
Abstract
Substance use disorder (SUD) organizations are often siloed, with little integration across specialty addictions treatment, primary care and hospitals, harm reduction, policy, and advocacy. COVID-19 introduced a pressing need for collaboration and leadership, given a fast-changing, high-stakes environment; widespread anxiety; and lack of guidance. This research letter describes our approach to convening and supporting leaders across the US state of Oregon's SUD continuum during the pandemic. We rapidly developed and implemented a SUD COVID Response ECHO, adapting ECHO – a telementoring model – to convene leaders across 32 statewide agencies. Our experience allowed participants to lead their agencies to respond to real-time COVID-related needs, address existing barriers within SUD systems, and build relationships and community across statewide SUD leaders. This kind of collaboration – which helped bridge gaps among the diverse agencies, disciplines, and regions addressing SUDs in the state – was long overdue, and sows seeds for long-term advances in care for people with SUD.
Keywords
Research letter
Substance use disorder (SUD) systems are often siloed, with little integration or communication across specialty addictions treatment, healthcare, harm reduction, policy, and advocacy organizations. 1 COVID-19 emerged in the midst of a relentless overdose crisis, 2 and created pressing leadership need given a global health emergency, a rapidly changing environment, widespread anxiety, and lack of governmental guidance.
Project ECHO (Extension for Community Healthcare Outcomes) is a distance tele-mentoring medical education model that connects specialists with generalist providers across geographically diverse communities.
3
ECHO is highly interactive, and uses case-based learning and brief expert presentations. In April 2020, we quickly repurposed existing ECHO infrastructure
4
to convene leaders in substance use treatment, advocacy and policy making across the US state of Oregon to participate in an SUD COVID Response ECHO. We aimed to:
Share emerging resources and best practices to deliver SUD care during the COVID-19 pandemic (e.g. low-barrier telemedicine; virtual peer support) Share clinical and regulatory information about COVID-19 Support partnerships across regional agencies Provide a learning community and idea incubator
Unlike traditional ECHO programs, which are generally structured around core faculty experts who support and guide participant-learners, we intentionally amplified the ECHO philosophy of “all teach, all learn.” The rapidly changing environment that emerged in the wake of COVID-19 meant that all parties were adapting as quickly as possible, and in their own ways. Thus, instead of designating specific faculty experts we determined that all – and no – participants were experts as we confronted this unsettling new landscape. This letter describes our experiences and lessons learned, highlighting implications for future collaborative efforts across regional and state SUD organizations.
ECHO timeline and recruitment was as follows: On March 23, Oregon's Governor issued a statewide stay-at-home order. 5 On March 24th, we emailed 28 state-wide SUD agency leaders and asked those leaders to invite others whom they believed would be both interested and have population-level needs, insights and contributions. On April 1 we launched the ECHO with 48 participants across 32 organizations. Leaders heralded from SUD and behavioral health treatment agencies (12); primary care (11) and hospital (1) addiction teams; peer agencies (2); harm reduction organizations (2); advocacy and social service organizations (2); Medicaid payers (1); and state agencies (1). Participant disciplines included physicians and advance-practice providers (21), social workers and counselors (8), public health (3), peer support specialists (2), medical students (4), and others (10). On average, 34 participants attended each session.
The ECHO included twelve weekly hour-long virtual meetings, each including a 5–7 minute didactic by one of the participants followed by a “practice situation,” presented by a different participant. We developed an initial set of didactics based on our own knowledge of community challenges and innovations and expanded that list based on participant feedback and expertise. For example, one didactic outlined how a local treatment center adapted alcohol-withdrawal management protocols to an ambulatory settings after reducing its inpatient bed-capacity to enable physical distancing. The Table 1 describes each of the didactics and summarizes policy/practice implications.
Summary of SUD COVID response ECHO didactics and practice situations.
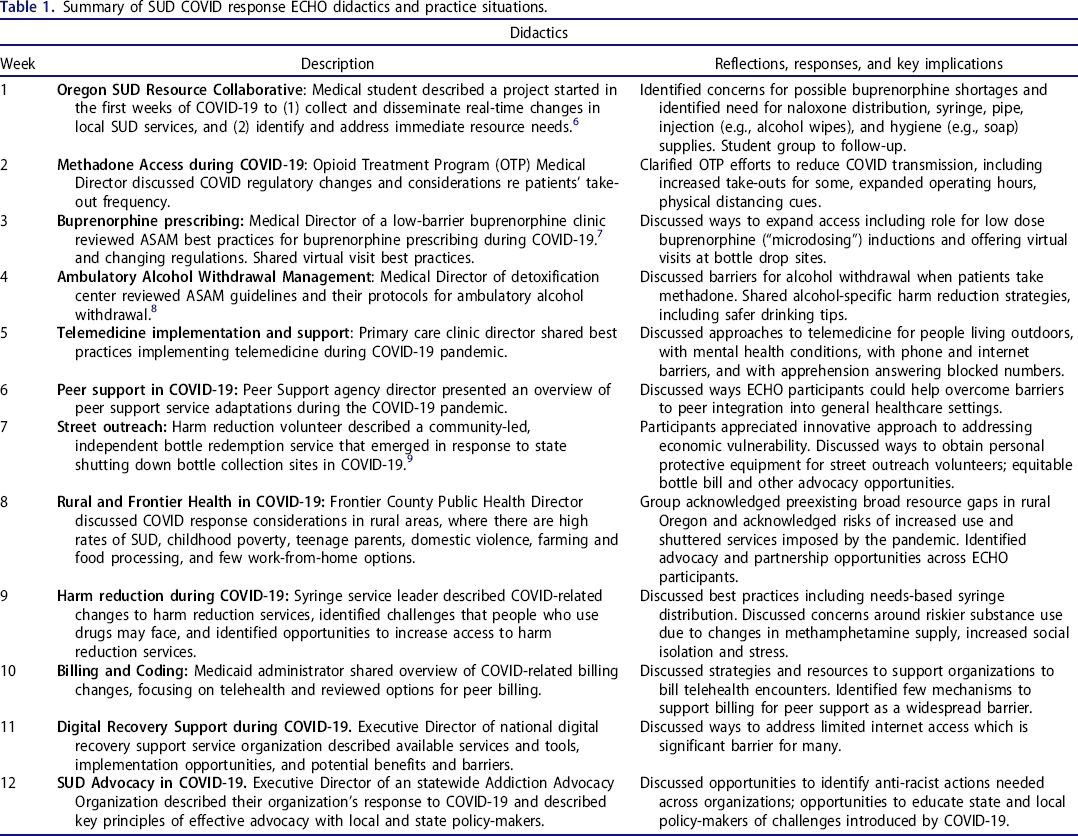
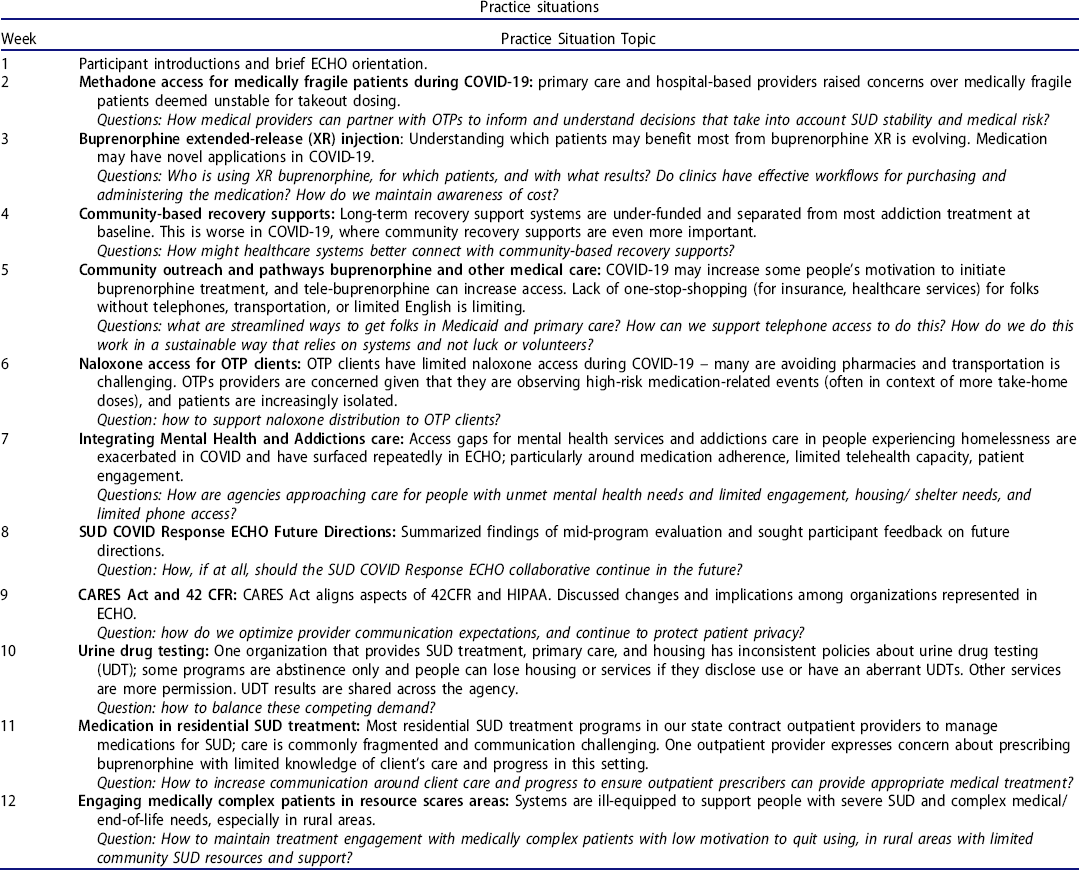
Practice situations included leaders’ challenges addressing addiction from a systems or population level, and could include administrative, resource, process, or other systems-level challenge. We used an SBAR (Situation, Background, Assessment, Request) format and followed presentation with collaborative problem solving among diverse participants. For example, in the first session a physician shared concerns about buprenorphine supply shortages due to longer prescriptions written to minimize in-person clinic and pharmacy time. In response, a participant from the Oregon Health Authority elevated the concern to the state pharmacy board, and a group of medical students systematically contacted pharmacies to assess medication stocks. Over the ensuing weeks, the group shared updates about medication access and efforts underway to prevent shortages. The Table 1 describes the practice situations participants brought to the ECHO, and some practical solutions that emerged.
We conducted a program evaluation in response to early positive feedback about a future-role for the group. We distributed a mid-program open-ended survey exploring participant experiences with COVID-19, with the ECHO, and the group's future. Twenty-one participants completed the survey. We also added an extra session for feedback and future planning, which 26 participants attended. Many participants described an important comradery and support that helped leaders “keep [their] energy going during these strange times.” Many also felt that this collaboration – which included diverse agencies, disciplines, and regions, and focused on concrete and pressing challenges – was long-overdue in a state already struggling to meet needs of people with SUD. Participants noted that the pandemic provided a reason to move past silos and ECHO provided a structure that emphasized collaborative problem solving around discrete issues. Finally, many felt that the presence of strong peer and harm reduction leaders helped center practice and policy decisions on needs of the most vulnerable patients.
We submitted a Request for Determination and the Oregon Health & Science University institutional review board determined this study was not human subjects research.
Participants’ conviction of the value of ECHO beyond the acute COVID-19 crisis pushed us to launch a year-long SUD Leadership ECHO in August 2020. This ECHO builds on strengths of the SUD COVID Response ECHO and expanded recruitment to further engage rural, culturally-specific, and abstinence-based SUD programs; housing, law enforcement, and corrections; government officials; and payers.
Lessons learned include that an SUD COVID Response ECHO provided time and space for shared problem solving and leadership support, resulting in immediate solutions to emergent pandemic-related challenges, and sowing seeds for long-term advances in systems for people with SUDs in our state. The ease of recruitment, robust participation, and positive participant experience highlighted that this kind of collaboration – which helped bridge gaps among the diverse agencies, disciplines, and regions addressing SUDs in the state – was long overdue. ECHO provided a forum to gather around a unifying, common challenge – addressing SUD population health and organizational needs in the pandemic, and is informing how we continue to collaborate and lead amidst an unrelenting substance use epidemic. We hope that our experience is valuable to others working to build more integrated and responsive regional SUD systems.
Footnotes
Acknowledgements
Authors would like to acknowledge all of Oregon's SUD leaders who participated in ECHO for their comradery, collaboration, and hard work during the first months of the COVID pandemic. They would like to acknowledge Drs. Raymundo Garcia-Dwyer, Jennifer Hartley, and Cydney Heims for taking weekly notes and the Oregon ECHO Network for their support.