
Abstract
Background: Research has shown that medications, especially opioid agonist treatments, are an effective way to treat opioid use disorder (OUD); however, negative attitudes held by health professionals contribute to their underutilization. Methods: A 23-year review of studies that examined health professionals’ attitudes toward medications for OUD (MOUD) was conducted to describe the current state of knowledge and to inform future research and interventions. Results: Studies examined attitudes toward the use of methadone, buprenorphine, and naltrexone among various types of health professionals: prescribers, non-prescribing clinicians, pharmacists, and administrators. The characteristics and findings of the included studies were reviewed and synthesized. Findings indicate that attitudes toward MOUD affect access and utilization by influencing prescribing practices, referrals, and adoption within programs. Exposure, knowledge, and treatment orientation were found to be important factors related to attitudes toward MOUD across multiple studies of various types of health professionals. Conclusions: To increase access and utilization, continued efforts are needed to increase positive attitudes toward MOUD among various types of health professionals. Findings indicate that interventions should seek to increase knowledge about MOUD and foster interprofessional communication related to MOUD, especially between prescribers and behavioral health providers.
Introduction
In the last 20 years, both therapeutic and illicit opioid use have escalated at alarming rates in the United States. 1 , 2 Americans consume more opioids than any other country, and as a result, we continue to face a crisis of opioid misuse, dependence, and overdoses. 3 The opioid crisis levies substantial costs in the United States as it inflicts losses on families and communities, requiring massive prevention and treatment efforts. 4 , 5
Treatment efficacy
While many efforts are needed to address the opioid epidemic including policy changes and prevention programs, the delivery of effective treatments for opioid use disorder (OUD) is one of the most important. Millions of Americans suffer from OUD, and outcomes are often grim without access to effective treatments. 6 Thankfully, there are established treatment protocols for OUD which drastically reduce mortality among those addicted to opioids. 7
Pharmacological treatments such as opioid agonist treatments are the most effective treatments available for OUD. Opioid agonist medications such as methadone and buprenorphine enhance relapse prevention and enable individuals with OUD to regain control of their lives. There is substantial evidence that agonist-based treatments are effective in reducing mortality 7 and preventing relapse when properly utilized. 8 Not only are medications for opioid use disorder (MOUD) the most clinically effective treatment available for OUD, but they are also the most cost-effective. Baser et al. 9 found that patients with OUD who received agonist-based treatments had lower hospital utilization and lower total costs than patients who did not.
MOUD are used for both long-term treatment and short-term treatment such as pharmacologically assisted withdrawal. 10 When agonist medications are used for long-term treatment, complete detoxification is not required as patients simply transition from illicit use into opioid agonist therapy without having to suffer withdrawal. 11 When MOUD are used for pharmacologically assisted withdrawal, patients achieve complete detoxification by tapering gradually with the assistance of an opioid agonist or other supportive medication to mitigate withdrawal symptoms. 12 While both of these methods are still widely used, evidence has shown that long-term treatment with methadone or buprenorphine is more effective than tapering and detoxification (i.e., pharmacologically assisted withdrawal). 12 , 13
Methadone, a full opioid agonist, has been available for decades and is relatively inexpensive. 14 However, methadone for OUD is highly regulated and is generally dispensed under direct supervision, requiring frequent visits to a federally approved opioid treatment program. 14 Buprenorphine, a partial opioid agonist, was first approved for the treatment of OUD by the U.S. Food and Drug Administration in 2002. 15 Buprenorphine can be prescribed by any Drug Addiction Treatment Act (DATA) waived physician in an office-based setting, requiring infrequent visits and allowing patients to take the medication in unsupervised settings. 16
Naltrexone, an opioid antagonist, is another medication used for the treatment of OUD which works differently than agonists like buprenorphine and methadone. 17 Instead of activating opioid receptors to reduce cravings, naltrexone blocks opioid receptors, and it is typically administered after complete detoxification. 8 , 17 Naltrexone has a low potential for misuse or diversion compared to opioid agonists, making it an attractive alternative to community-based providers. 18 However, naltrexone does not address withdrawal symptoms, and protocols using naltrexone have shown poor patient compliance and lower induction success rates compared to opioid agonist treatment protocols. 8 , 19
Psychosocial interventions are often strongly encouraged or required in conjunction with MOUD in the U.S, 20 but there is little evidence to suggest that they are effective on their own or additive to agonist-based treatments. 21 – 24 While some MOUD patients find counseling helpful during treatment, and targeted psychosocial interventions may be beneficial supplements for these patients, evidence and practicality support tailoring treatment to the specific needs of each patient rather than a mandate requiring counseling for all. 25 , 26
Treatment access and utilization
Low treatment utilization is a major barrier to combatting the opioid epidemic. In most parts of the country, opioid misuse and addiction rates outpace treatment capacity. 27 Even if the current system for providing MOUD in the United States were at full capacity, it is estimated that nearly one million Americans with OUD would still lack access to these life-saving treatments. 27 Opioid addiction has disproportionately affected those with low-income and living in rural areas, where access to MOUD is often minimal or non-existent. 28
Strategies to combat the opioid epidemic in the United States have targeted low treatment utilization by improving access to MOUD. 29 – 31 Increasing access to agonist-based treatments has been associated with large reductions in opioid-related overdose deaths. 32 , 33 Regulations that allow primary care and other office-based physicians with DATA waivers to prescribe buprenorphine have helped to increase access to MOUD in underserved areas; however, despite improvements, access to and utilization of buprenorphine are still lacking, particularly in the South and in rural areas. 34
Attitudes toward medications for opioid use disorder
While many individuals with OUD lack access to appropriate treatment in the United States, lack of access, alone, does not explain the poor utilization of MOUD observed. There is often underutilization of MOUD even where they are available. 35 Beyond problems with accessing treatment, negative attitudes, and stigma associated with MOUD have contributed to their underutilization in the United States. 8 , 36 , 37 Unfortunately, there is evidence that many health professionals involved with the treatment of OUD harbor negative attitudes toward MOUD, especially opioid agonists. 36 , 38 , 39 Despite the strong evidence supporting the efficacy of MOUD, many health professionals still view them as illegitimate. 40 , 41 Negative attitudes and beliefs toward MOUD held by health professionals can be attributed to a lack of knowledge, perceptions, and concerns. 42 Inadequate training and lack of information about MOUD among prescribing 43 and non-prescribing health professionals such as social workers and counselors 42 are barriers to their successful implementation.
Addressing the stigma associated with participating in treatment with MOUD requires education efforts for both the public and for all health professionals who interact with individuals addicted to opioids, including those who do not prescribe such as counselors and social workers. 44 To develop clinician-targeted interventions that promote evidence-based practices for the treatment of OUD and help address the underutilization of MOUD, a thorough understanding of the current literature regarding health professionals’ attitudes and beliefs toward pharmacological treatments for OUD is necessary.
Research questions
What is the current state of research literature regarding attitudes toward MOUD held by health professionals? What is known about the factors that underlie these attitudes? What is known about whether and how these attitudes affect the implementation and utilization of MOUD? What is known about interventions and strategies to change or modify health professionals’ attitudes related to MOUD?
Methods
Eligibility criteria
A systematic review of studies examining health professionals’ attitudes toward MOUD was conducted for this study. The inclusion criteria for this study were as follows:
studies published in the English language; peer-reviewed articles or dissertations included in at least one of the following databases: Web of Science Core Collection: Science Citation Index Expanded and Social Sciences Citation Index, PubMed, PsycINFO, Social Work Abstracts, Cochrane Library, or ProQuest Dissertations & Theses Global; studies published between January 1, 1997, and June 17, 2021. original studies which sampled U.S. health professionals or conducted secondary analyses with samples of U.S. health professionals; studies which described data or examined outcomes related to implicit or explicit attitudes and/or beliefs toward MOUD held by health professionals; studies that included quantitative data analysis.
Search, distillation, and coding
Using the stated inclusion and exclusion criteria, search and distillation were conducted in four phases: (i) search, (ii) screening titles and abstracts, (iii) retrieval and full review, and (iv) citations review. Phase I utilized Boolean terms to identify articles in any of the included databases. The following Boolean terms were used to search titles, abstracts, and topics: (attitude* OR belief* OR opinion* OR perception* OR perceive* OR position* OR stigma*) AND (“medication-assisted treatment” OR agonist OR antagonist OR naltrexone OR methadone OR buprenorphine) AND (opioid* OR opiate* OR heroin) AND (professional* OR nurse* OR physician* OR counselor* OR social worker* OR psychologist* OR psychiatrist* OR therapist*). Searches were limited to those results written in English and published within the time frame of January 1, 1997, to June 17, 2021. Phase I (search) returned 819 studies. After Phase II (screening), 69 studies remained. Phase III (full retrieval and review) yielded 54 studies. Phase IV (citations review) yielded 16 additional studies resulting in a total of 70 included studies. See Figure 1 for details regarding the search and distillation process including how inclusion criteria were applied during each phase. The author read and coded the 70 included studies into an Excel spreadsheet for the following characteristics: authors, publication year, journal, times cited, purpose, setting, sampling information, types of health professionals, types of pharmacological treatments, outcome measures, factors, analytic methods, findings, conclusions, and limitations.
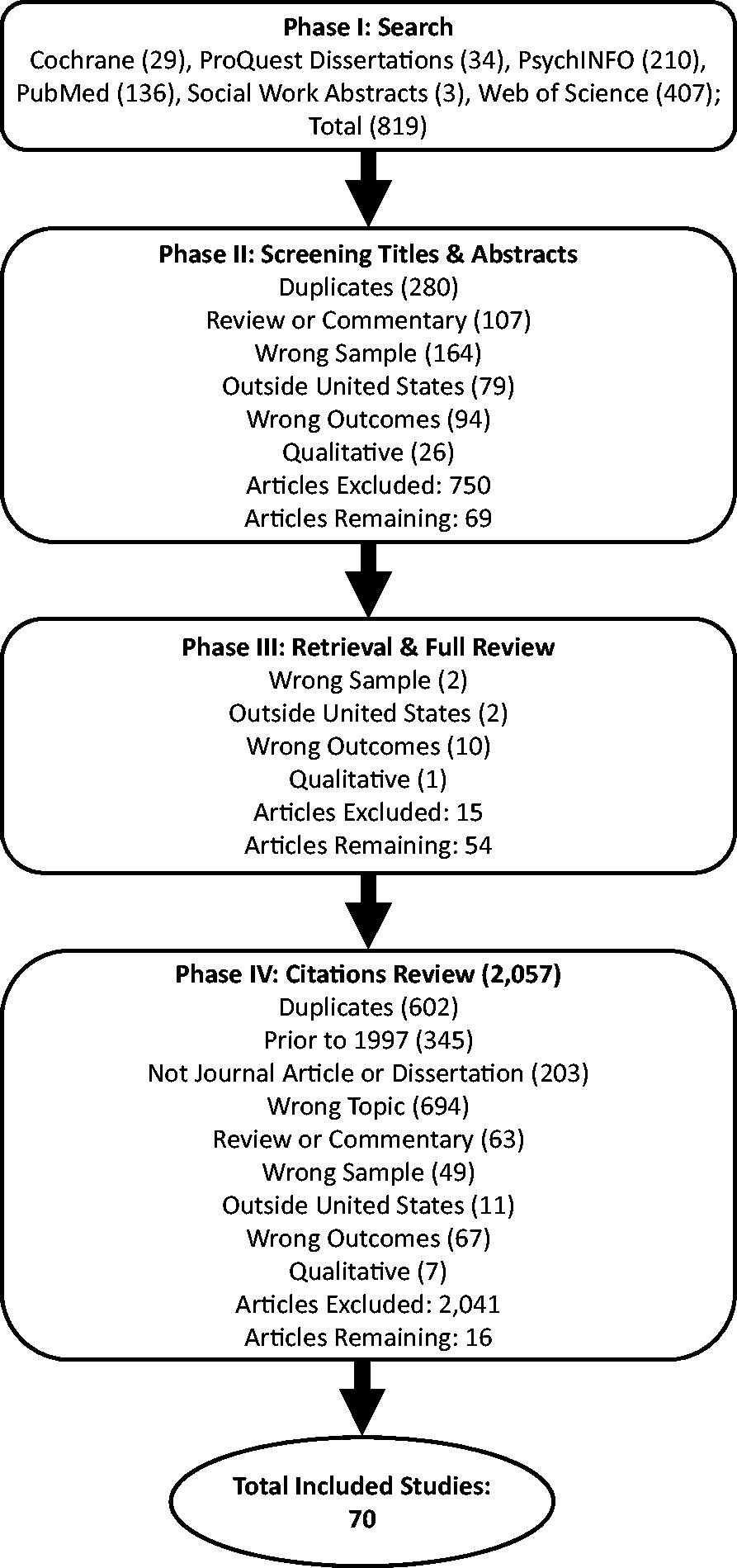
Search and distillation.
Results
Characteristics of included studies
Medications and timeframe
Included studies were published between 1997 and 2021 (see Table 1). Studies that examined attitudes toward methadone (39 of 70; 55.7%) tended to be published earlier in the time frame. The opposite was true for studies that examined attitudes toward buprenorphine (54 of 70; 77.1%); the first such study was published in 2004 soon after FDA approval. Fourteen included studies (20.0%) examined attitudes toward naltrexone and 27 (38.6%) studied attitudes toward more than one type of medication; these studies appeared to be evenly distributed across the time frame.
Included Studies in Chronological Order.
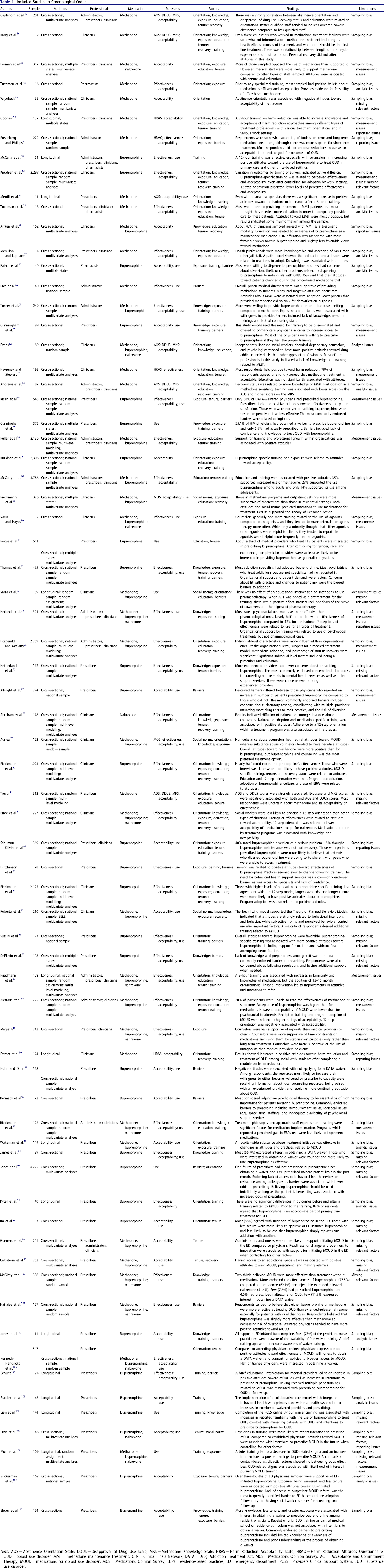
Note. AOS = Abstinence Orientation Scale; DDUS = Disapproval of Drug Use Scale; MKS = Methadone Knowledge Scale; HRAS = Harm Reduction Acceptability Scale; HRAQ = Harm Reduction Attitudes Questionnaire; OUD = opioid use disorder; MMT = methadone maintenance treatment; CTN = Clinical Trials Network; DATA = Drug Addiction Treatment Act; MOS = Medications Opinion Survey; ACT = Acceptance and Commitment Therapy; MOUD = medications for opioid use disorder; MOS = Medications Opinion Survey; EBPs = evidence-based practices; ED = emergency department; PCSS = Providers Clinical Support System; SUD = substance use disorder.
Samples
A majority of included studies sampled professionals in multiple states (37 out of 70; 52.9%), and less than half used national samples of health professionals (30 of 70; 42.9%). However, only 18 included studies (25.7%) used some form of random sampling. Fewer still used random sampling from national sampling frames (14 of 70; 20.0%). The average sample size of included studies was 485 (SD = 836.74; Skewness = 2.88), ranging from 11 45 to 4,225. 46 Among the included studies many types of health professionals were represented including prescribing professionals and other medical staff; non-prescribing clinicians (NPCs, e.g., counselors, social workers, and psychologists); pharmacists and pharmacy assistants; and those who worked primarily as administrators. Medical professionals were the most represented (46 of 70; 65.7%) followed by NPCs (34 of 70; 48.6%), administrators (14 of 70; 20.0%), and pharmacists (4 of 70; 5.7%). About a quarter of included studies (16 of 70; 22.9%) sampled multiple types of health professionals.
Designs
The designs of included studies were primarily cross-sectional, however, 13 studies implemented longitudinal designs. Only 3 studies utilized random assignment to different conditions. 73 , 88 , 108 Six of the included studies utilized multi-level modeling to assess how organizational characteristics affect attitudes and beliefs toward MOUD among health professionals. Half of the included studies (35 of 70) used some form of multivariate analyses to allow for better statistical control when considering factors related to attitudes and beliefs toward MOUD.
Measures of attitudes and beliefs
Outcome measures related to attitudes and beliefs about MOUD were categorized as follows: attitudes toward effectiveness; attitudes toward acceptability; and measures of use, willingness to use, or intentions to use MOUD. Attitudes toward the acceptability of MOUD was the most common category of outcome measure, representing 78.6% of included studies (55 of 70), followed by measures of use, willingness to use, or intentions to use MOUD (42 of 70; 60.0%), and attitudes about their effectiveness (34 of 70; 48.6%). Several scales were used across the included studies to measure attitudes toward the acceptability and/or effectiveness of pharmacological treatments for OUD. The most commonly used scales to measure attitudes were the Abstinence Orientation Scale (AOR; 6 of 70) and the Methadone Knowledge Scale (MKS; 5 of 70) both of which were developed by Caplehorn et al. 111 Other scales included the Harm Reduction Acceptability Scale (HRAS), 50 Harm Reduction Attitudes Questionnaire (HRAQ), 51 and Medication Opinions Survey (MOS). 69
Individual-level and organizational-level characteristics
The most common individual-level characteristic measured among studies in its relations with attitudes toward MOUD was the receipt of MOUD-specific training (39 of 70; 55.7%). Exposure to MOUD was the second most examined factor (36 of 70; 51.4%). Exposure was frequently indicated by experience treating individuals participating in these forms of treatment 41 , 55 or adoption of MOUD within one's treatment program or affiliated program. 53 , 81 The third most common factor was treatment orientation (35 of 70; 50.0%), followed by awareness or knowledge (32 of 70; 45.7%), tenure (29 of 70; 41.4%), educational attainment (26 of 70; 37.1%), barriers to providing treatment (24 of 70; 34.3%), and personal recovery status (16 of 70; 22.9%). Several organizational-level factors were also examined in their relationship with attitudes toward MOUD. Some of the more common organizational factors examined were pharmacological treatment adoption, research involvement, levels of care provided, training resources, use of evidence-based practices, the proportion of staff in recovery, and treatment orientation or culture. 78 , 88
Limitations among included studies
Each study's limitations were considered and categorized as follows: problems with external validity (sampling bias), measurement issues, methodological issues, and reporting issues. By far the most common type of limitation represented among the included studies was problems with external validity (61 of 70; 87.1%). Many studies used sampling frames that limited the generalizability of findings. Studies frequently sampled in such a way that may have led to sampling bias due to the self-selection of health professionals who were more opinionated or interested in MOUD. 50 , 82 Other studies used national samples but excluded relevant work settings such as VA-based centers, opioid treatment programs (a.k.a. methadone clinics), transitional living facilities, private practices, and correctional settings. 75 , 89 Other times only administrators were sampled and asked to respond based on the views of the majority of the staff working at their agency. 51 , 59 , 93
Measurement issues were also somewhat common amongst studies (17 of 70; 24.3%). One noteworthy measurement issue was that several studies asked questions in ways that probed attitudes and beliefs about harm reduction or pharmacotherapy for addiction in general rather than specifically related to the treatment of OUD. 78 , 89 This was especially problematic when studies probed attitudes toward the use of naltrexone. While naltrexone is approved for the treatment of OUD until recently it has more commonly been used to treat alcohol use disorder (AUD). Some studies used items that clearly asked about naltrexone in the treatment of AUD 66 , 75 or OUD 40 whereas other studies used items that probed attitudes about naltrexone more generally without specifically asking about its use in the context of alcohol or opioid addiction treatment. 62 , 81
Another important measurement issue was related to the measurement of use or willingness to use MOUD among NPCs in some studies. 52 , 69 , 73 These studies either measured the “use” of pharmacological treatments among NPCs or intentions to direct clients to take medications used to treat OUD. While NPCs may discuss medication compliance or provide information about medications such as discussing possible side effects and possible benefits, it would be considered outside the scope of an NPC's practice to direct clients to take specific medication to treat OUD, unless it had already been prescribed. This measurement issue may explain why responses to intention items were largely neutral in these studies except for counselors working in methadone treatment programs where it could be assumed that NPCs frequently discuss medication compliance and thus direct clients to take methadone as prescribed.
Findings of included studies
Prescribing professionals
Several studies that sampled primarily prescribing professionals examined the use of methadone and attitudes toward its effectiveness and acceptability (See Table 1). Merrill et al. 54 examined the effects of training related to office-based methadone treatment among a small sample of generalist physicians, all of whom expressed interest in providing office-based methadone treatment. Merrill et al. 54 observed that, after the training, there was an increase in knowledge and positive attitudes toward office-based methadone treatment. Trevor 41 found that providers who more frequently interacted with patients in methadone treatment were more accepting of drug use and less oriented toward abstinence. Abstinence orientation and disapproval of drug use were also strongly associated with one another, and knowledge of methadone treatment was negatively associated with abstinence orientation. 41 Calcaterra et al. 99 found that hospitalist physicians with access to an addictions specialist tended to have more positive attitudes toward agonist treatments including methadone and were more likely to continue prescriptions for MOUD compared to hospitalists without access to an addictions specialist.
Since buprenorphine was approved for the treatment of OUD by the FDA in 2002, many studies have examined attitudes toward buprenorphine and prescribing practices. Studies found that knowledge about buprenorphine, exposure to its use, and attitudes about its effectiveness and acceptability in treating OUD are related to prescribing practices. 64 , 72 , 87 , 91 , 94 , 95 , 110 Certain types of physicians, especially generalist physicians and addiction specialists, tend to be more open to prescribing buprenorphine. 61 , 64 , 72 , 83 , 94 Recent studies have shown that physicians with less tenure tend to have more positive attitudes toward MOUD including buprenorphine and are more likely to express interest in obtaining a DATA waiver compared to more established physicians. 97 , 103 , 107 , 109 , 110 Studies have found that non-physician prescribers (nurse practitioners and physician assistants) are at least as likely to be interested in providing buprenorphine compared to generalist physicians, 71 , 97 although more efforts may be needed to increase their awareness of the waiver process. 102 Recent studies have focused on the initiation of buprenorphine in emergency departments (ED), and have found that most prescribers working in these settings are supportive of ED-initiated buprenorphine. 97 , 102 , 109
Recent surveys of physicians have indicated that they tend to believe that agonist treatments are more effective at treating OUD than extended-release naltrexone and that buprenorphine is slightly more effective than methadone. 100 , 101 However, only 7.6% of primary care physicians sampled as part of a recent nationally representative survey reported prescribing buprenorphine, and even fewer (4.0%) reported prescribing naltrexone for OUD. 100 Even among a sample of prescribers who had recently obtained a DATA waiver or applied for a patient limit increase, one in four had not prescribed buprenorphine since obtaining a waiver and only 13% prescribed at or near their patient limit in the past month. 95
The most commonly endorsed barriers to prescribing buprenorphine include inadequate access to behavioral health, counseling, and other support services; logistical issues such as patient limits, DEA involvement, scheduling, and record-keeping; lack of knowledge about OUD treatment and need for additional training; and concerns about fit with practice and potential changes to the patient mix. 64 , 65 , 76 , 77 , 83 , 86 , 87 , 91 , 92 , 95 , 101 , 109 , 110 Netherland et al. 76 found that prescribers with more experience tend to have fewer concerns about providing buprenorphine treatment, and Suzuki et al. 86 found that those who have received buprenorphine-specific training are less likely to endorse barriers to its use.
Recent studies have examined the effects of various organizational and educational interventions related to the adoption of buprenorphine treatment among prescribers. 96 , 102 , 104 – 106 , 108 Receipt of buprenorphine-specific training is associated with increases in knowledge, positive attitudes about buprenorphine's effectiveness, and intending to or obtaining a DATA waiver. 83 , 86 , 106 , 108 However, evidence indicates that participating in more than one training may be necessary to have an impact on actual prescribing practices based on studies that have examined prescribing at follow-up. 83 , 104 Brackett et al. 105 found that implementing a collaborative care model with integrated behavioral health led to increases in the number of waivered physicians and prescribing within a health care system's five primary care clinics.
Non-prescribing clinicians
Tenure at methadone treatment programs among NPCs, an indicator of exposure, has been associated with more knowledge about methadone and more positive attitudes toward its use. 46 , 69 Exposure to MOUD through program adoption or training has been linked to perceptions of the effectiveness of both methadone and buprenorphine in others types of programs as well. 71 , 75 , 81 , 84 , 89 , 90 , 109 However, even among samples of those working in methadone treatment programs, a substantial minority (∼25%) of NPCs endorsed abstinence orientations and negative attitudes toward methadone. 46 , 69 Being more oriented toward abstinence has been associated with negative attitudes toward methadone. 62 , 89 Many NPCs, especially those who do not specialize in addiction treatment or work in addiction treatment programs, lack knowledge and training about methadone treatment and as a result hold negative attitudes about the acceptability of methadone as a treatment modality. 56 , 62 Studies have found that NPCs are generally split regarding beliefs about whether methadone should be the first-line treatment or if it should only be offered after the failure of alternative treatments. 46 , 49 Even among those who support methadone treatment, many NPCs favor short-term use and believe that those in long-term treatment should be encouraged to withdraw from methadone after achieving stability. 40 , 46 , 51
In perhaps the first study of NPCs’ awareness of and attitudes toward buprenorphine treatment, Knudsen et al. 53 surveyed substance abuse counselors during the two years after it was approved by the FDA, finding that 67% of those sampled did not know enough about it to rate its efficacy. Buprenorphine-specific training, tenure, and personal-recovery status were related to more awareness of its efficacy. 53 Knudsen et al. 53 found a significant relationship between the time since FDA approval and awareness of its efficacy. More recent studies have found that close to 90% of NPCs providing substance abuse treatment can rate the effectiveness of buprenorphine, indicating that diffusion of knowledge related to buprenorphine has reached similar levels to methadone among NPCs. 79 , 89
In several studies, NPCs with higher levels of educational attainment were more likely to have positive attitudes about the effectiveness and acceptability of buprenorphine. 53 , 56 , 112 Attitudes about the effectiveness and acceptability of buprenorphine have been positively associated with receipt of buprenorphine-specific training and exposure to its use in practice. 53 , 80 , 81 , 84 , 112 Abstinence-based treatment orientations are associated with negative attitudes about buprenorphine's acceptability and effectiveness among NPCs. 53 , 65 , 89
Although few studies have examined NPCs’ attitudes toward naltrexone, evidence indicates that many NPCs lack knowledge related to the use of antagonists such as naltrexone and tend to perceive agonist treatments as being more acceptable and effective. 70 , 78 Exposure to naltrexone's use in treatment, tenure in the field, educational attainment, and medication-specific training are positively associated with attitudes toward naltrexone. 78 Abraham et al. 78 found that adherence to or identification with an abstinence-based orientation is negatively associated with perceptions of naltrexone's acceptability and effectiveness. However, Bride et al. 81 found the opposite among their sample; those who endorsed an abstinence-based orientation were more likely to rate naltrexone as effective.
Studies have shown that perceived social norms among NPCs are associated with attitudes and practice behaviors related to pharmacological treatments for OUD. 69 , 73 Varra et al. 73 found that one of the most frequently endorsed barriers to referring clients to MOUD was fears of the views of coworkers. Longer tenure in substance abuse treatment programs has been linked to positive attitudes about pharmacological treatments for OUD, 84 however, NPCs who work in treatment programs that are more oriented toward abstinence are less likely to view MOUD as acceptable. 80 NPCs who work in residential settings tend to have more negative attitudes toward MOUD compared to those who work in other settings. 63 , 68 , 69
Evidence suggests that NPCs tend to prefer MOUD to be combined with adjunctive counseling. Agnew 79 found that buprenorphine with adjunctive counseling was the most preferred treatment modality among a sample of NPCs. Herbeck et al. 74 found that NPCs rated psychosocial treatments as more effective than pharmacological ones; however, few indicated knowing about the effectiveness of specific pharmacological treatments. Aletraris et al. 89 found that NPCs tended to rate the acceptability of buprenorphine higher than for methadone, but still less than for psychosocial interventions.
Administrators
Four studies utilized samples that were primarily made up of administrators (e.g., medical directors, senior clinicians, and clinical supervisors/directors). Among a sample of senior clinical staff and administrators representing 222 substance abuse treatment programs across the United States, Rosenberg and Phillips 51 found that respondents were somewhat accepting of both short-term and long-term methadone treatment, although there was more support for short-term treatment. Most respondents did not endorse reductions in use as an acceptable intermediate goal for the treatment of addiction. 51 The most frequently endorsed reasons for not offering methadone treatment at their agencies were an inconsistency with the agency's treatment philosophy, availability at a nearby agency, and lack of resources to enable its implementation. 51
Rich et al. 59 interviewed medical directors of federal prisons representing 39 states, finding that about half provided methadone to inmates; however, most provided it only during detoxification. Security concerns and administrative opposition were the most frequently endorsed barriers to providing methadone to inmates within federal prisons. 59 Very few respondents reported the practice of referring inmates to methadone treatment upon release, and only about 30% believed methadone was beneficial for inmates with OUD. 59 There was a significant association between attitudes/beliefs and practices, such that those who did not believe methadone to be beneficial were less likely to provide methadone in their facilities. 59
Turner et al. 60 surveyed directors of New York state primary care or human immunodeficiency virus specialty services clinics that serve Medicaid enrollees to examine their attitudes and adoption of buprenorphine and methadone. Only about a third were willing to provide office-based methadone whereas nearly two-thirds were willing to provide buprenorphine in an office-based setting. 66 Attitudes about methadone and buprenorphine were associated with willingness to provide them. 60 Exposure to methadone through affiliation with methadone treatment programs was associated with willingness to provide it. 60 Salient barriers to providing methadone and buprenorphine were lack of knowledge, need for training, lack of social workers or counselors on staff, and concerns about reimbursement. 60
Among a sample of clinical directors and senior clinicians representing agencies that served American Indian and/or Alaskan Native (AI/AN) populations, Rieckmann et al. 93 found that the rate of MOUD implementation among these programs was much lower than the general population of substance abuse treatment programs, indicating that AI/AN individuals may have less access to MOUD. Rieckmann et al. 93 found that treatment philosophy and staff expertise were significant factors for the implementation of MOUD. Programs that reported a perceived gap in the use of evidence-based treatments (EBTs) were less likely to report the adoption of MOUD, showing a clear connection between attitudes toward EBTs in general and the adoption of MOUD. 93
Pharmacists
A few studies examined pharmacists’ attitudes toward MOUD, specifically methadone and buprenorphine. Raisch et al. 58 and Tuchman et al. 48 found that prior to any specialized training in methadone treatment, most pharmacists sampled had positive beliefs about methadone's efficacy and felt comfortable working with patients undergoing methadone treatment. McCarty et al. 52 found that training related to MOUD was effective in improving attitudes about the effectiveness of buprenorphine among a sample that included pharmacists. Raisch et al. 58 found that most (70%) of their sample of pharmacists and pharmacy assistants were willing to dispense buprenorphine to those in treatment for OUD and that only about 20% of those sampled were worried about the additional risk of theft or break-ins due to dispensing buprenorphine or had concerns about diversion of buprenorphine dispensed.
Mixed samples
Several studies utilized mixed samples of different types of health professionals, sometimes comparing attitudes and practices across types of professionals. Caplehorn et al. 45 examined attitudes toward methadone among a mixed sample of professionals working in urban methadone treatment programs, finding that abstinence orientation and disapproval of drug use were strongly correlated among the sample. Those who indicated being in recovery were more likely to endorse an abstinence orientation. 45 Similarly, Fitzgerald and McCarty 75 found at the organizational level that lower percentages of staff in recovery were associated with more support for methadone. Using mixed samples, both Forman et al. 47 and McCarty et al. 68 found that medical professionals tended to be more supportive of MOUD than other types of professionals sampled. McCarty et al. 68 found that managers and supervisors were the most supportive of evidence-based practices such as MOUD whereas support staff was the least supportive. Magrath 40 found that counselors were less supportive of MOUD, especially those which utilize agonists, than medical providers or clients. Among a sample of mixed ED professionals, administrators and nurses were more likely to support ED-initiated buprenorphine compared to physicians, however, nurses were more likely to agree with stereotypes regarding people who use drugs compared to physicians. 98
Studies using mixed samples have found that receipt of training, knowledge, education, tenure, and exposure are associated with more positive attitudes toward the use of MOUD. 45 , 47 , 68 , 75 , 82 Several studies of mixed samples have shown that pieces of training related to MOUD are effective in improving attitudes and increasing practice behaviors related to their use. 50 , 52 , 63 , 66 Furthermore, research has also shown that there is a strong desire for additional training related to MOUD among different types of health professionals. 55 , 85 Other studies have examined whether supplements to educational interventions can improve the efficacy of such pieces of training. In a randomized trial with substance abuse counselors, Varra et al. 73 found that an Acceptance and Commitment Therapy plus educational intervention related to pharmacotherapy was significantly more effective at increasing reported referrals to pharmacotherapy for addiction than an education-only condition. Friedmann et al. 88 examined whether the addition of an organizational linkage intervention improved upon a training related to MOUD and found that both the training and the training plus linkage conditions were associated with increases in familiarity and knowledge of MOUD, but only the training plus linkage organizational linkage condition saw significant improvements in attitudes and intentions to refer. Similarly, Wakeman et al. 113 examined the effects of a hospital substance use disorder treatment initiative that included educational and linkage components, finding that initiative was effective in changing attitudes and practices related to MOUD.
Discussion
Across multiple types of health professionals, studies found that attitudes about the effectiveness and acceptability of using MOUD are related to their implementation. Studies demonstrated that attitudes are associated with prescribing practices of physicians, referrals to programs that offer MOUD by NPCs, participation in dispensing MOUD by pharmacists, and the adoption of MOUD in treatment programs by administrators. Findings from this review indicate that health professionals’ attitudes toward MOUD are a critical consideration in the ongoing implementation of these interventions in OUD treatment. While policy changes and efforts to improve public perception of MOUD are needed to increase access and utilization, steps must also be taken to address negative attitudes that still exist among many health professionals.
Given the importance of health professionals’ attitudes in the implementation, access, and utilization of MOUD, this review also sheds light on factors associated with attitudes. Three related factors were repeatedly found to be associated with more positive attitudes toward MOUD: exposure, training, and knowledge. The significance of these factors across studies of multiple types of health professionals and regarding multiple types of medications used to treat OUD provides evidence that exposure to these treatments in practice and through pieces of training leads to more knowledge which, in turn, contributes to more positive attitudes about the effectiveness and acceptability of MOUD. Consistent with these findings, tenure within the field of substance abuse treatment was also frequently observed to be a factor related to attitudes.
Several studies examined the effects of training on increasing knowledge and positive attitudes toward MOUD. Results from these studies were largely successful, though the pieces of training themselves were heterogeneous in terms of length and content. Furthermore, it is unclear whether training, alone, is sufficient for changing attitudes and practices. Some studies found that linkage efforts are a necessary supplement to training if practices are to be changed. These findings corroborate the most frequently endorsed barriers to implementation.
Office-based settings are important for increasing access and utilization of MOUD. Studies found that efforts to increase office-based buprenorphine have been effective in increasing the number of prescribers ready and able to prescribe buprenorphine, and studies that sampled pharmacists showed that many are willing to be involved in dispensing buprenorphine. However, many prescribers are far below their capacity for office-based buprenorphine treatment. Several studies surveyed prescribing professionals about barriers to prescribing buprenorphine, indicating that several issues still need to be addressed. Two of those barriers seem particularly ripe for research and intervention: inadequate knowledge and training among staff and inadequate access to behavioral health, counseling, and support services. For successful implementation of MOUD, collaboration and communication are necessary between prescribing professionals, pharmacists, administrators, and NPCs. NPCs who provide behavioral health services to individuals with OUD (e.g., social workers, counselors, and psychologists) will need to reach out to prescribers in their communities to facilitate the successful implementation of office-based buprenorphine. Buprenorphine prescribers should also seek to connect with behavioral health providers in their communities to facilitate referrals and increase treatment capacity.
Treatment orientation was also found to be an important factor across many included studies. When health professionals are more oriented toward abstinence, they tend to be less accepting of agonist-based treatments and less likely to assist in their implementation. This was an especially salient factor among NPCs who tended to be more supportive of psychosocial treatments compared to pharmacological treatments. Treatment orientation was also observed to be a significant organizational factor, such that working in a treatment program that was more oriented toward abstinence-based treatment models was related to less positive attitudes among the health professionals working in those programs. This was consistent with findings related to social norms; health professionals’ attitudes tend to be affected by those of their colleagues.
Most of the findings across studies were remarkably consistent regarding the significance and direction of associations between factors and attitudes, with only a couple of exceptions. Findings related to personal recovery status among health professionals were mixed. Those in recovery are to be more likely to be aware of MOUD and to have opinions about them, but there is less evidence that being in recovery is associated with either negative or positive attitudes. The association between educational attainment and attitudes toward MOUD among NPCs was mixed. One explanation could be that educational attainment, as a factor, is less important than exposure, training, and knowledge. Educational attainment is likely associated with attitudes, but only in as much as it indicates exposure, training, and knowledge related to MOUD. Estreet et al. 90 found that the inclusion of training related to harm reduction and MOUD within a social work curriculum led to more positive attitudes. To produce health professionals who are knowledgeable about MOUD and able to assist in their implementation, curriculums must ensure exposure to multiple treatment paradigms including harm reduction.
Limitations
The primary limitation of this review is the possibility of bias due to it having been conducted solely by its author. Ideally, a systematic review should make use of multiple reviewers for search, distillation, and extraction to minimize bias and avoid exclusion of eligible articles. Although the author took great care in these processes, attempting to strictly adhere to inclusion and exclusion criteria, it is important to acknowledge this limitation.
Another limitation of this review was the failure to include sufficient studies that examined attitudes toward naltrexone to allow for meaningful conclusions. Few included studies examined attitudes toward naltrexone, and those which did examine these attitudes tended to do so without differentiating between its use for the treatment of AUD or OUD. The current research regarding attitudes toward naltrexone for use in treating OUD is mixed and inconclusive. Future research should measure attitudes toward naltrexone in a way that differentiates between attitudes about its use for the treatment of AUD versus for OUD. Studies should also compare attitudes about oral naltrexone and injectable naltrexone (e.g., Vivitrol).
Conclusions
This study conducted a systematic review of the last 23 years of research on health professionals’ attitudes toward MOUD. Findings emphasize that attitudes toward MOUD affect access and utilization by influencing prescribing practices, referrals, and adoption within programs. To increase access and utilization, efforts are needed to increase positive attitudes toward MOUD among various types of health professionals. Findings indicate that exposure, knowledge, and treatment orientation are important factors for attitudes toward these treatments and should inform potential interventions. Findings also indicate that future interventions should seek to increase interprofessional communication, especially between prescribers and behavioral health providers.
Footnotes
Acknowledgment
Sherry Cummings reviewed and provided feedback for this manuscript throughout its completion.
Disclosure statement
This work was supported in part by The University of Tennessee's College of Social Work. The funding organization had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.