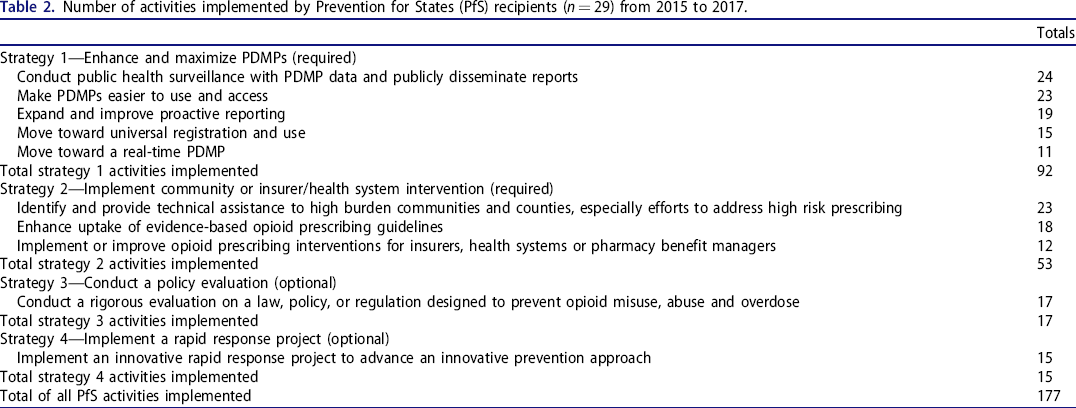
Twenty-eight PfS recipients implemented 177 activities across four major strategies from 2015 to 2017 (Table 2). The majority of activities were implemented for Strategy 1 (N = 92, 52%), followed by Strategy 2 (N = 53, 30%), Strategy 3 (N = 17, 10%) and Strategy 4 (N = 15, 8%). For Strategy 1, activity 5 (conduct public health surveillance with PDMP data and publicly disseminate) was the most widely implemented activity (n = 23) and for Strategy 2, activity 1 (identify and provide technical assistance to high-burden communities and counties) was the most widely implemented activity (n = 23) across all funded recipients. Although Strategy 3 (conduct a rigorous evaluation on a law, policy, or regulation to prevent opioid overuse, misuse, abuse, or overdose) and Strategy 4 (implement an innovative rapid response project) were optional and did not require implementation of specified activities, there were 17 policy reviews (Strategy 3) and 15 rapid response projects (Strategy 4) implemented.
Number of activities implemented by Prevention for States (PfS) recipients (n = 29) from 2015 to 2017.
Cross cutting implementation challenges
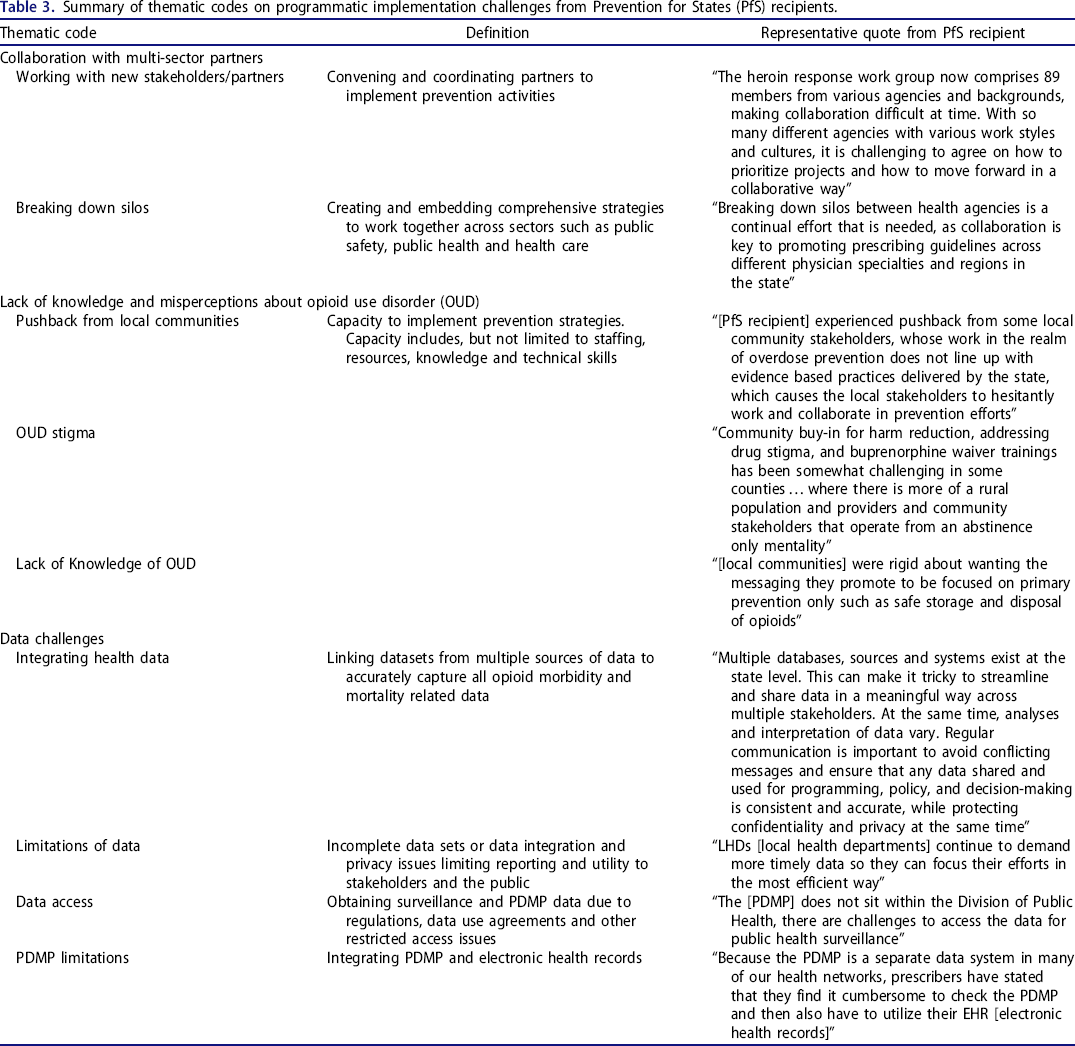
CDC identified several crosscutting implementation challenges across the PfS strategies and activities. The major codes or themes that emerged were (1) collaboration challenges with multi-sector partners, (2) lack of knowledge and misperceptions about OUD among some partners and local communities and (3) navigating opioid data from multiple sources among PfS recipients. There were several sub codes or sub-themes, which are detailed below. Table 3 includes subcode definitions and a representative quote.
Summary of thematic codes on programmatic implementation challenges from Prevention for States (PfS) recipients.
Collaboration with multi-sector partners
PfS recipients reported that collaboration with multi-sector partners was challenging. Specifically, these challenges included working with new partners and stakeholders in different sectors, breaking down silos and implementation delays. The first challenge identified was difficulty working beyond the typical public health sectors with new partners such as law enforcement, licensing boards and emergency medical services (EMS). PfS recipients also expanded their work with emergency departments, physicians, hospitals, public safety, pharmacists, behavioral health, and health insurers to implement activities to decrease morbidity and mortality associated with opioid overdose, which impacted multiple sectors. Specifically, activities associated with Strategy 1 (enhance and maximize PDMP) and Strategy 2 (implement community or insurer/health systems interventions) pushed recipients to engage with new, multi-sector partners to improve prescribing of prescription opioids. An increased number of stakeholders created communication challenges and difficulties navigating competing priorities and responsibilities among diverse partners. One recipient noted that, “some local groups have expressed that the issues arising from the opioid epidemic should be handled at a local level and that the state should not play a role, while other local groups have expressed that the state should provide additional funding and aid [to the local level].”
Engaging partners across multiple sectors (e.g., public health, licensing boards, healthcare systems, public safety and the judicial system) to address the opioid overdose crisis created collaboration challenges. Breaking down organizational silos was another cross-cutting collaboration challenge PfS recipients encountered. One recipient echoed a common theme and noted the difficulties working across different organizations, “Breaking down silos between health agencies is a continual effort that is needed, as collaboration is key to promoting prescribing guidelines across different physician specialties and regions in the state”, while another noted that,
the heroin response work group now comprises 89 members from various agencies and backgrounds, making collaboration difficult at time[s]. With so many different agencies with various work styles and cultures, it is challenging to agree on how to prioritize projects and how to move forward in a collaborative way.
Breaking down silos was important to this work because several PfS strategies and activities specifically required work with PDMPs, clinicians, communities, law enforcement and a variety of other partners to comprehensively address opioid overdose.
Lack of knowledge and misperceptions about OUD
In addition to silos, lack of knowledge and misperception about OUD among some partners and local communities caused implementation delays. Because PfS recipients at the state level were required to work with local communities, they were able to learn more about knowledge gaps and potential stigma associated with OUD among their local partners. For example, knowledge gaps included general substance misuse subject matter, strategies to message prevention of overdose versus harm reduction and ensuring implementation of evidence-based practices. Stigma associated with OUD was a challenge. PfS recipients noted that, “community buy-in for harm reduction, addressing drug stigma, and buprenorphine waiver trainings has been somewhat challenging in some counties [identifying information removed] where there is more of a rural population and providers and community stakeholders that operate from an abstinence only mentality” and
Another challenge has been in addressing the ongoing myths and misconceptions associated with buprenorphine prescribing and the strenuous process providers must go through to prescribe buprenorphine….this is addressed during all trainings; however, in speaking throughout some counties and regions, the DOH [department of health] team has been met with resistance or disagreement to our effort in buprenorphine expansion, and this will continue to be a problem as the team works on addressing stigma associate with drug use and treatment
Navigating and accessing opioid data
PfS recipients faced and continue to grapple with complex and multifaceted data issues to address the opioid overdose crisis. Specifically, challenges with opioid data were integrating data from multiple sources, limitations of existing data, data access and limitations with PDMP specific data. PfS recipients not only relied on traditional public health morbidity and mortality surveillance systems, but also captured new types of data due to the nature of the epidemic. Recipients collected data from various health information systems such as coroner or medical examiner reports, pharmacy dispensing and hospital billing information from multiple sources and merged them to capture accurate data on opioid prescribing rates, morbidity and mortality associated with opioids. One recipient noted the difficulties that gathering, capturing and reconciling so much data created,
multiple databases, sources and systems exist at the state level. This can make it tricky to streamline and share data in a meaningful way across multiple stakeholders. At the same time, analyses and interpretation of data vary. Regular communication is important to avoid conflicting messages and ensure that any data shared and used for programming, policy, and decision-making is consistent and accurate, while protecting confidentiality and privacy at the same time
Integration of data from electronic health records (EHR), medical billing data, and death records was complex and caused implementation delays of several required PfS strategies and activities. For example, one recipient reported “challenges associated with developing, updating and integrating a complex IT system, and gaining approval for facets of data use and data sharing, as well as a lengthy and often multi-layered approval process, has caused delays.” Many of these data systems existed independently, but PfS recipients were now building unique data systems to merge independent data sources to communicate and share data about prescription opioid prescribing and dispensing along with fatal and non-fatal overdoses.
Another major challenge PfS recipients encountered was the inadequacy of collected data. Existing data was inadequate due to its inability to meet the needs of stakeholders to implement community interventions (Strategy 2), enhance PDMPs (Strategy 1) and conduct rapid response projects (Strategy 4). Due to the nature of the epidemic, there was increased demand for more rapid data to improve prescribing of prescription opioids and prevent overdose deaths. Several recipients expressed that, “LHDs [local health departments] continue to demand more timely data so they can focus their efforts in the most efficient way.”
PDMP data is complex and created numerous challenges for PfS recipients. Additional PDMP challenges were underutilization of the PDMP by providers and prescribers, limitations with collecting specific data fields and reporting, difficulties with access to PDMP data and PDMP integration within states and across states. Underutilization of PDMPs by prescribers and pharmacists was a challenge that slowed progress associated with Strategy 1 (enhance and maximize PDMPs). PfS recipients often relied on PDMP data to guide many of their prevention efforts and identify high dose prescribers to provide additional education and training. Some PfS recipients identified low registration of prescribers and pharmacists as a common challenge. For example, one recipient noted, “getting prescribers and dispensers to understand the importance of registering and utilizing the PDMP when providing care for patients has been difficult.” Additionally, limited registration and use of PDMPs by prescribers and pharmacists prevented recipients from accurately capturing volume of opioids prescribed and identifying areas with elevated numbers of dispensed prescriptions.
Additionally, PfS recipients faced challenges with collecting PDMP specific data fields and reporting specific data back to stakeholders due to limited participation and lack of mandatory registration of prescribers in PDMPs, regulations on sharing health information, delays in receiving data and the need to protect patient and prescriber privacy. For example, PfS recipients noted that prescribers wanted the, “[PDMP] data to be able to benchmark themselves against their peers to see where their prescribing habits really are against others in the same specialty and areas of the state”, but “the biggest challenge is the inability to collect clinical specialty data to compare across a single discipline.” Some PfS recipients were unable to collect that data in their PDMP system or legally could not extract that data from the information system to distribute widely.
PDMP integration into electronic health records within a single state with different hospital systems (intrastate integration) and across state lines (interstate integration) was a challenge that numerous PfS recipients reported. Prescribers reported to PfS recipients that, “because the PDMP is a separate data system in many of our health networks, prescribers have stated that they find it cumbersome to check the PDMP and then also have to utilize their EHR” and “one limitation of the PDMP integration project is providers are not able to see prescription data from all states when they sign-in to the system.” The lack of a completely integrated system of PDMPs into EHRs within a state's medical system and an inability of prescribers to check the PDMP across state lines contributed to underutilizations of PDMPs by prescribers. Laws requiring mandatory reporting by physicians and pharmacists varied by state, and the variation in these requirements also created data sharing challenges. One recipient reported that, “there were some issues with educating pharmacists on the new reporting timelines, especially out of state pharmacies that are located in a state that reports on a different schedule.”
Access to PDMP data was another common challenge. Several recipients identified limited access to PDMP data for public health surveillance because data stored in a different department, collected by different agencies, or inaccessible data from other states. As of July 2019, 18 states house the PDMP within the state health department, while 20 states house the PDMP within the state pharmacy board. 13 Other states housed their PDMPs with law enforcement agencies, professional licensing boards and substance abuse agencies. One recipient noted that, “the [PDMP] does not sit within the Division of Public Health, there are challenges to access the data for public health surveillance.” When recipients have direct access to PDMPs, challenges still arise with delays in receiving data for public health surveillance and prevention projects. Specifically, some PfS recipients are unable to get complete and usable datasets for reporting.
Discussion
This analysis described activities implemented by PfS recipients and the programmatic challenges encountered. The PfS program funded state health departments or their bona fide agent to implement different prevention strategies in an effort to address the opioid overdose crisis and the findings showed the vast range of activities implemented by the major strategies. PfS recipients implemented 15 innovative opioid overdose prevention activities that will contribute to the growing body of knowledge of opioid overdose prevention interventions.
There were three main implementation challenges identified from the APR data: (1) collaboration with multi-sector partners, (2) lack of knowledge and misperceptions about OUD among some partners and local communities and (3) navigating opioid data among PfS recipients. The remainder of the discussion recaps some implementation challenges and highlights state driven solutions that PfS recipients developed for each challenge to advance opioid overdose prevention in the unique context of their state. Finally, presented are lessons learned for CDC staff over the 3-year implementation period of the PfS program.
Our findings also showed that establishing and maintaining multisector collaborations was a major challenge. Recipients faced various collaboration challenges and the creation of advisory or work groups were opportunities to gather stakeholders to develop a state-wide strategy. 8 Collaboration with multi-sector partners and agencies is key to implementing opioid overdose prevention strategies. Many PfS recipients had to build trust among partners with competing priorities, institute group communication norms and negotiate the commitment of time-limited partners. 14 One methodology utilized to resolve this challenge was the development of capacity building plans, which identify actions, proposed activities and their alignment with PfS goals. As more jurisdictions continue to address the opioid overdose epidemic, a strategic or capacity building document can help guide partners in contributing to overall goals and priorities to address overdose prevention. Studies show that clearly articulated goals, roles and responsibilities impact the functionality of coalitions, which many PfS recipients convened. 15 ,16
As this epidemic evolves into one around polysubstance use, multisector partnerships need to continue to grow to fully address prevention efforts. One of the most promising collaborations is between public safety and public health and CDC is funding and supporting the advancement of these partnerships. Public health and public safety have largely had separate approaches to opioid overdose, yet the opioid overdose epidemic has encouraged the two disciplines to increase collaboration to prevent overdoses. These two disciplines have previously collaborated to address other public health issues such as bioterrorism and violence prevention. 17 , 18 The emerging partnerships between public health and public safety can be seen clearly in the development of data sharing models designed to help public safety and public health identify hotspots, overdoses and refer patients to local treatment centers. 19 – 21 Efforts by PfS recipients to increase trust and collaboration between public safety and public health continues to emerge as a promising method to decrease opioid overdose deaths. Judicial and corrections partners can further facilitate overdose prevention efforts within criminal justice settings. Many individuals with OUD end up in the judicial system without access to treatment while incarcerated and after release. 22 PfS recipients can develop partnerships to link individuals to medication-assisted treatment for opioid use disorder and other support services such as housing instead of incarceration.
PfS implementation barriers such as stigma and lack of knowledge among some partners and local communities present an opportunity for CDC to provide resources and increase capacity to address this public health issue. PfS recipients and future recipients working in opioid overdose prevention must be diligent about building the capacity of CBOs and addressing stigma in communities in order to implement opioid overdose prevention activities such as naloxone distribution. Similar to the HIV/AIDS epidemic, stigma is a significant barrier for individuals accessing medication assisted treatment and healthcare services, and creates difficulties in achieving buy-in from key stakeholders. 10 , 23 – 25 Countering stigmatizing beliefs with narratives that OUD can be managed effectively with medications is important to promote. One cross-sectional study found that healthcare providers had beliefs that people who use drugs or alcohol are making a choice or have a moral weakness separates this illness from other chronic diseases and may contribute to additional barriers, such as lack of access to treatment facilities, limited health insurance coverage and biases among healthcare providers. 26 Development of communications and media campaigns to increase knowledge about the opioid overdose epidemic and OUD has potential to increase buy-in from local communities and among healthcare providers.10
There are additional opportunities where CDC can support partners to build knowledge and skills through information sharing to decrease stigma associated with OUD. Studies assessing stigma associated with HIV/AIDS show that information together with skill building is more effective at raising knowledge levels and reducing stigmatizing attitudes compared with information alone. 10 , 25 If there are gaps, training healthcare, public safety officers, emergency medical service (EMS)/first responders in motivational interviewing along with equipping individuals such as teachers, family members, friends, social service workers and faith-based leaders to identify signs of an overdose and administer naloxone are ways to develop the skills in the community. Motivational interviewing is a type of counseling style utilizing constructive conversation to elicit behavior change originally developed to address addictive behavior such as excessive alcohol consumption. 27 It has since been adapted to address a range of health issues including substance use disorder and healthcare professionals often use it. 28 , 29 There is potential to adapt motivational interviewing techniques and train individuals in frequent contact with individuals with opioid use disorder to assess their readiness for behavior change such as utilizing harm reduction techniques or linkage to care.29
Finally, there were numerous challenges with navigating opioid data because it comes from so many different sources. PfS recipients noted numerous challenges focused on implementing activities associated with maximizing and enhancing PDMPs and integrating health information systems. This strategy required intense planning and complex implementation and coordination involving multiple sectors. Many PfS recipients made efforts to integrate PDMPs into clinical workflows and electronic health records, which required immense resources across sectors such as hospital systems, electronic health record vendors, and regulatory boards overseeing individual state PDMP systems. The goal of this multisector collaboration was often universal registration of prescribers and/or dispensers of prescription opioids to improve prescribing behaviors and prevent obtaining prescriptions from multiple doctors. Multisector collaborations at impactful levels are often difficult among multiple systems that were not designed to be integrated can be challenging. Collaborating with numerous partners is not new for PfS recipients; however, building the innovative health information systems that allow multiple prescribers and dispensers to communicate within the state and across state lines introduced new challenges.
At the beginning of the PfS program in 2015, the available evidence suggested that PDMPs were under-utilized yet had the potential to significantly impact vulnerable populations in regard to opioid overdose. 30 – 32 Nine PfS recipients implemented activities to move toward universal registration and use of PDMP systems by prescribers at the initiation of PfS in 2015 and currently only four PfS recipients have no mandatory reporting requirements. Furthermore, integrating PDMPs universally into existing electronic medical records and increasing interstate interoperability across state lines has the potential to decrease opioid misuse and overdose. 33 – 36 States continue to tackle the challenges associated with increasing the function and utilization of PDMPs and CDC continues to support this work through subsequent funding efforts. To continue addressing the opioid overdose epidemic, it is important that surveillance and clinical decision support tools increasingly and routinely incorporate PDMPs.
Limitations
There were several limitations to this analysis. First, not all PfS recipients noted programmatic challenges or solutions in their APR data, thus the data does not reflect the entire PfS program. PfS recipients had the option to provide as much or little information about challenges and solutions associated with each of the four major strategies. While many recipients did indicate challenges, CDC did not require recipients to submit this information. Many PfS recipients also received additional funding from other federal agencies, which could be leveraged to expand some of their work that impacted the number of PfS strategies and activities implemented. APR data submitted to CDC did not capture any additional federal or state funding used for opioid overdose prevention efforts.
Using challenges and lessons learned to guide next steps
There is still a significant amount of prevention work needed to address the evolving epidemic. This manuscript identifies cross-cutting prevention implementation challenges, solutions and lessons learned to advance the field. Based on the challenges and solutions PfS recipients presented, CDC had several lessons learned, which were manifested in the Overdose Data to Action cooperative agreement. Overdose Data to Action (OD2A) is a 3-year cooperative agreement beginning September 2019 that highlights a multisector and comprehensive approach to the overdose epidemic. This funding continues to support PDMP advancements such as inter and intra state operability and also allows recipients to implement innovative surveillance activities, which many PfS noted as challenges. Specifically, this funding requires submission of opioid surveillance data in shorter time periods allowing states to address the lack of timely data used for prevention purposes from many of their local communities. Additionally, PfS recipients emphasized the relationship between public safety, EMS, healthcare systems and public health. Thus, OD2A funds explicitly allow recipients to support public safety projects. 37 and linkages to care that aim to decrease opioid overdose. PfS recipients also noted challenges with implementing evidence-based programs in communities. As a result, technical assistance resources such as the “Evidence-Based Strategies for Preventing Opioid Overdose: What's Working in the United States” guide provides a list of evidence-based intervention that state health departments and local communities can select (https://www.cdc.gov/drugoverdose/policy/index.html). A technical assistance hub was also developed to streamline technical assistance resources and provide a warehouse of overdose prevention evidence based materials for recipients. OD2A funds also support peer to peer learning networks, in which jurisdictions implementing evidence-based work in opioid overdose prevention can teach and support other jurisdictions navigating this landscape. This is a unique opportunity for recipients to not only connect with each other to continue advancing prevention strategies but provide technical assistance and fuel innovative solutions to challenges. As the opioid overdose epidemic continues to evolve, implementation challenges will arise. State and local recipients remain nimble in developing strategies to overcome challenges, while raising awareness of these issues to CDC. CDC will continue to learn from the challenges and recipient driven solutions to ultimately improve funding mechanisms and advance evidence-based overdose prevention strategies.
Conclusions
The opioid overdose epidemic continues to affect people across the United States. Implementation of prevention strategies is critically important. This analysis shows that there was considerable effort by PfS recipients focused on PDMP and community/health systems interventions. PfS recipients expanded PDMPs in a variety of ways despite obstacles and pushed the work of engaging health systems, including insurers, prescribers and dispensers to new levels. Interventions focused on community and prescriber behaviors have the potential to improve prescribing of prescription opioids by physicians and include all community members in prevention efforts to decrease overdose morbidity and mortality. Although PfS recipients faced complex challenges, they implemented solutions to address this crisis. These solutions and the work PfS recipients implemented continue to advance the field to address an evolving epidemic. In a subsequent paper, we will examine how these efforts by recipients addressed the goals of PfS to decrease rates of opioid misuse, increase OUD treatment, decrease rates of emergency department visits related to opioids, decrease opioid overdose death rates, and improve health outcomes. Practitioners should continue to disseminate information about opioid overdose prevention interventions and implementation challenges to inform the efforts of other states to advance opioid overdose prevention efforts. Importantly, dissemination of resources and strategies to overcome those implementation challenges is greatly needed to address this critical issue.
Footnotes
Disclosure statement
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.