
Abstract
Background: National studies often examine associations between sexual identity and substance use at a single point in time and neglect to examine whether these associations change over time. The present study examines U.S. trends in the past-year prevalence of binge drinking, marijuana use, illicit drug use, and polysubstance use across sexual identity subgroups (gay, lesbian, bisexual and heterosexual). Methods: The data come from four independent, cross-sectional samples measured by the National Survey of Family Growth (2006–2010, 2011–2013, 2013–2015, and 2015–2017). Based on the consistency in the sampling procedures used over time, merging the four data sets was possible. The target population is men and women 15–44 years of age. Results: Lesbian women had the sharpest decline in past-year binge drinking over time, followed by heterosexual women. The prevalence of binge drinking for bisexual women did not change significantly over time and was higher in 2015–2017 than for any sexual identity subgroup. In contrast, there were no significant differences in the prevalence of binge drinking among men by sexual identity subgroup. Past-year abstinence from substance use was consistently lower among lesbian women, gay men, and bisexual women relative to other sexual identity subgroups. Polysubstance use was consistently more prevalent among bisexual women (e.g., 32.3% in 2015–2017) as compared to other sexual identity subgroups. Conclusion: This is the first study to examine U.S. national trends in alcohol, marijuana, illicit drug, and polysubstance use across sexual identity subgroups, and demonstrates that sexual identity subgroup differences were robust with relatively few changes in trends over time. The consistently high rates of binge drinking and polysubstance use among bisexual women deserve much closer attention based on the related health consequences.
Introduction
Alcohol, tobacco, and other drug misuse contribute considerably to morbidity and mortality worldwide. 1 – 4 More than 3 million global deaths were attributable to harmful alcohol use in 2016, accounting for over 5% of the global disease burden. 4 Tobacco use remains the leading preventable cause of death; worldwide, tobacco use causes more than 5 million deaths per year, and current trends show that by 2030 tobacco use will cause more than 8 million deaths annually. 5 A large body of research indicates that sexual minorities (e.g., individuals who self-identity as lesbian, gay, or bisexual) are disproportionately impacted by adverse substance-related consequences because they are more likely than heterosexuals to engage in heavy drinking, cigarette smoking, and other substance use. 6 – 12 However, national studies often examine associations between sexual identity and substance use at a single point in time and have not examined whether these associations have changed over time. Although researchers increasingly consider sexual identity an important area of inquiry, no studies have examined U.S. trends in alcohol, tobacco, marijuana, and illicit drug use based on sexual identity. And among sexual minorities, major changes in the U.S. landscape over the past decade—including same-sex marriage laws, marijuana policy, and online direct-to-consumer advertising—have impacted their substance use behaviors and their risk of experiencing substance-related adverse consequences. 13 – 15
To date, polysubstance use trends have received little attention (i.e., the use of two or more substances simultaneously or within a specified time), despite the persistent and severe developmental course associated with polysubstance use. 16 – 18 Several epidemiological studies have documented high rates of polysubstance use in general populations worldwide and among sexual minorities. 16 – 24 In addition, there is evidence that abstinence from alcohol use and cigarette smoking has increased in the U.S. over the past decade while abstinence from marijuana use has decreased during the same period. 25 – 28 However, there have been no studies examining whether these trends in abstinence from substance use differ for U.S. sexual minorities relative to heterosexuals. Therefore, the main objective of the present study is to examine U.S. trends in the prevalence of alcohol, tobacco, marijuana, illicit drug (e.g., cocaine, crystal methamphetamine), and polysubstance use across sexual identity subgroups (gay/lesbian, bisexual, and heterosexual) based on four independent, cross-sectional samples from the National Survey of Family Growth (NSFG; 2006–2017).
Methods
Data description
The data analyzed in this study came from four independent, cross-sectional samples of individuals measured by the NSFG between 2006 and 2017. Our target population was civilian, noninstitutionalized men and women aged 15–44 years who live in U.S. households. Sample sizes and response rates can be found in Table 1. More information about the NSFG's sample design, sample selection, and data collection procedures can be found elsewhere. 29 – 32 This study was exempt from Institutional Review Board approval and informed consent, as deidentified data were used.
NSFG sample sizes and response rates, by sample, NSFG, 2006–2017.a
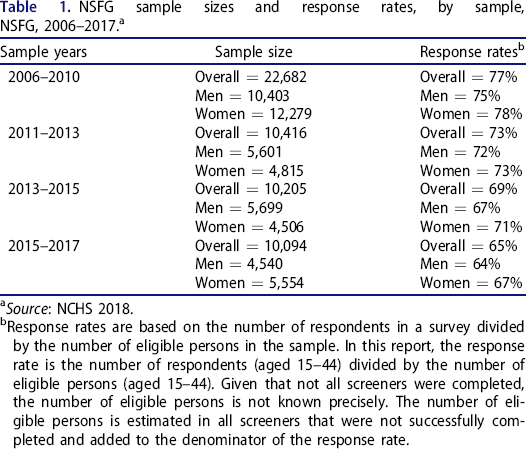
Source: NCHS 2018.
Response rates are based on the number of respondents in a survey divided by the number of eligible persons in the sample. In this report, the response rate is the number of respondents (aged 15–44) divided by the number of eligible persons (aged 15–44). Given that not all screeners were completed, the number of eligible persons is not known precisely. The number of eligible persons is estimated in all screeners that were not successfully completed and added to the denominator of the response rate.
Data merging
Based on the consistency in the complex sampling procedures used for the NSFG during this time period, merging the four data sets was possible. However, between the 2006–2010 and the 2011–2013 samples, there was a fifteen-month hiatus in data collection. 30 Based on this, caution was taken with data merging. For the 2011–2013, 2013–2015, and 2015–2017 cycles, the National Center for Health Statistics (NCHS) suggests that it is possible to append these samples as there was no hiatus in data collection. 30 Correct sampling cluster IDs, non-overlapping codes for sample strata, and final survey weights were used for proper merging across the independent samples. The 2013–2015 NSFG codebook includes a specific note about the stratum and cluster variables, known as the sample design variables: “No transformation is needed to the sample design variables if you are only combining data from 2002 or later because the numbering for the primary sampling units did not overlap for these NSFG survey years.” 29 Thus, stratum and cluster variables were non-overlapping and correct, respectively.
For correct survey weights, manipulation of the available weights was required when merging the data files. The NSFG offers six-year weights for 2011–2017, allowing us to merge the cohorts within that range (i.e., 2011–2013, 2013–2015, and 2015–2017). No weights are offered to append 2006–2010 with 2011–2017, meaning that weight manipulation was required for proper appending. The National Health and Nutrition Examination Survey (NHANES) Analytic Guidelines suggest scaling weights based on the number of years within each sample. 33 Since a single 12-year sample was desired for this study, the 2011–2017 weights were multiplied by 7/12 and the 2006–2010 were multiplied by 5/12. With this manipulation, the scaled survey weights enabled population inferences based on the full 12-year sample. Alternatively, when we analyzed the four samples separately, we used the specific survey weights provided for each of the four public-use data files.
We downloaded data for each sample from the NSFG website (https://www.cdc.gov/nchs/nsfg/nsfg_questionnaires.htm), except for the 2006–2010 audio computer-assisted self-interviewing (ACASI) sensitive data on drug use and sexual identity. These data were received via hard copy from NCHS. After using the data set-up files provided by NCHS, initial data cleaning occurred. For 2006–2010, an extra step was taken by merging the 2006–2010 ACASI data with the NSFG-provided 2006–2010 data. We appended the 2011–2017 samples together with the six-year weights provided by NCHS.
Measures
Sexual identity
Between 2006 and 2017, the NSFG used two different response options to assess sexual identity. In 2006–2007, a four-category version with response options “homosexual, heterosexual, bisexual or something else” was used. In 2008, the “something else” response option was removed, reducing the response options to three categories. In the 2015–2017 sample year, a split-ballot experiment was conducted with two versions (a three-category version and a four-category version) of the sexual identity question. While research suggests that including “something else” as a response option alters associations of sexual identity with substance use behaviors, 34 for the present analysis, similar response options were needed across the samples. Two approaches were assessed: (1) including respondents who received the four-category version of the sexual identity question and removing respondents who answered “something else” from analysis, or (2) only using respondents who received the three-category version of the question. Comparing the approaches across the outcome variables showed no statistically significant differences. Thus, in order to maximize cases that could be included, we implemented the first approach.
Binge drinking, marijuana use, and illicit drug use
These substance use measures were the main outcome variables of interest, and these indicators were coded as either “Yes” or “No.” Binge drinking was defined as consuming ≥5 alcoholic beverages for men and ≥4 alcoholic beverages for women on the same occasion in the past 12 months. Marijuana use was defined as using any marijuana in the past 12 months. Any illicit drug use was defined as using cocaine, crack, or crystal methamphetamine in the past 12 months. Abstinence from substance use was defined as no use of alcohol, marijuana, and illicit drugs in the past 12 months. Polysubstance use was defined as reporting two or more of the following substance use behaviors: binge drinking, marijuana use, cocaine use, crack use, crystal methamphetamine use, or other injection drug use in the past 12 months.
Socio-demographic covariates
The covariates included age (15–24, 25–34, 35–44), race (African-American, White, Other), Hispanic/Latino ethnicity (Yes, No), income ($0-$19,999, $20,000-$34,999, $35,000-$74,999, $75,000+), and sample (years of participation in the NSFG).
Statistical analysis
All statistical analyses were conducted using the survey (svy) commands in Stata (Version 16.1). These commands ensure appropriate design-based analyses of the NSFG data, enabling population inferences that account for the NSFG survey weights and the stratified cluster sampling in the analysis. For our analysis, the main independent variable was sexual identity. Our analyses were stratified by sex to account for well-documented sex differences in alcohol and other drug use. 6 , 35 – 37 To stratify by sex in the analysis, we used the subpop() option in the svy commands that enables appropriate analysis of subpopulations in complex samples. 38 For both the combined sample and each of the four samples, we first estimated bivariate associations between sexual identity and age, race, Hispanic ethnicity, income, sample years, past-year binge drinking, past-year cigarette smoking, past-year marijuana use, and past-year illicit drug use. We estimated the distribution of each variable as a function of sexual identity along with 95% confidence intervals for the percentages estimated. The significance level based on the Rao-Scott test of association was also computed. 39 The combined analyses employed the scaled survey weights described above, and the sample-specific analyses employed the original survey weights provided by NCHS for each sample.
After examining the bivariate associations for each of the four samples, we fitted logistic regression models to the data from the combined sample, with the substance use indicators as our main outcome variables and sexual identity as our main independent variable. Covariates in the models included a categorical factor representing the study years (with four possible levels: 2006–2010, 2011–2013, 2013–2015, and 2015–2017), income, age, race, and Hispanic ethnicity. We also included interactions between sexual identity and the study year factor to test the possibility that the sexual identity disparities varied over time. In order to obtain marginal predicted probabilities of each behavior for the sexual identity subgroups across the years, we used the margins command in Stata after fitting each logistic regression model. We performed pairwise comparisons of the marginal probabilities (across sexual identity subgroups and across study years) based on the fitted models.
To examine and compare trends based on the fitted models, we compared outcomes for groups defined by later study years to outcomes for groups defined by earlier study years. For example, we compared the odds of selected outcomes based on the 2011–2013 study years to the odds based on the 2006–2010 study years, and then 2013–2015 to 2011–2013, and so on. Each logistic regression model fitted contained the same variables and used the same cases, and we simply changed the reference category for the categorical study years factor to compare the reference study years to the previous sample years.
Results
Sexual identity and substance use (2006–2017 combined)
Table 2 shows results from the first analysis, examining overall bivariate associations between sexual identity and the substance use variables, stratified by sex, based on the combined 12-year sample (2006–2017). Bisexual (56.4%) and lesbian (55.6%) women had higher estimated past-year binge drinking rates than heterosexual women (38.0%, p < 0.0001). Bisexual and lesbian women also had higher estimated rates of past-year cigarette smoking (40.5%, 36.5%), marijuana use (43.3%, 36.3%), and illicit drug use (9.5%, 6.9%) when compared to heterosexual women (21.4%, 15.0%, and 2.1% respectively, p < 0.0001).
Estimated distributions of socio-demographic variables and substance use by sexual identity in the U.S., condensed sexual identity question, NSFG, 2006–2017 (sample years combined).
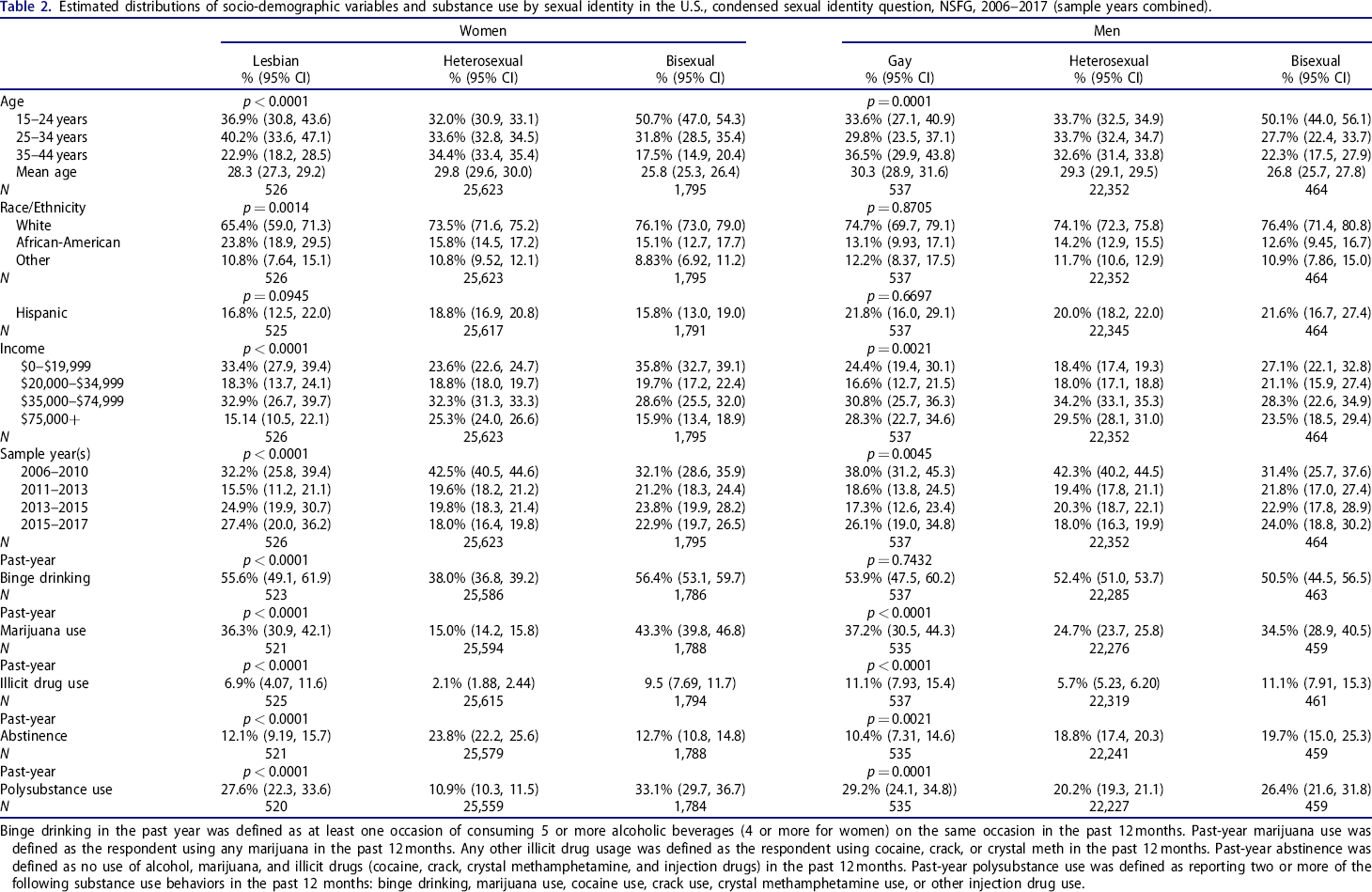
Binge drinking in the past year was defined as at least one occasion of consuming 5 or more alcoholic beverages (4 or more for women) on the same occasion in the past 12 months. Past-year marijuana use was defined as the respondent using any marijuana in the past 12 months. Any other illicit drug usage was defined as the respondent using cocaine, crack, or crystal meth in the past 12 months. Past-year abstinence was defined as no use of alcohol, marijuana, and illicit drugs (cocaine, crack, crystal methamphetamine, and injection drugs) in the past 12 months. Past-year polysubstance use was defined as reporting two or more of the following substance use behaviors in the past 12 months: binge drinking, marijuana use, cocaine use, crack use, crystal methamphetamine use, or other injection drug use.
For men, there were statistically significant differences by sexual identity for marijuana use (37.2% for gay men, 34.5% for bisexual men, and 24.7% for heterosexual men, p < 0.0001) and illicit drug use (11.1% for gay men, 11.1% for bisexual men, and 5.7% for heterosexual men, p < 0.0001). However, there were no statistically significant differences in other substance use behaviors.
In Table 2, past-year abstinence from substance use differed significantly by sexual identity subgroups for both men and women. Among women, past-year abstinence from alcohol, marijuana, and illicit drugs was lower among lesbian women (12.1%) and bisexual women (12.7%) than heterosexual women (23.8%; p < 0.0001). Among men, past-year abstinence was less prevalent among gay men (10.4%) relative to bisexual (19.7%) and heterosexual men (18.8%; p = 0.0021). Similar associations were present in past-year polysubstance use across the sexual identity subgroups among women. Approximately one in three bisexual women (33.1%) reported polysubstance use relative to 27.6% of lesbian women and 10.9% of heterosexual women (p < 0.0001). Similarly, past-year polysubstance use was more prevalent among bisexual men (26.4%) and gay men (29.2%) than heterosexual men (20.2%) (p < 0.0001). The bivariate associations between sexual identity and substance use examined for Table 2 were also examined for each sample (e.g., 2011–2013) separately, and differences in substance use as a function of sexual identity were consistently more robust in women than men (Online Supplemental Material 1).
Sexual identity differences in substance use over time (2006–2010, 2011–2013, 2013–2015, and 2015–2017 separately)
Table 3 presents differences in substance use by sexual identity within each sample (2006–2010, 2011–2013, 2013–2015, 2015–2017). Lesbian and bisexual women had a significantly higher probability of past-year binge drinking than heterosexual women across all samples (p < 0.005), except for lesbian women in 2015–2017 (Figure 1). Generally, lesbian and bisexual women had significantly higher probabilities of past-year marijuana use, illicit drug use, and polysubstance use. Lesbian and bisexual women also had lower probabilities of abstinence (p < 0.01) for all sample years, except for lesbian women in the 2013–2015 sample year. For each outcome, no significant differences between lesbian and bisexual women were found. Sporadic differences existed between gay and heterosexual men in the probability of marijuana and illicit drug use. No significant differences were found between gay men and bisexual men.
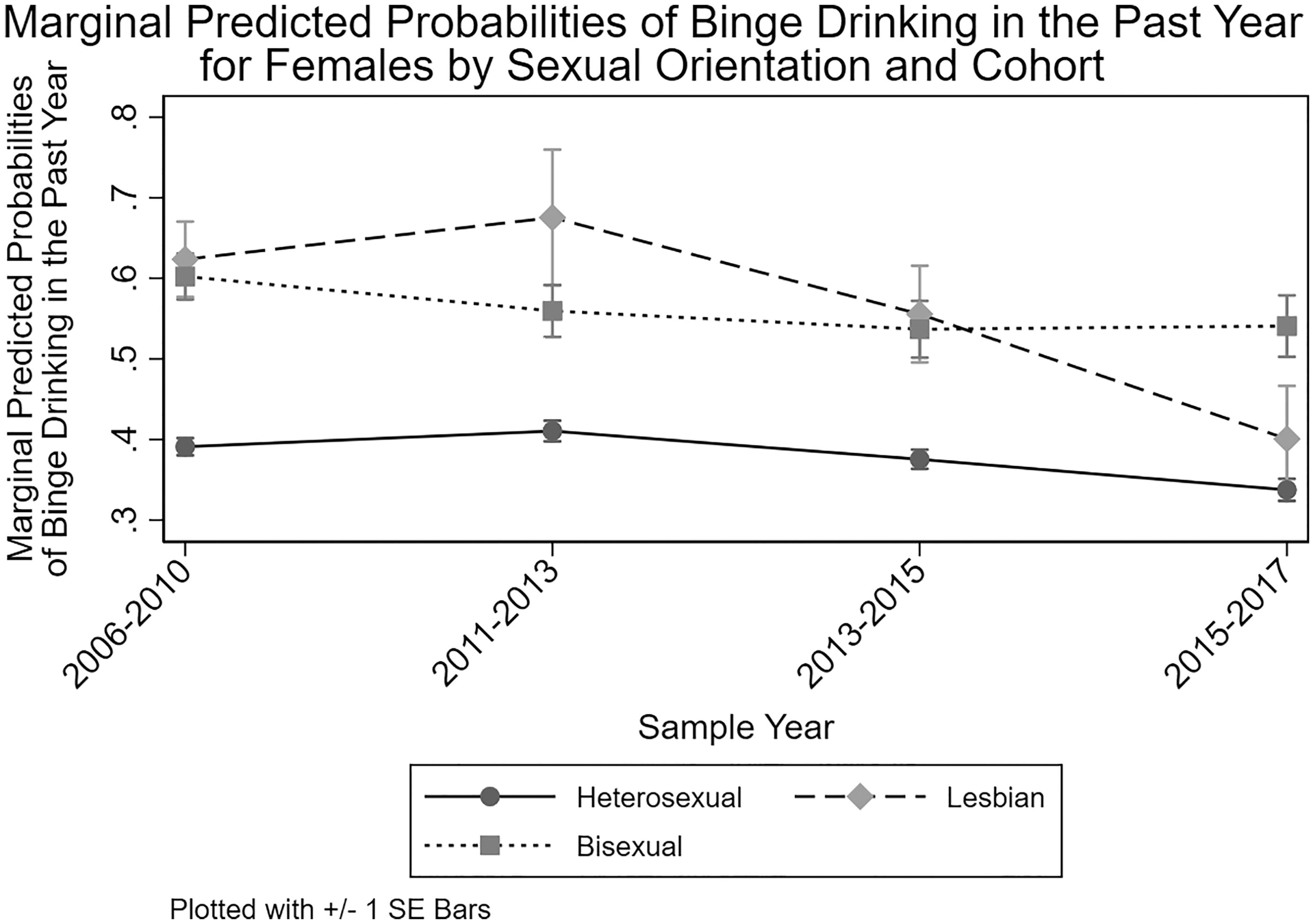
Marginal Predicted Probabilities of Binge Drinking in the Past Year for Females by Sexual Orientation and Cohort.
Marginal predicted probabilities for past-year alcohol use, marijuana use, illicit drug use, polysubstance use, and abstinence by sexual identity and cohort in the United States, NSFG, 2006–2017.
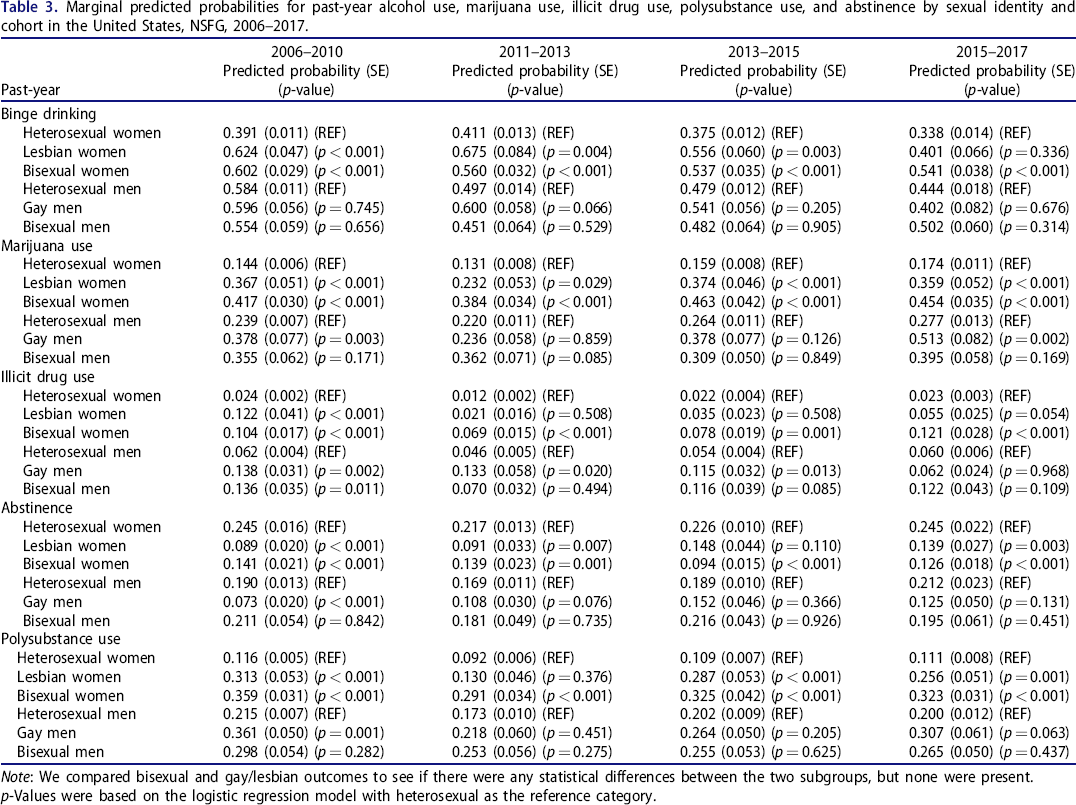
Note: We compared bisexual and gay/lesbian outcomes to see if there were any statistical differences between the two subgroups, but none were present.
p-Values were based on the logistic regression model with heterosexual as the reference category.
Short-term differences in substance use within sexual identity subgroups
Table 4 presents differences in substance use within sexual identity subgroups across the samples, with estimates based on each sample relative to the previous sample (e.g., 2013–2015 compared to 2011–2013). There were few significant differences in substance use across time. In 2011–2013, binge drinking among heterosexual men (p < 0.001) and illicit drug use among heterosexual women (p < 0.001) decreased compared to 2006–2010. In the 2013–2015 sample, heterosexual men increased their marijuana use (p < 0.01) and heterosexual women increased their illicit drug use (p < 0.01) compared with their respective counterparts in 2011–2013. There were no significant differences in abstinence within sexual identity subgroups by sample years. Polysubstance use among heterosexual men and heterosexual women decreased significantly in 2011–2013 (p < 0.01) compared to their counterparts in 2006–2010. No other significant differences were found in sexual identity subgroups across the other sample years.
Marginal predicted probabilities for past-year alcohol use, marijuana use, illicit drug use, polysubstance use, and abstinence by sexual identity and cohort in the United States across cohort years, NSFG, 2006–2010 vs. 2011–2013 vs. 2013–2015 vs. 2015–2017.
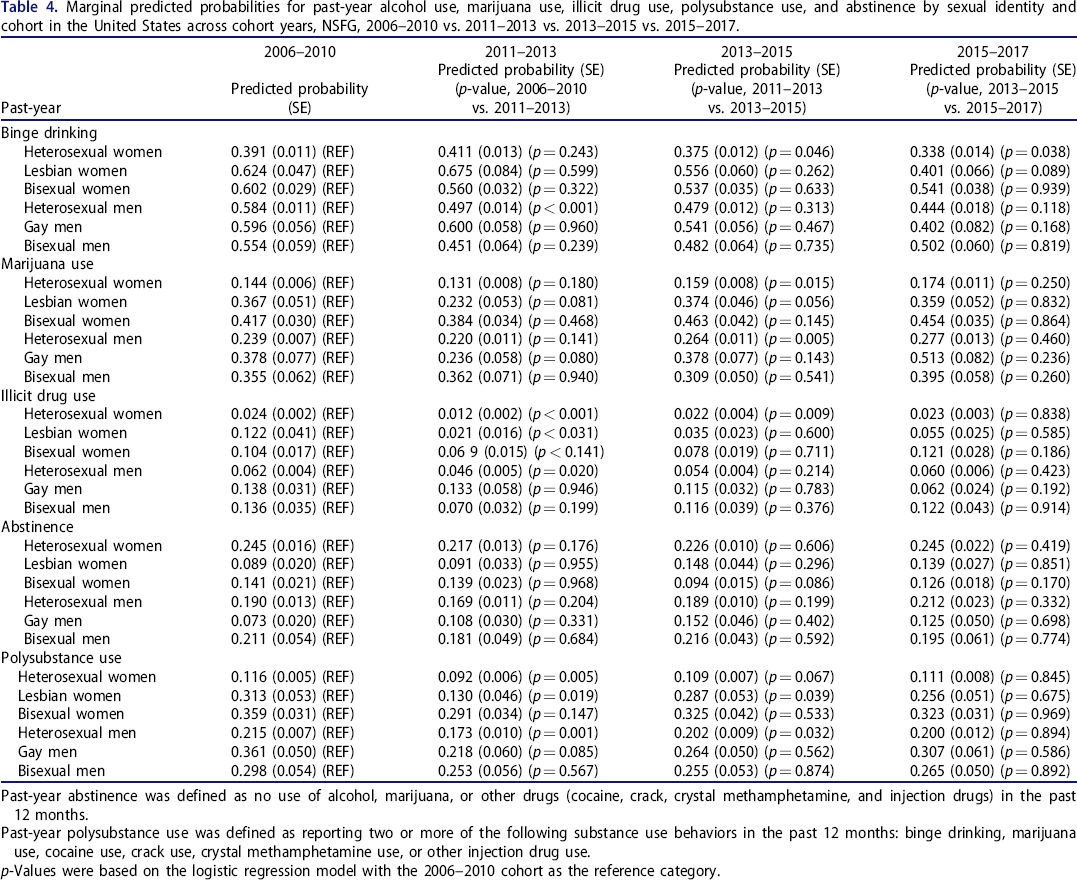
Past-year abstinence was defined as no use of alcohol, marijuana, or other drugs (cocaine, crack, crystal methamphetamine, and injection drugs) in the past 12 months.
Past-year polysubstance use was defined as reporting two or more of the following substance use behaviors in the past 12 months: binge drinking, marijuana use, cocaine use, crack use, crystal methamphetamine use, or other injection drug use.
p-Values were based on the logistic regression model with the 2006–2010 cohort as the reference category.
Long-term differences in substance use within sexual identity subgroups
Table 5 presents long-term differences in substance use outcomes by comparing the 2015–2017 sample to the 2006–2010 sample. In 2015–2017, past-year binge drinking significantly decreased for heterosexual women (p < 0.005) and lesbian women (p < 0.01) when compared with 2006–2010. Past-year binge drinking did not significantly decrease for bisexual women in 2015–2017 compared to 2006–2010. In 2015–2017, pack-a-day cigarette smoking (p < 0.001) significantly decreased for bisexual women compared to bisexual women in 2006–2010, but the same decreases were not present among lesbian women (Online Supplemental Material 2). No significant differences were found among men for any sexual identity subgroup by sample years. Additionally, no long-term significant differences were found in abstinence and polysubstance use among sexual identity subgroups when comparing the 2015–2017 and 2006–2010 sample years.
Long-term marginal predicted probability differences for past-year binge drinking, marijuana use, illicit drug use, polysubstance use, and abstinence by sexual identity and cohort in the United States, NSFG, 2006–2010 vs. 2015–2017.
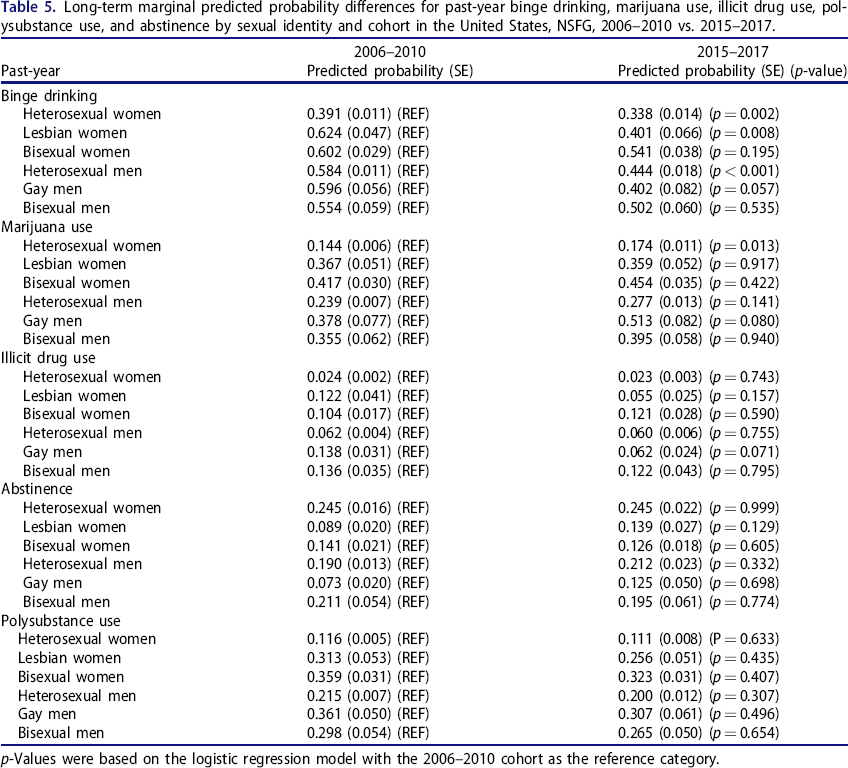
p-Values were based on the logistic regression model with the 2006–2010 cohort as the reference category.
Discussion
The current investigation is the first known U.S. study to examine trends in the prevalence of alcohol, marijuana, illicit drug, and polysubstance use across sexual identity subgroups. We found notable differences in substance use behaviors as a function of sexual identity that often persisted for over a decade. In some cases, sexual minorities did not experience the same significant declines as heterosexual subgroups over time for behaviors that may place individuals at risk for harm, such as binge drinking among bisexual women, which has grave health consequences. Indeed, the prevalence of past-year binge drinking among bisexual women in 2015–2017 was the highest for any sexual identity subgroup, whether male or female. Additionally, we assessed polysubstance use and found that not only are sexual minorities more likely to use individual substances (alcohol, marijuana, illicit drugs), but they are also more likely to use multiple substances. Most notably, the trend analysis revealed that bisexual women consistently reported the highest prevalence of polysubstance use, with approximately one-third of bisexual women reporting polysubstance use across the last decade and most recently in 2015–2017 (33%). These new findings regarding national trends in polysubstance use as a function of sexual identity are especially important as polysubstance use is associated with a persistent and severe developmental course. 16 – 18
The present study revealed sex differences that generally included more robust differences for women than men. For women, there were differences by sexual identity for all substance use outcomes. In contrast, for men, differences were present for marijuana and illicit drug use but did not exist for other substances. We found evidence for different trends in binge drinking over time among women as a function of sexual identity. Lesbian women had the sharpest decline in past-year binge drinking over time, followed by heterosexual women; the prevalence of binge drinking for bisexual women remained steady over time. In contrast, there were no significant differences in the prevalence of binge drinking among men by sexual identity subgroup. There was also evidence that the declines in binge drinking were larger among men over time than women, which is consistent with gender convergence in alcohol use observed nationally. 40 , 41 It is worth noting that there were general declines in binge drinking across all groups, which is consistent with research showing binge drinking decreases in the U.S. 26 , 27
There are several individual and environmental drivers for the differences in substance use among U.S. sexual minorities. For instance, studies have found that the alcohol and tobacco industries target sexual minorities. 42 – 44 Consequently, alcohol prevention and tobacco control among sexual minority populations remain an important public health priority. 45 Additionally, several states have legalized marijuana in the past decade for medical and/or recreational use, meaning that respondents in the present study may be reporting medical use of marijuana. Some studies using nationally representative data have found that sexual minority individuals are more likely to report marijuana use than heterosexual respondents, aligning with the findings of the present study. 46 , 47 One study examined the prevalence of nonmedical and medical marijuana use among sexual minorities in states with medical marijuana laws and found that sexual minorities in states with medical marijuana laws—particularly bisexual women—reported higher medical and nonmedical marijuana use than sexual minorites in states without these laws. 47 One explanation for the higher prevalence of substance use among sexual minorities compared to heterosexuals can be explained by Meyer's Minority Stress Model. 48 – 50 The model posits that sexual minorities experience prejudice, stigma, and discrimination produced by institutional and interpersonal homophobia and heterosexism, and this excess stress creates a hostile social environment that may lead them to engage in substance use as a coping process. 48 , 50 The Minority Stress Model has been extended and supported across a wide range of substance use and mental health outcomes by numerous empirical studies. 7 , 8 , 48 – 53 Thus, the social conditions that produce minority stress can result in adverse health outcomes in sexual minorities, which deserve public health attention. 49
The NSFG has a number of strengths for the present study, including large nationally representative samples and consistent measures of substance use for more than a decade to allow for an examination of U.S. trends (2006–2017). The NSFG also has the limitations of national cross-sectional survey research, including self-reporting bias and an inability to examine sexual orientation as a more fluid construct. The present study focuses on cross-sectional prevalence estimates of sexual identity and substance use that can portray an incomplete picture of sexual identity and substance use severity, as opposed to a needed account of sexual identity fluidity with relevant measures (e.g., substance use disorder symptoms). 54 , 55 In addition, the sexual identity measure was extracted from two different questions (3-category vs. 4-category). As noted in the Methods section, we compared the two question types across the outcome variables and found no statistically significant differences. While the present study focused on trends in substance use as a function of sexual identity, prior work has shown differences across sexual orientation dimensions (i.e., attraction, behavior, and identity) in substance use. 37 , 56 , 57 Finally, this study combines the use of several illicit drugs that have lower prevalence. While looking at individual illicit drugs is ideal, small cell sizes within some of the sexual identity subgroups limited possible analyses.
In sum, these findings reinforce the importance of understanding multiple substance use trends among sexual minorities rather than relying solely on cross-sectional estimates, as emerging substance use trends are often missed in cross-sectional studies examining individual drug classes. Importantly, studies focusing on substance use trends can assess whether known health disparities are becoming worse or improving over time. Binge drinking and polysubstance use among bisexual women deserve closer attention based on the health consequences associated with these substance use behaviors. Disparities in these health behaviors persist among sexual minorities, and thus, these vulnerable populations deserve continued public health attention and resources.
Footnotes
Authors’ contributions
Drs. McCabe and West conceptualized and designed the study. Drs. McCabe and West drafted the initial manuscript. Drs. Kcomt and Evans-Polce reviewed and revised the manuscript. Mr. Engstrom and Dr. West conducted all statistical analyses. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Acknowledgments
The authors would like to thank Ms. Kathryn Lundquist, Mr. Mahmoud Abdulkarim, and Ms. Kate Leary for their assistance with preparing this manuscript for submission.