
Abstract
Background: Previous research has linked the internalization of shame and negative stereotypes associated with substance use to increased severity of substance use problems (i.e., negative consequences associated with alcohol and drug use, including occupational or relational difficulties and illegal behavior). However, little work has examined how other aspects of substance-use-related stigma (e.g., encounters with and anticipation of discrimination) might be related to the severity of substance use problems. Further, the psychological mechanisms through which stigma drives substance use problems remain poorly understood. Addressing these key limitations, the current study examined the role of executive functioning (EF) deficits in the relation between substance-use-related stigma and severity of substance use problems. Methods: In fall 2019, adults exposed to trauma who use substances were recruited via Amazon's Mechanical Turk (N = 320, 46.9% women) and completed self-report measures of substance-use-related stigma, EF deficits, and substance use problems. Results: Substance-use-related stigma was positively associated with EF deficits, which in turn related to substance use problems. Substance-use-related stigma was also indirectly associated with substance use problems through EF deficits, suggesting that EF deficits accounted for the significant association between substance-use-related stigma and substance use problems. Conclusions: These findings provide initial support for the role of EF deficits as a mechanism through which stigma drives substance use problems among individuals exposed to trauma. Results underscore the potential utility of addressing stigma coping and EF deficits in interventions aimed at preventing and treating substance use disorders.
Introduction
Substance use is highly prevalent in the United States, with approximately half of all people reporting past month alcohol use and nearly 15% reporting past month drug use. 1 A large number of these individuals − 20.2 million adults 2 – report symptoms consistent with a substance use disorder (SUD). SUDs remain one of the most stigmatized conditions compared to other physical and mental illnesses. 3 Across a number of studies, stigma (i.e., social devaluation and discrimination) has been identified as a major barrier to recovery among individuals with SUDs (see Kulesza et al., 4 for a review). In particular, the internalization of negative stereotypes and shame associated with substance use, such as the belief that people who use substances are untrustworthy and immoral, has been linked to increased severity of substance use problems among individuals receiving outpatient treatment for SUDs, 5 primary care patients diagnosed with SUDs, 6 and college students at risk for SUDs. 7
Despite a well-documented association between stigma and substance use problems, it is important to note that substance-use-related stigma (i.e., stigma associated with substance use) is a multifaceted construct that encompasses three interrelated processes: enacted stigma (i.e., experiences of stereotyping, prejudice, and discrimination from others in the past or present), anticipated stigma (i.e., expectations of stereotyping, prejudice, and discrimination from others in the future), and internalized stigma (i.e., endorsement and application of negative stereotypes to oneself). 8 Whereas internalized stigma has been consistently linked to increased severity of substance use problems in prior research, 5 – 7 few studies have examined the roles of enacted and anticipated stigma. Further, the psychological mechanisms through which stigma operates to drive substance use problems remain poorly understood. To this end, the present research examined the role of executive functioning (EF) deficits as a potential mechanism underlying the association between substance-use-related stigma and the severity of substance use problems among a community sample of adults exposed to trauma who use substances, a population known to be disproportionately at risk for developing SUDs. 9
EF deficits encompass dysfunction across five self-regulatory domains, including time management, self-organization and problem-solving, self-restraint, self-motivation, and self-regulation of emotions. 10 Although little research has examined the links among stigma, EF deficits, and substance use problems among people who use alcohol and/or drugs, existing work on other stigmatized groups provides support for these associations. Specifically, an emerging body of literature highlights the role of EF deficits as an important mechanism through which stigma operates to drive health risk behaviors such as substance use. As explained by Inzchlit et al., 11 chronic exposure to stigma-related stress can deplete executive resources, thereby undermining individuals’ ability to regulate their cognition and behaviors. Indeed, across a number of studies that span across racial/ethnic minorities, women, and people who are overweight, exposure to episodes of enacted or anticipated stigma associated with their respective marginalized identities (e.g., overhearing a stigmatizing comment, interacting with others who do not belong to one's stigmatized group, recalling past experiences of discrimination) has been linked to various indicators of EF deficits, including poorer attentional control, increased risky decision-making, and a greater willingness to engage in impulsive behaviors (e.g., aggression, overeating). 12 – 15
EF deficits have also been implicated in the development and perpetuation of substance use problems given their associations with behavioral and emotional regulation difficulties. Longitudinal studies, for example, have linked EF deficits to higher initial levels of substance use as well as increases in substance use over time. 16 , 17 Other cross-sectional studies also linked EF deficits to binge drinking and risky drug use. 18 , 19 Of particular relevance to the present study's focus on stigma, EF deficits have been identified as one of the key mediators underlying the association between experiences of racial discrimination (i.e., enacted stigma associated with one's race) and increases in tobacco, alcohol, and marijuana use among African Americans. 20 Taken together, these findings underscore the utility of examining EF deficits in the context of coping with substance-use-related stigma.
In the current study, we examined the associations among substance-use-related stigma, EF deficits, and severity of substance use problems among a community sample of adults exposed to trauma who currently use substances. We chose to focus on this target population given that individuals exposed to trauma are disproportionately at risk for SUDs 9 and other psychopathology associated with EF deficits (e.g., posttraumatic stress disorder, depression), 21 thus making them particularly vulnerable to the impact of stigma on EF and substance use. Recognizing that substance use can be stigmatizing even when it does not meet diagnostic criteria for SUDs, 8 we opted to include individuals with varying severities of substance use (ranging from use to probable SUD) in our sample. Further, consistent with previous research, 5 – 7 we operationalized substance use problems as the negative consequences associated with alcohol and drug use, including occupational or relational difficulties and illegal behavior. We hypothesized that substance-use-related stigma would be positively associated with EF deficits, which would in turn relate to substance use problems. We further hypothesized that substance-use-related stigma would be indirectly associated with substance use problems through EF deficits.
Methods
Participants and procedures
Data for the present study were collected in the fall of 2019 as part of a larger study examining co-occurring posttraumatic stress and substance use disorders. Participants were recruited from Amazon's Mechanical Turk (MTurk) platform, a crowdsourcing website that facilitates online data collection by allowing researchers to post a Human Intelligence Task (HIT), such as an online survey, that is available to qualified participants. MTurk allows for the rapid recruitment of large samples at relatively low costs, 22 offering a recruitment method that is both time and cost-efficient and capable of generating high quality data. 23 , 24
Participants were screened for the larger study on the basis of five inclusionary criteria: (1) aged 18 years or older; (2) living in North America; (3) working knowledge of the English language; (4) endorsed experiencing a traumatic event on the Primary Care PTSD Screen for DSM-5 25 (i.e., something that is unusually or especially frightening, horrible, or traumatic, such as a serious accident or fire, a physical or sexual assault or abuse, an earthquake or flood, a war, seeing someone be killed or seriously injured, or having a loved one die through homicide or suicide) in their lifetime; and (5) endorsed at least one instance of substance use in the 30 days prior to survey completion. Participants who met eligibility criteria provided informed consent and completed the survey on Qualtrics data collection platform. Participants were compensated $2.50 USD for study participation. All procedures were approved by the University of Rhode Island Institutional Review Board prior to beginning data collection.
Measures
Substance-use-related stigma
The Substance Use Stigma Mechanisms Scale (SU-SMS) 8 is an 18-item validated self-report measure that assesses experiences of substance-use-related stigma across three subscales: enacted stigma (six items; e.g., “family members have looked down on me”), anticipated stigma (six items; e.g., “family members will think that I cannot be trusted”), and internalized stigma (six items; e.g., “having used alcohol and/or drugs makes me feel unclean”). Participants rate each item on a five-point scale from 1 = never to 5 = very often; item scores are averaged to create subscale composite scores, with higher scores indicating more substance-use-related stigma. The SU-SMS has demonstrated good internal consistency, structural validity, and convergent validity, 8 and Cronbach's αs in the current sample were 0.92, 0.93, and 0.95 for the enacted, anticipated, and internalized stigma subscales, respectively.
Executive functioning (EF)
The Barkley Deficits in Executive Functioning Scale – Short Form (BDEFS-SF 26 ) is a 20-item validated self-report measure that assesses problems related to EF across five subscales: time-management (four items; e.g., “procrastinate or put off doing things until the last minute”), self-organization/problem solving (four items; e.g., “have difficulty explaining things in their proper order or sequence”), self-restraint (four items; e.g., “make impulsive comments to others”), self-motivation (four items; e.g., “others tell me I am lazy or unmotivated”), and self-regulation of emotions (four items; e.g., “I remain emotional or upset longer than others”). Participants rate each item on a four-point scale from 1 = never to 4 = very often; respective item scores are summed to create total scores for each subscale, with higher scores indicating greater EF deficits. The BDEFS-SF has been found to align well with the long form of the BDEFS 10 and to have adequate psychometric properties. 27 , 28 Cronbach's αs in the current sample were 0.89, 0.87, 0.87, 0.87, and 0.92 for the time-management, self-organization, self-restraint, self-motivation, and self-regulation subscales, respectively.
Substance use problems
The Alcohol Use Disorder Identification Test (AUDIT) 29 is a 10-item self-report measure assessing alcohol consumption, drinking behaviors, adverse reactions to drinking, and alcohol-related problems. Participants rate each item on a scale ranging from 0 = never to 4 = daily or almost daily, and items are summed to create a total scale score. Scores of 8 or higher indicate hazardous or harmful patterns of alcohol use. While the AUDIT was initially developed as a screener to detect hazardous alcohol use, it has been widely used in extant literature as a continuous variable, with higher scores reflecting greater severity of alcohol use problems or greater likelihood of hazardous or harmful drinking. 30 In the present study, we treat the AUDIT as a continuous variable, with higher scores reflecting greater severity of alcohol use problems. The AUDIT has demonstrated good psychometric properties, 29 , 30 including when used as a continuous severity rating, 31 and Cronbach's α in the current sample was 0.90.
The Drug Abuse Screening Test (DAST-10) 32 is a 10-item measure that assesses the presence of problems related to drug use, such as occupational or relational problems, illegal activities, or regret. Participants rate whether they have experienced each problem with response options 0 = no and 1 = yes, and items are summed to create a total scale score. Scores of 3 or higher indicate hazardous or harmful patterns of drug use. While the DAST-10 was originally developed as a screener to detect hazardous drug use, it has been widely used as a continuous variable reflecting a quantitative index of severity of problems related to drug use. 32 In the present study, we treat the DAST-10 as a continuous variable, with higher scores reflecting greater severity of drug use problems. The DAST-10 has demonstrated good psychometric properties, and Cronbach's α in the current sample was 0.82.
Data analysis
As recommended by Tabachnick and Fidell, 33 all study variables were assessed for assumptions of normality. Next, in IBM SPSS version 26, Pearson product-moment correlations were calculated among the primary study variables to explore their bivariate associations. Finally, in Mplus version 7.1, structural equation modeling was used to examine whether EF deficits indirectly explained the relation between substance-use-related stigma and substance use problems. Substance-use-related stigma was modeled as a latent (exogenous) variable measured with the three SU-SMS subscales (i.e., enacted, anticipated, and internalized stigma), EF deficits was modeled as a latent (endogenous) variable measured with the five BDEFS-SF subscales (i.e., time-management, self-organization/problem solving, self-restraint, self-motivation, and self-regulation of emotions), and substance use problems was modeled as a latent (endogenous) variable measured with the AUDIT (i.e., alcohol use problems) and DAST-10 (i.e., drug use problems).
Overall model fit was assessed using the likelihood ratio test based on the chi-square value, which assesses the magnitude of difference between the observed and proposed covariance matrices. 34 A nonsignificant likelihood ratio test indicates good model fit. However, because the chi-square test rejects even adequately fitting models, 35 fit indices based on the chi-square distribution were also used to assess model fit. Agreement among fit indices provides evidence that at least adequate model fit has been achieved. The comparative fit index (CFI) 35 , an incremental fit index, assessed fit relative to a null model (e.g., a model with all variables uncorrelated); CFI values greater than 0.95 indicated good model fit. The root mean square error of approximation (RMSEA) 36 with accompanying 90% confidence intervals (CIs) assessed closeness of fit, with values less than 0.05 indicating good fit and less than 0.10 indicating adequate fit. The standardized root mean square residual (SRMR) is the standardized difference between the observed and predicted covariance matrices, with values closer to zero indicating better fit and values less than 0.08 considered acceptable. 34 The bootstrap method was used to estimate the standard error of parameter estimates and bias-corrected confidence intervals of the indirect effects. 37 In this study, 1,000 bootstrap samples were used to derive estimates of the indirect effect. To confirm the directionality of the indirect effects, we also tested an alternative model in which substance use problems is posited to influence substance-use-related stigma through EF deficits.
Results
Of the obtained 951 responses, 392 were excluded for not meeting one or more inclusionary criteria (remaining n = 559). We then excluded 172 participants (remaining n = 387) who failed to respond correctly to any of the four validity checks interspersed throughout the survey to ensure attentive responding (three items; e.g., participants were asked to rate “I am paid biweekly by leprechauns” on a six-point scale from “strongly disagree” to “strongly agree”) and comprehension (one item asking participants to click on a small blue circle rather than the scale with items labeled from 1 to 5 38 , 39 ), as well as 67 participants who attempted to complete the survey more than once. Thus, the final sample included in the present study was 320 participants (Mage = 35.79, 46.9% women, 81.6% White). See Figure 1 for a schematic flowchart and Table 1 for further sample characteristics.
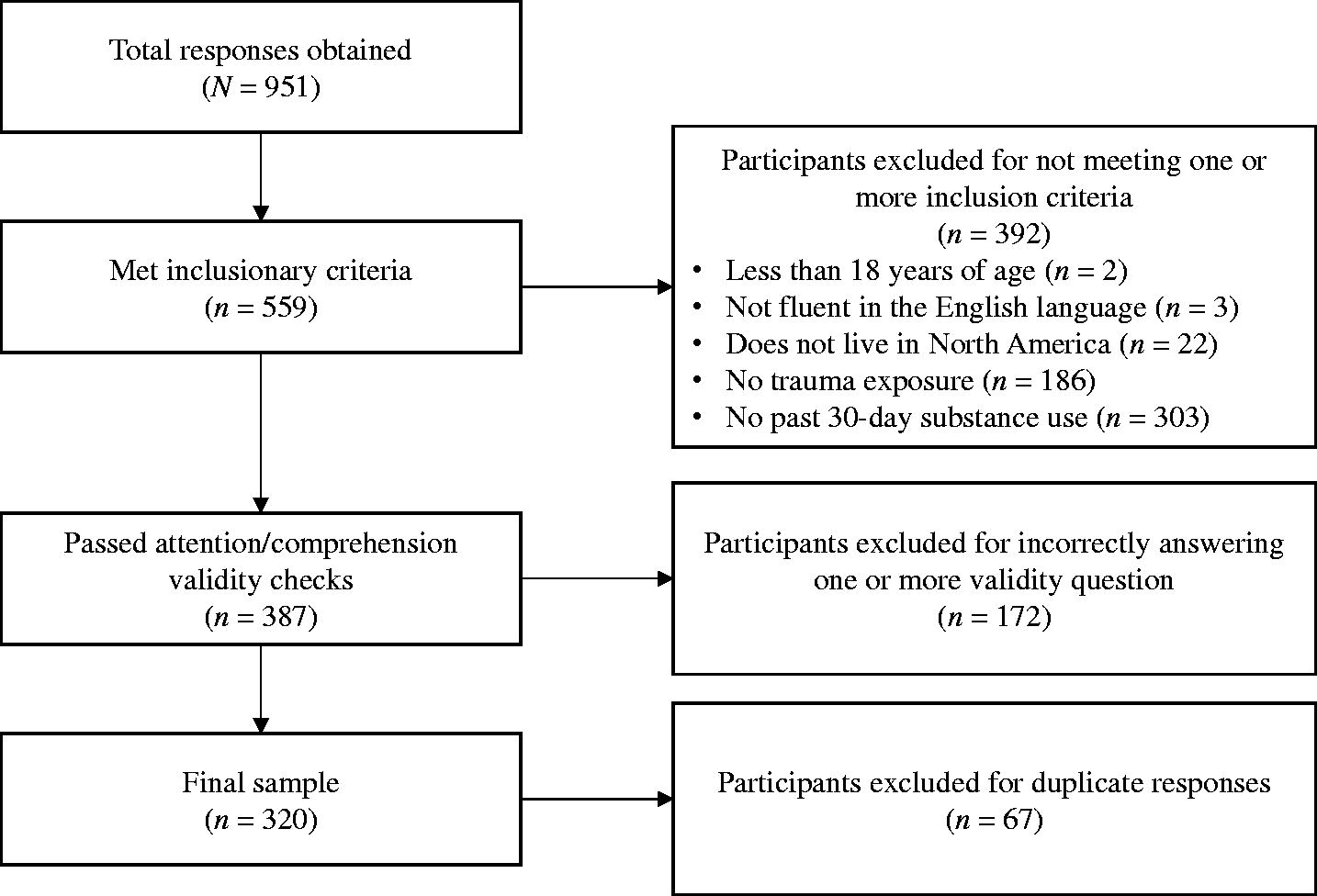
Flowchart for sample selection.
Sample characteristics.
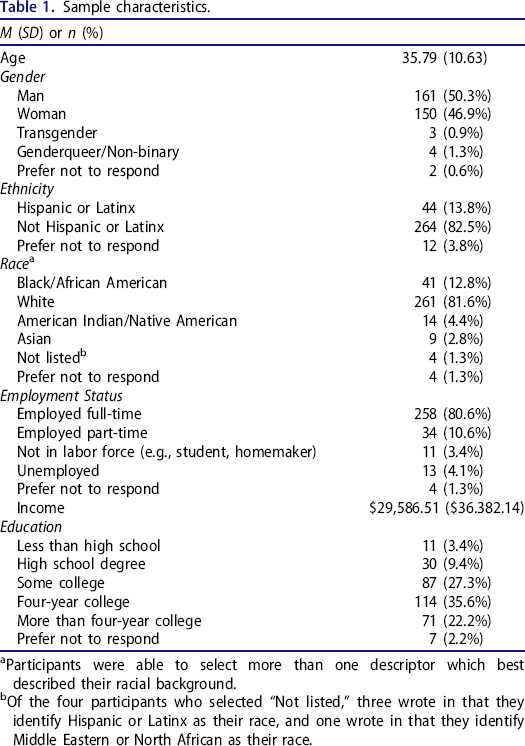
Participants were able to select more than one descriptor which best described their racial background.
Of the four participants who selected “Not listed,” three wrote in that they identify Hispanic or Latinx as their race, and one wrote in that they identify Middle Eastern or North African as their race.
Preliminary analyses
Based on benchmarks of skewness >2 and kurtosis >7 reflecting non-normality, 40 scores for the primary study variables were normally distributed. Approximately half of participants reported a hazardous pattern of alcohol use (n = 175, 54.7%) and more than one-third reported a hazardous pattern of drug use (n = 126, 39.4%) based on cutoff scores of 8 and 3 on the AUDIT30 and DAST-10, 32 respectively. Bivariate correlations and descriptive statistics of primary study variables of interest are presented in Table 2. Each of the substance-use-related stigma subscales, EF deficits subscales, and alcohol and drug use problems were significantly positively associated with one another.
Bivariate correlations and descriptive statistics for primary variables of interest.
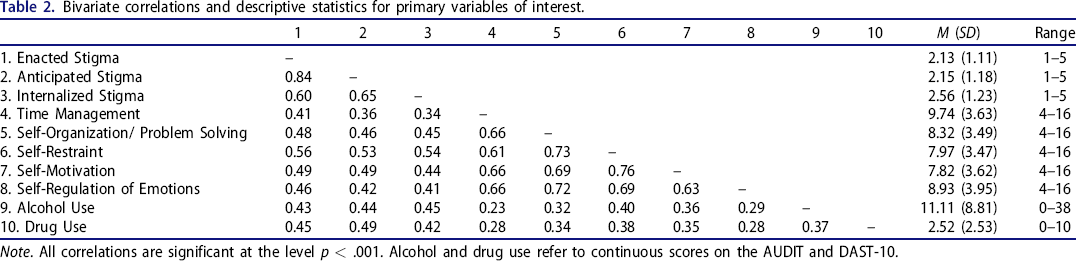
Note. All correlations are significant at the level p < .001. Alcohol and drug use refer to continuous scores on the AUDIT and DAST-10.
Primary analyses
The hypothesized structural model demonstrated good model fit, χ2(32) = 83.11, p < .001, CFI = 0.97, RMSEA = 0.07, 90%CI [0.05, 0.09], SRMR = 0.04; this model is summarized in Figure 2. The association between substance-use-related stigma and EF deficits was significant (β = 0.64, SE = 0.05, p < .001, 95%CI [0.54, 0.72]), as was the association between EF deficits and substance use problems (β = 0.21, SE = 0.10, p = .04, 95%CI [0.01, 0.41]). Furthermore, the indirect effect of substance-use-related stigma on substance use problems through EF deficits was also significant (β = 0.13, SE = 0.07, p = .04, 95%CI [0.01, 0.27]), though the direct effect linking substance-use-related stigma and substance use problems remained significant after controlling for EF deficits (β = 0.70, SE = 0.10, p < .001, 95%CI [0.49, 0.91]).
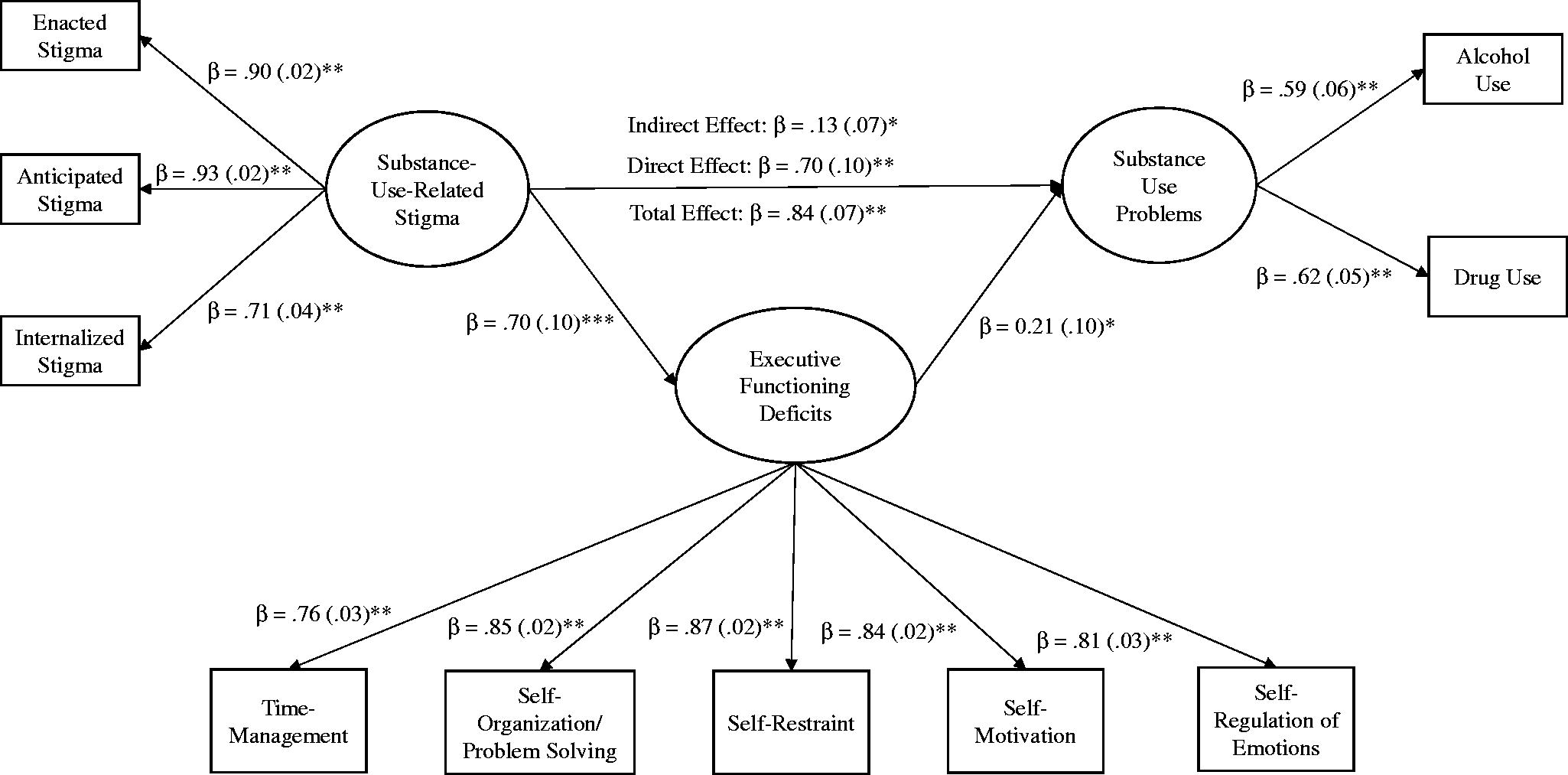
Indirect effect of executive functioning deficits in the association between substance-use-related stigma and substance use problems.
Supplementary analyses
An alternative model was also tested to examine the reverse directionality with substance use problems being related to substance-use-related stigma through EF deficits. This model provided similar fit to the data, χ2(32) = 83.11, p < .001, CFI = 0.97, RMSEA = 0.07, 90%CI [0.05, 0.09], SRMR = 0.04; this model is summarized in Figure 3. In this model, the association between substance use problems and EF deficits was significant (β = 0.66, SE = 0.07, p < .001, 95%CI [0.53, 0.78]), though the association between EF deficits and substance-use-related stigma was not significant (β = 0.16, SE = 0.16, p = .34, 95%CI [–0.25, 0.33]). Further, the indirect effect of substance use problems on substance-use-related stigma through EF deficits was not significant (β = 0.10, SE = 0.12, p = .37, 95%CI [–0.20, 0.21]), while the direct effect of substance use problems on substance-use-related stigma was significant after controlling for EF deficits (β = 0.73, SE = 0.17, p < .001, 95%CI [0.51, 1.04]).
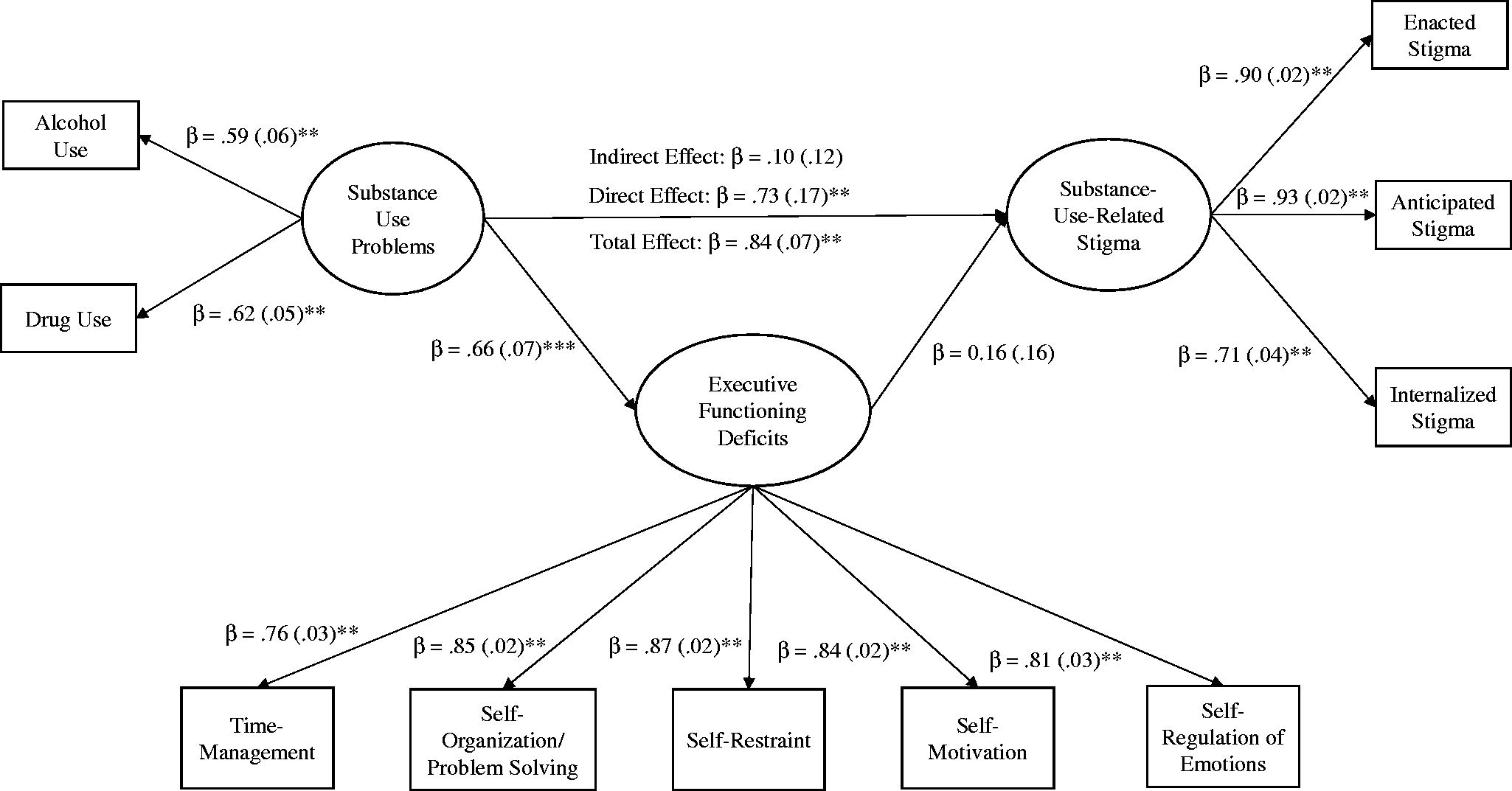
Reverse model depicting the indirect effect of executive functioning deficits in the association between substance use problems and substance-use-related stigma.
Discussion
Recent studies have identified stigma as a potential risk factor for exacerbating substance use problems among individuals who use alcohol and/or drugs, 5 – 7 yet little is known about the psychosocial mechanisms underlying this relationship. The current investigation extends prior research by examining the associations among substance-use-related stigma, EF deficits, and substance use problems in a sample of adults exposed to trauma, a population known to be at exponential risk for developing SUDs. Consistent with our hypotheses, we found that substance-use-related stigma was positively associated with EF deficits, which in turn related to substance use problems. Furthermore, stigma was indirectly associated with substance use problems through EF deficits. Taken together, these results highlight the role of EF deficits as a potential mechanism through which stigma drives substance use problems among this at-risk population.
The present findings have important theoretical and practical implications. Previous studies linking substance-use-related stigma to substance use problems have almost exclusively focused on internalized stigma among people diagnosed with SUDs. 5 – 7 The present research contributes to the existing literature by conceptualizing substance-use-related stigma as a multifaceted construct that encompasses enacted, anticipated, and internalized stigma, and by examining the impact of these distinct facets of stigma among individuals with varying severities of substance use. Our results provide preliminary support for the proposition that different manifestations of substance-use-related stigma, which are known to differentially impact physical, mental, and behavioral health outcomes, 8 may be collectively linked to varying severities of substance use problems, thus exacerbating substance use risk and undermining recovery. More practically, our results highlight the potential value of addressing stigma and EF deficits in substance use prevention and treatment efforts, especially those geared toward populations exposed to trauma. Indeed, acceptance and commitment therapy (ACT), which focuses on facilitating emotional and behavioral regulation via mindfulness and acceptance, has demonstrated initial promise in reducing internalized stigma and substance use problems among patients in a residential substance use treatment program. 41 Future research is needed to assess the impact of ACT on various indicators of EF, as well as its efficacy with more diverse populations who use substances, including those without a SUD and those with a history of trauma. Beyond internalized stigma, researchers could also explore ways to address enacted and anticipated stigma, both by facilitating stigma coping among individuals who use substances and by reducing stigmatizing attitudes among key stakeholders, such as healthcare providers. For example, exercises that have been known to facilitate stigma coping among other marginalized populations (e.g., consciousness-raising, self-affirmation) 42 might be incorporated into standard substance use prevention and treatment interventions, such as motivational interviewing and cognitive behavioral therapy. Further, educational workshops and coursework that address common stereotypes and misperceptions about substance use should be incorporated into clinical training programs and continuing education curricula for medical and mental health professionals, which would in turn enable those individuals to create programs that are more conducive to reducing substance use risk and enhancing recovery.
The present investigation has several limitations. First, the cross-sectional nature of our data precluded predictive, causal conclusions. Specifically, whereas our conceptualization of substance-use-related stigma as a predictor of EF deficits and substance use problems is well-grounded in the empirical literature, 5 , 6 , 20 it is also possible that individuals who reported more substance use problems would experience more stigma and EF deficits as a result of their alcohol and/or drug use. Future research using prospective designs, such as longitudinal or daily diary studies that assess substance-use-related stigma, EF deficits, and substance use problems repeatedly over time, is needed to clarify the relationships among these constructs and elucidate the long-term, causal impact of substance-use-related stigma on substance use behaviors.
Second, given that trauma-exposed individuals might be particularly vulnerable to stigma-related EF deficits due to comorbid psychopathology (e.g., posttraumatic stress disorder, depression), 21 our focus on this population represents a key strength of the present research. Nevertheless, consistent with the inclusion criteria of the larger study on which the current investigation is based (i.e., individuals who have engaged in at least one instance of alcohol/drug use in the past 30 days were eligible), our sample includes participants with varying severities of substance use, and many might experience significantly less stigmatization than individuals who are diagnosed with SUDs. Further, because participants for the current study were recruited on-line via Amazon's MTurk, our sample was relatively homogeneous, with most of the participants being White and well-educated. Lastly, although all participants lived in North America in line with eligibility criteria for the larger study, their specific country of residence was not assessed and thus could not be accounted for in data analyses. Future research should carefully examine the generalizability of our findings to other samples, such as individuals without trauma histories, individuals who are currently receiving substance use treatment, and individuals from diverse racial/ethnic backgrounds. Additionally, given that social norms surrounding substance use, stigma, and treatment might vary significantly across cultures (even among countries within North America), future research should take participants’ country of residence into account (either by including country of residence as a covariate or by stratifying participants based on country of residence) when examining the generalizability of our findings.
In sum, the present research contributes to the existing literature by providing initial support for the role of EF deficits as a mechanism underlying the association between substance-use-related stigma and substance use problems among individuals exposed to trauma who use substances. Further, findings underscore the potential utility of addressing stigma coping and EF deficits in substance use prevention and treatment interventions.
Footnotes
Author Contributions
Author Wang conceptualized the project, guided the selection of study variables and analyses, and contributed to writing the initial draft. Author Schick provided the formal statistical analyses and contributed to writing the initial draft. Author Weiss provided the data used in the present project and contributed to writing the initial draft. All authors reviewed and approved the final manuscript before submission.
Acknowledgement
The authors would like to thank the lead research assistant for this study, Devon Quinn.
Disclosure statement
No potential conflict of interest was reported by the author(s).