
Abstract
Background: Travel distance to medication treatment for opioid use disorder (OUD) is a challenge for many patients, but little is known about how distance is associated with medication treatment utilization. This study examines the association between distance to the nearest physician waivered to prescribe buprenorphine and patient-level buprenorphine treatment among West Virginia Medicaid expansion enrollees with diagnosed OUD. Methods: We conducted a cross-sectional spatial analysis with 2016 Medicaid claims data, separately examining individuals living in metropolitan and non-metropolitan areas. We calculated the driving distance from the centroid of patients’ residential ZIP codes to the street address of the nearest waivered physician derived from the 2015 Drug Enforcement Administration listing. Regression models examined the association between distance and initiation and duration of buprenorphine (among those initiating). Results: We focused on 8,008 individuals with OUD in 2016. The nearest waivered prescriber in metropolitan areas was an average of 7.13 miles away from patients’ residential ZIP codes and 14.54 miles in non-metropolitan areas. The providers they actually visited were a mean of 33.63 miles away in metro areas and 46.36 in non-metropolitan areas. In multivariable analyses, compared to those living <10 miles from a waivered physician, living >20 miles from a waivered physician was associated with −32.13 fewer days of treatment (95% CI: −57.86, −6.40) in metro areas and −16.70 fewer days in non-metro areas (95% CI: −32.32, −1.08). Conclusions: Longer travel distance to buprenorphine treatment is associated with a shorter duration of care that is likely to be clinically meaningful.
Background
The United States is in the midst of an unprecedented crisis related to opioid addiction and overdose. 1 One of the main public health challenges has been increasing access to effective treatment for opioid use disorder (OUD). OUD is a chronic condition that can be effectively treated with the Food and Drug Administration-approved opioid agonist medications methadone and buprenorphine. 2 Methadone for OUD can only be provided by licensed opioid treatment programs, while buprenorphine can be provided by clinicians with a federal waiver to prescribe buprenorphine. The waiver was limited to physicians until the passage of the Comprehensive Addiction and Recovery Act (CARA), which became effective in 2017 and has allowed nurse practitioners and physician assistants to prescribe buprenorphine. 3 Clinicians with a waiver were previously required to complete a training program (8 h for physicians and 24 h for advanced practice practitioners), but this requirement was rescinded in 2021 by the US Department of Health and Human Services. 4
Only about one-fifth of all individuals with OUD receive any treatment and treatment often does not include medications. 5 Given the high risk of overdose that accompanies premature treatment discontinuation, recent national quality guidelines propose at least 180 days of pharmacotherapy for OUD. 6 Most patients do not achieve this treatment length. 7 , 8 Under-utilization of medication treatment may reflect inadequate access to treatment providers. The number of clinicians waivered to prescribe buprenorphine for OUD and treatment facilities that offer medication treatment for OUD (MOUD) has grown over time, 9 but many areas lack enough providers to meet the demand for medication. Access in rural communities has been particularly limited, 10 and many rural patients need to travel long distances to receive MOUD. 11
Several recent studies document issues related to geographic proximity to treatment. Recent studies have found that most Americans live close to buprenorphine prescribers and that waiver growth has been highest in areas with a high overdose burden. 12 There are clusters in the US, particularly in the Midwest and South, where treatment provider availability is low, 13 , 14 including areas where overdose burden is high. 15 Additionally, several older studies (mostly published before the current opioid crisis) found that greater travel distance is associated with under-utilization of treatment for substance use disorders, commonly, non-medication counseling programs. For example, a study from Baltimore city found clients traveling even relatively small distances were less likely to complete treatment. 16 A study conducted in the Veteran's Administration of individuals completing residential treatment found that continuity of care was substantially lower for patients located farther from aftercare treatment sources. 17 Studies from Spokane County, Washington found that patients who initiated methadone maintenance missed fewer doses if they lived closer to the treatment program. 18 , 19
Particularly relevant to the current opioid crisis in rural communities, a recent study of rural Pennsylvania Medicaid enrollees with diagnosed OUD found that every additional mile of distance from a treatment provider was associated with a 1.2% reduction in the odds of receiving medication treatment. 20 Patients lived a median of 4.2 miles from a waivered prescriber but traveled a median of 48.8 miles to their treatment programs. Longer travel distance was associated with substantially lower continuity of medication treatment.
The cumulative evidence suggests that travel distance could be a critical barrier to initiating and persisting in buprenorphine treatment, but several questions remain unanswered. First, while studies such as the one from Pennsylvania point to the difficulty of accessing treatment in rural areas, differences between rural and urban areas are not well characterized in the literature. 11 In general, we expect people in rural areas to live farther from treatment, 21 but it may be that patients in rural areas either have more adaptations to longer travel distances (e.g., greater vehicle ownership) or greater willingness to travel. On the other hand, urban patients may have access to better transit infrastructure, including public transit. 22 These differences are well-documented in the health care utilization literature, 23 , 24 but are less well understood for substance use treatment. Second, we separately examine the initiation and continuity of buprenorphine treatment, since travel distance could independently influence both outcomes. Specifically, travel distance could deter patients from getting an initial consultation, but could also present a burden for patients returning to the clinic for continuing prescriptions. Third, we wanted to examine travel distance in the context of high-volume prescribers. Specifically, buprenorphine treatment is known to be highly concentrated within a small group of waivered prescribers treating most patients, and many active waivered prescribers treat few patients. 25 Given this, we expected many patients to bypass nearby physicians to travel to high-volume physicians that might be in other parts of the states.
With these questions in mind, we examine the relationship between travel distance to the nearest buprenorphine waivered physician and the utilization of buprenorphine treatment among adults with diagnosed OUD enrolled in West Virginia Medicaid. West Virginia has the highest opioid overdose death rate among all states 26 and is a good state to compare urban-rural differences, as it is a state where most people live outside urban areas. 27 West Virginia Medicaid did not cover methadone maintenance until 2018, 28 thus buprenorphine was the only covered opioid agonist medication during the 2014–2018 period.
We focus on differences in buprenorphine utilization within small geographic areas, stratifying our analysis between metropolitan and non-metropolitan areas. Because many waivered physicians do not actively prescribe 29 or impose substantial barriers on entry or decline to accept Medicaid, 30 we hypothesized that many individuals would receive treatment from physicians far from their home as their nearest waivered physician may not be accepting patients for buprenorphine treatment. We expected driving distances to the most commonly visited physicians to be longest in rural areas. We also hypothesized that a greater driving distance from a waivered physician would be associated with lower initiation rates of buprenorphine treatment and shorter duration of treatment, however, we were uncertain about whether similar patterns would exist between metropolitan and non-metropolitan areas.
Methods
Our study used two data sources. West Virginia Medicaid claims from the calendar year 2016 focused on individuals in the Medicaid expansion were used to construct both patient-level treatment outcomes and to identify practices most frequently visited for OUD treatment. To identify the closest physician waivered to prescribe buprenorphine, we used the list of physicians who held a waiver to prescribe buprenorphine in West Virginia from the US Drug Enforcement Administration as of October 2015. This database includes a street address for the clinic location.
With the Medicaid data, we focused on individuals enrolled in the Medicaid expansion in the calendar year 2016 who had at least one claim with an OUD diagnosis (ICD-10 code F11.X) in any setting and who were enrolled for at least 10 months of the calendar year (n = 8,318). Enrollment in the Medicaid expansion was defined using the state's eligibility category code. We excluded 310 individuals who could not be linked to five-digit residential ZIP code for a final sample of 8,008. Individuals with OUD in our data were located in 714 unique ZIP codes (as a reference, the mean area of a West Virginia ZIP code is about 34 square miles). 31 We created indicators for demographics (age, sex, race/ethnicity, comorbidities). We defined buprenorphine treatment as filling at least one pharmacy claim for buprenorphine with a three-digit hierarchical identification code for buprenorphine (HIC3: H3W). We excluded any formulations indicated exclusively for pain management (e.g., the transdermal buprenorphine patch). We also counted the total number of non-overlapping days of buprenorphine prescribed to the patient in the year (i.e., we did not allow for stockpiling of medication between refills). The study protocol was approved by the Johns Hopkins School of Public Health Institutional Review Board.
We considered several patient-level covariates that could independently influence measures of treatment utilization and choice of primary provider: age, sex, race/ethnicity (non-Hispanic white, non-Hispanic black, Hispanic, or other), and presence of a comorbid diagnosis, including diagnoses of hypertension, hyperlipidemia, atherosclerosis, asthma, chronic obstructive pulmonary disease, arthritis, depression, anxiety disorder, bipolar disorder, hepatitis C, HIV/AIDS, and chronic pain. Diagnoses were identified with International Statistical Classification of Diseases and Related Health Problems (ICD-10) codes and represent common chronic conditions among Medicaid enrollees with OUD. 32
We used the claims data to also identify locations of where individuals receiving buprenorphine treatment were most likely to get the majority of their care from a buprenorphine prescriber. Because pharmacy claims did not identify the buprenorphine prescribing physician, we used as a proxy the provider with the most services with an associated procedure code of evaluation and management (E&M) (CPT 99XXX) and a diagnosis code of OUD. Half the sample (50.1%) visited two or more providers and received a service in which an OUD diagnosis was recorded. In these cases, we defined the primary provider rendering the greater number of visits. All patients in our sample with buprenorphine fill had some outpatient records with an OUD diagnosis, but in some cases they did not have a physician office visit that was attributable to a specific physician. When patients lacked any claims with an OUD diagnosis and an E&M code, we used the provider that provided the most counseling (CPT codes 90791, 90792, 908.X and HCPCS codes H0004, H0031, H0036, H0040, and H2036) visits.
For purposes of calculating travel distances, we first identified the ZIP code tabulation area (ZCTA) that corresponds to their ZIP code. ZCTA provides spatial boundaries that allow for geographic mapping, whereas ZIP codes are used for mail delivery routes and are not organized by spatial points. However, ZCTA and ZIP code are generally the same in an area, and we found every ZIP code for a person in our data was mappable to a ZCTA (we generally refer to the geographic unit as the ZIP code for simplicity). 33 Next, we approximate a residential address using the geographic center of the ZCTA, these centroids are made available by the US Census Bureau. 33 We then calculated the driving distance between the centroid of the ZCTA and the location of a physician or clinic using the gmapsdistance package in R. Gmapsdistance uses the Google Maps Distance Matrix API in order to compute the distance of the recommended driving directions between two points, and places points on the nearest road when latitude and longitude are provided. 34
Once we had calculated all driving distances, we proceeded to examine the association between driving distances and patient outcomes. Given our hypothesis that the relationships would be different in core urban areas versus rural areas, we stratified the sample in all analyses between individuals with residences in ZIP codes within metropolitan statistical areas (MSAs) and non-MSA based on the patient's county of residence using a federal definition of non-MSA areas. 35 Because some ZIP codes cross county boundaries, we assigned ZIP codes to the county where the plurality of the residents reside. 36
In unadjusted analysis, we examined the driving distance to the practices most frequently visited for OUD treatment. We also examined the concentration of patients overall within these practices by plotting the share of patients associated with the largest practices in the state. We created a ZIP code-level choropleth map of the distance to the nearest waivered physician. We calculated the mean, median, and interquartile range for driving distances to the nearest waivered physician (irrespective of whether the patient in fact visited these physicians). We compared differences in study outcomes and demographics based on whether individuals resided <10, 10–20, >20 miles from a waivered physician, stratifying by metro versus non-metro residents. Categories were chosen to be readily interpretable and to reflect meaningful groupings in the data. Sensitivity analyses considering other measures of distance (including continuous distance) produced similar results.
We estimated regression models where the main predictor was driving distance category to the nearest buprenorphine prescribing physician separately for the two main study outcomes: use of any buprenorphine treatment and, among patients filling a buprenorphine prescription, number of days filled. We used logistic regressions for our binary outcome and calculated predicted margins, which can be interpreted as the predicted difference in the outcome associated with the predictor in percentage points, holding other variables at their mean. We selected ordinary least squares (OLS) as the preferred specification for the continuous measure of days filled because this outcome was not highly skewed and OLS is easily interpreted. Models adjusted for individual-level predictors that may independently be associated with treatment outcomes: age, sex, race/ethnicity, and presence of comorbidities. We clustered standard errors at the ZIP code level to account for autocorrelation within areas.
Results
Table 1 displays the mean and median distances in driving miles to the closest buprenorphine prescribing physician and to the primary provider that the patient visited for OUD treatment. The data are shown overall for the sample and then stratified by metro and non-metro residency. Overall, individuals lived a mean distance of 10.08 miles to a buprenorphine prescribing physician. The distance was 7.13 miles in metropolitan areas and 14.54 miles in non-metropolitan areas (p < 0.01 for difference). However, in practice, individuals traveled much longer distances to treatment: the most commonly visited provider was located 38.73 miles away on average (median = 21.9 miles) from patients with OUD. Travel distances were notably higher in non-metro areas than metro areas (46.36 miles versus 33.63, p < 0.01). Figure 1 shows the geographic variation in mean driving distances to the nearest buprenorphine waivered physician in West Virginia at the ZIP-code level. Travel distances were longer, on average, in eastern parts of the state, including mountainous areas near the Virginia and Maryland borders.
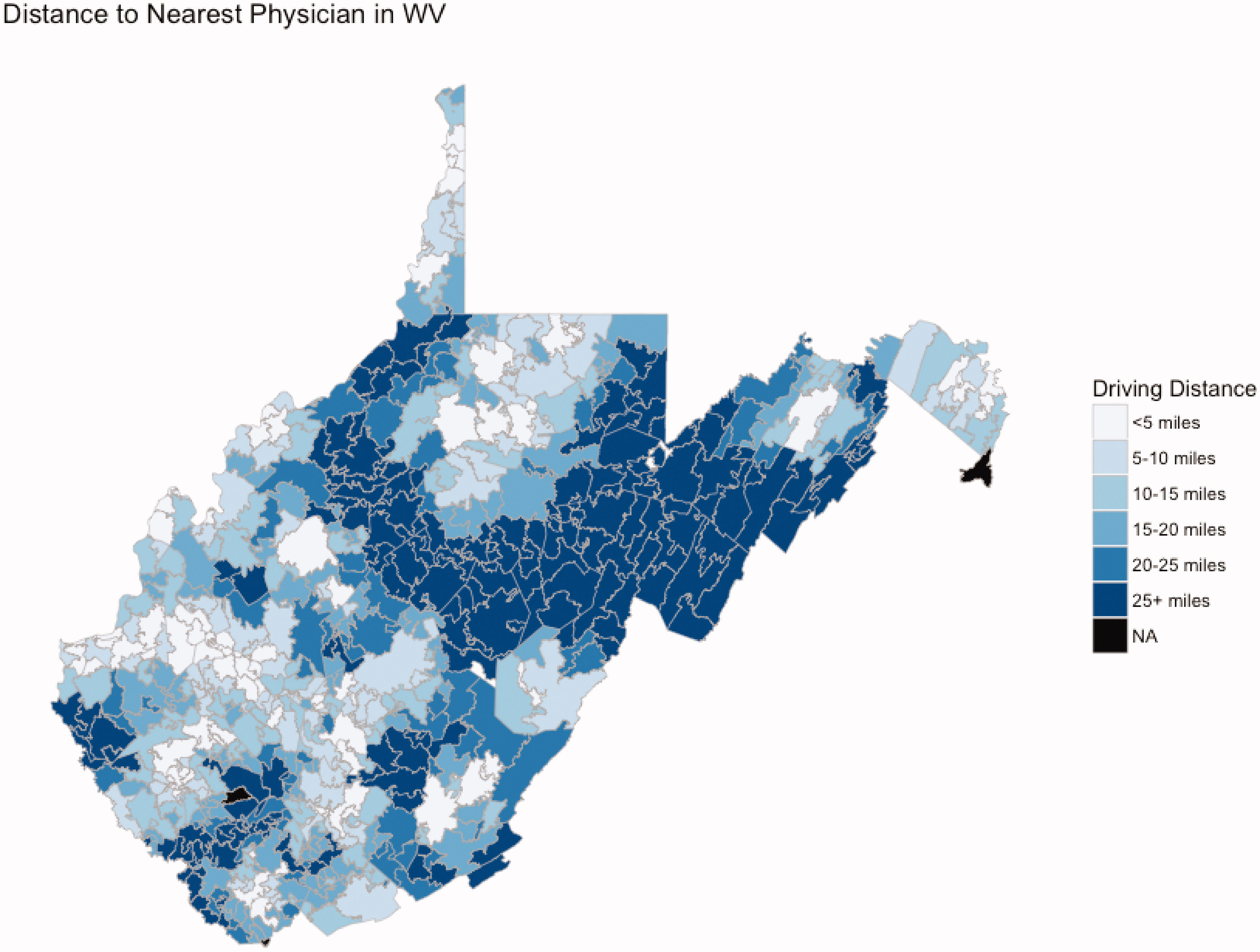
Driving distance to the nearest buprenorphine waivered physician in 2016. Notes: figure visualizes driving distance to nearest waivered physician from the centroid of each ZIP code in West Virginia in October 2015.
Travel Distance to Nearest Buprenorphine Prescriber and To Most Commonly Visited OUD Treatment Provider.
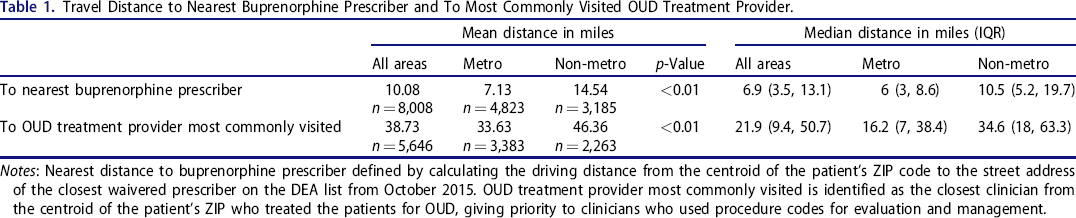
Notes: Nearest distance to buprenorphine prescriber defined by calculating the driving distance from the centroid of the patient's ZIP code to the street address of the closest waivered prescriber on the DEA list from October 2015. OUD treatment provider most commonly visited is identified as the closest clinician from the centroid of the patient's ZIP who treated the patients for OUD, giving priority to clinicians who used procedure codes for evaluation and management.
Table 2 displays unadjusted descriptive characteristics of the study population stratified by metro and non-metro areas and by travel distance to providers. In metro areas, individuals living closer to the nearest treatment provider were significantly more likely to be nonwhite but were otherwise similar. No significant differences were detected by individual characteristics in non-metro areas. In metro areas, roughly 4 out of 10 individuals with an OUD diagnosis received any buprenorphine and there were no significant differences in the use of buprenorphine based on distance category. Among those receiving buprenorphine in metro areas, there were no significant unadjusted differences in the number of days filled for those living <10 miles from treatment versus 10–20 miles. However, there was a significant difference for those living >20 miles away versus <10 miles. Individuals living within 10 miles of a waivered physician also traveled much shorter distances to their actual treatment provider.
Unadjusted Descriptive Characteristics of Individuals with an Opioid Use Disorder Diagnosis Stratified by Distance to the Nearest Waivered Physician, 2016.
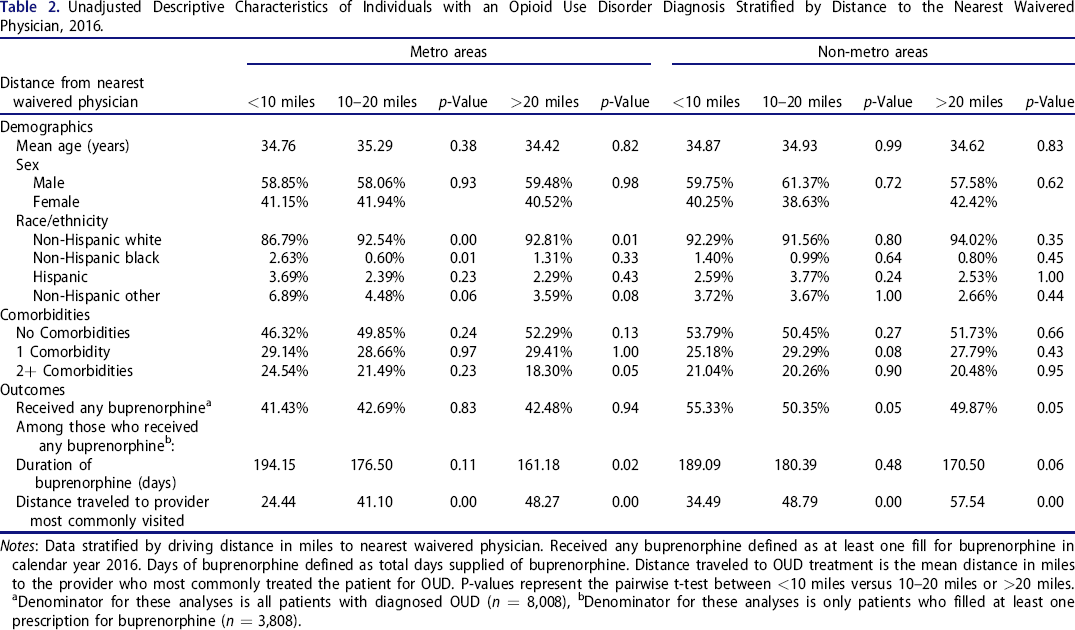
Notes: Data stratified by driving distance in miles to nearest waivered physician. Received any buprenorphine defined as at least one fill for buprenorphine in calendar year 2016. Days of buprenorphine defined as total days supplied of buprenorphine. Distance traveled to OUD treatment is the mean distance in miles to the provider who most commonly treated the patient for OUD. P-values represent the pairwise t-test between <10 miles versus 10–20 miles or >20 miles. aDenominator for these analyses is all patients with diagnosed OUD (n = 8,008), bDenominator for these analyses is only patients who filled at least one prescription for buprenorphine (n = 3,808).
In non-metro areas, more than half of all individuals with an OUD diagnosis received any buprenorphine, and buprenorphine use was higher for individuals living closer to treatment. Among those receiving buprenorphine, there was no significant difference in days filled with medication between those living <10 miles from a prescriber and 10–20 miles from a waivered. There was a notable, but non-significant, difference between <10 miles versus >20 miles (189.09 versus 170.5, p = 0.06). There were also significant associations between distance to nearest waivered physician and mean distance traveled to treatment.
Figure 2 illustrates the concentration of patients prescribed buprenorphine among the providers treating Medicaid patients with OUD. Overall, there were 347 total primary providers who saw all Medicaid expansion patients with OUD in West Virginia. Roughly one quarter (26.49%) of all patients were primarily seen by 9 providers (2.5% of all OUD treating providers), one half (49.68%) were seen by 25 providers (7.2% of all providers), and three quarters (74.63%) were seen by 59 providers (17.0% of all providers).
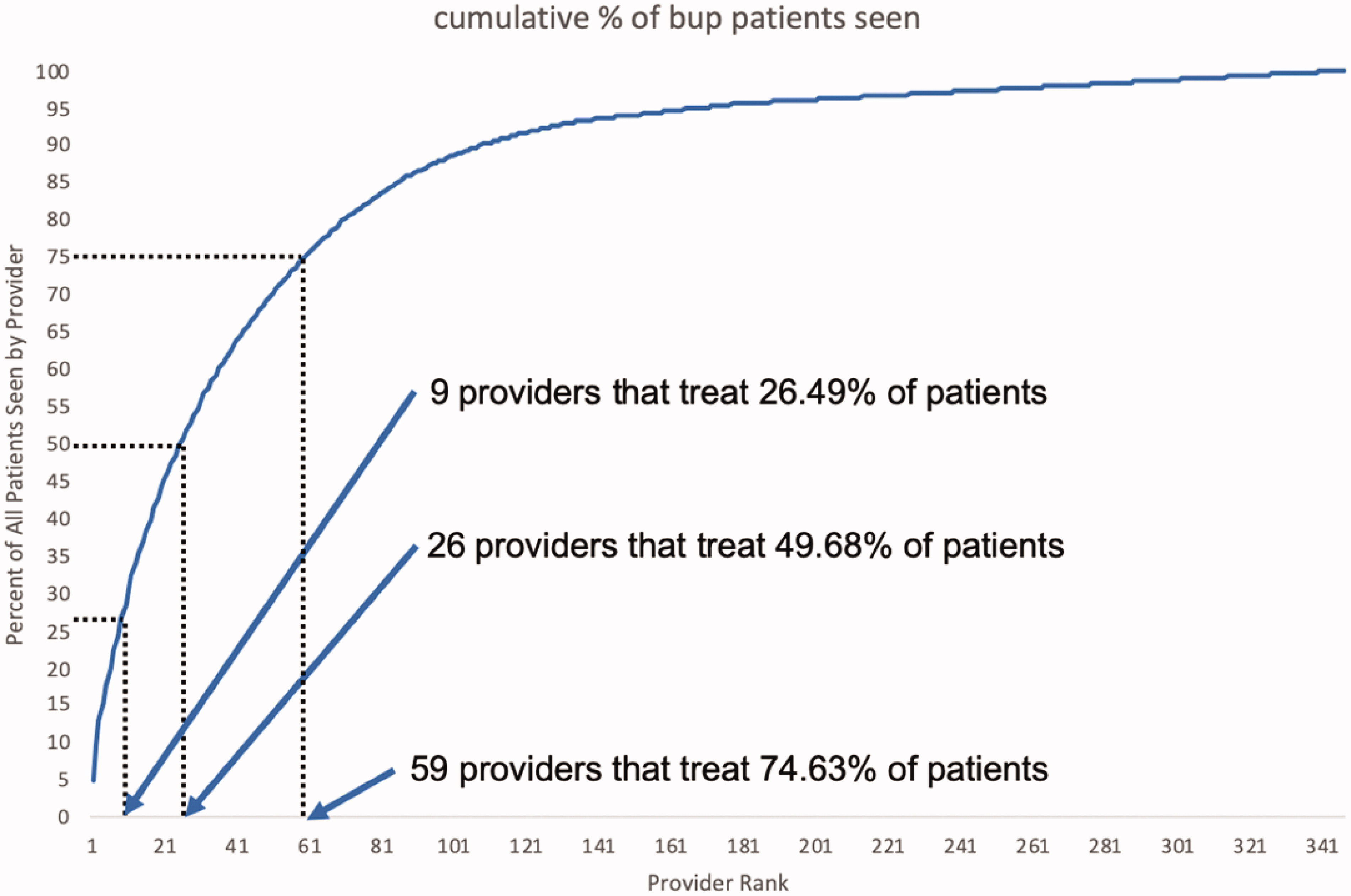
Cumulative percent of patients prescribed buprenorphine seen by providers treating opioid use disorder.
Table 3 displays multivariable regression results examining the effect of living 10–20 or >20 miles from the nearest waivered physician on the probability of receiving buprenorphine and the duration of buprenorphine use compared to people living within 10 miles stratified by living in a metro versus a non-metro area and adjusting for patient, age, sex, race/ethnicity, and for the presence of chronic conditions. Among enrollees with OUD living in metro areas, there was no association between living >10 miles from the nearest waivered physician and probability of any buprenorphine treatment (10–20 miles: 0.01 (95% CI: −0.04, 0.05); >20 miles: 0.00 (95% CI: −0.08, 0.08)). However, among those who received buprenorphine in metro areas, living farther away from a waivered physician was associated with significantly fewer days of filled buprenorphine. Compared to those living <10 miles from a waivered physician, individuals located >20 miles from treatment received 32.13 fewer days of treatment per year (95% CI: −57.86, −6.4).
Regression Estimates Predicting Receipt and duration of Buprenorphine Associated with Distance to the Nearest Waivered Physician.
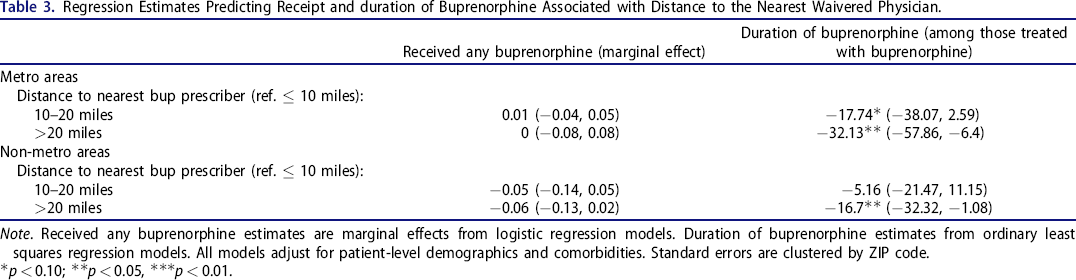
Note. Received any buprenorphine estimates are marginal effects from logistic regression models. Duration of buprenorphine estimates from ordinary least squares regression models. All models adjust for patient-level demographics and comorbidities. Standard errors are clustered by ZIP code.
p < 0.10;
p < 0.05,
***p < 0.01.
In non-metro areas, there was a suggestive, but not statistically significant, association between distance from the nearest waivered physician and probability of using any buprenorphine (smaller sample sizes for these non-metro areas resulted in wider confidence intervals). For example, the point estimate was a 5 percentage point (0.05) lower probability of receiving any buprenorphine for those living 10–20 miles from treatment, versus those living <10 miles from treatment (95% CI: −0.14, 0.05). Compared to <10 miles, being located >20 miles from treatment in non-metro areas was associated with fewer days of filled medication (−16.7 days, 95% CI: −32.32, −1.08). Compared to the mean of 189.09 for the <10 miles group, this represents a decrease of 8.3%.
Discussion
We explored the relationship between driving distance to physicians and utilization of buprenorphine treatment using 2016 claims for individuals with diagnosed opioid use disorder (OUD) in West Virginia. We found that living far from a waivered physician was associated with a shorter duration of buprenorphine treatment. There are likely to be several pathways underlying this association. People who need to travel farther may have greater difficulty maintaining continuity of care due to the time burden and expenses of travel to physician visits. Travel distance has been shown to be an impediment to continuity of OUD care in prior studies, particularly in rural areas. 37 There are also area-level factors that may influence the relationship between access and quality, including more limited health and social services that support individuals seeking treatment for OUD.
We found that most individuals with OUD lived relatively far from waivered physicians—a mean of about 7 miles in metro areas and 15 miles in non-metro areas. While proximity to treatment is associated with the receipt of more buprenorphine, patients do not necessarily go to the nearest prescriber. The providers that individuals actually visited for treatment were located substantially farther away—individuals who lived in metro areas traveled an average distance of 34 miles and those in non-metro areas traveled an average distance of 46 miles. It is likely that the nearest waivered physician may not be willing to treat the patient, as most waivered physicians prescribe buprenorphine well below their authorized patient caps and, according to one study, about 42% treat no patients over many years. 38 In another recent national study, waivered physicians treated a median of only 8.3 patients per month. 39 Moreover, a substantial share of buprenorphine prescribing physicians do not accept Medicaid and about one quarter only serve cash-paying patients. Even when physicians do accept new Medicaid-enrolled patients, they sometimes require a referral from a substance use disorder clinic or defer treatment to after an intake evaluation, delaying and discouraging treatment “on demand.” 30 All of these factors may lead patients to seek care from a smaller group of physicians who are known to provide easier access to buprenorphine and explain why patients may be willing to travel further distances for care. 40
Long travel distance to treatment is likely to detract from patient health and wellbeing. Patients needing to travel farther to treatment may be discouraged from starting buprenorphine treatment and experience difficulty sustaining treatment. Previous research finds that overdose risk decreases and symptoms remit with additional time spent in buprenorphine treatment. 7 , 41 The importance of medication has increased in recent years due to the emergence of highly potent illicit fentanyl that has accelerated overdose rates in West Virginia and other states. 42 Longer travel distance also imposes meaningful costs to patients from missed work, child care expenses, and money spent on fuel or transit fare. Patients in rural areas and outlying areas of cities are especially burdened by travel distance and often lack public transit options. 43 In West Virginia, Medicaid patients receiving buprenorphine are also required to attend counseling sessions, which may further increase the challenges of accessing and sustaining treatment. Major national guidelines now encourage patients to start buprenorphine even where counseling may not be available. 2
Several policies have been advanced to encourage the geographic availability of buprenorphine treatment. The 2017 CARA policy has allowed more non-physician clinicians to gain a scope of practice and has contributed to the supply of waivered clinicians in rural areas. 44 Federal initiatives such as the State Opioid Response and State Targeted Response grants have made investments in the expansion of the workforce to prescribe buprenorphine. 45 Local health systems and initiatives have also expanded waiver training. These efforts have increased the number of waivered clinicians with, the number of waivered clinicians more than doubling between 2016 and 2019. 46 During the COVID-19 pandemic, the US Department of Health and Human Services enacted emergency regulations that allowed for greater use of telehealth and waived the requirement that first prescriptions for buprenorphine be written in a face-to-face visit. 47 The broadened use of telehealth likely buffered access during the pandemic, 48 – 50 and long-term could be a particularly beneficial solution for patients residing in areas with long travel distance to a waivered prescriber but requires additional rulemaking to sustain these changes, adequate reimbursement, and networks of local clinicians who can partner with telehealth prescribers.
Several study limitations should be considered. First, our measurements of the waivered physician workforce and their practice locations are subject to error. While we drew on the comprehensive DEA list from late 2015, we do not capture clinicians who joined the workforce during 2016. The office addresses provided in the DEA file may also not fully reflect where physicians provide care, as some physicians operate from multiple locations. Likewise, imputing the centroid of a ZIP code is an imperfect measure of patient residential address. Second, our measure of driving distance may not reflect the real travel burden for individuals, including those without access to a vehicle who are reliant on public transportation or those who live in remote or mountainous areas. Third, our measure of provider most visited for OUD treatment among buprenorphine patients may not necessarily reflect the physician who prescribed buprenorphine, although we focused on procedure codes likely to be used by physicians prescribing buprenorphine. However, we did not require the provider to be a waivered physician. Fourth, our study does not capture the use of services that take place out-of-state, though West Virginia Medicaid generally does not reimburse for out-of-state care. 51
Conclusion
Travel distance is a critical element of access to care for patients with opioid use disorder. Focusing on a heavily rural state with a severe opioid crisis, our study shows that a longer distance to the nearest waivered physician was associated with a shorter average duration of treatment. Increasing access to treatment is an urgent policy priority, and requires a clearer identification of nearby locations where patients will be able to obtain treatment. Improving spatial availability of care can help to reduce meaningful barriers for patients and ultimately promote their recovery from opioid use disorder.
Footnotes
Authors’ contributions
BS conceptualized the study, supervised the research, and took the lead in writing the manuscript. RKL and RJ led the data analysis. BS, RKL, RJ, BDS, CLB provided critical feedback and contributed to the writing of the manuscript.
Disclosure statement
The authors have no conflicts of interest to disclose. The funding source had no role in the design of this study and will not have any role during its execution, analyses, interpretation of the data, or decision to submit results.