
Abstract
Background: Pharmacist stigma via examination of social distance preference and negative attitudes toward persons who misuse opioids is prevalent and may lower the quality of care provided to patients. Few studies have previously extended beyond the immediate post-intervention period to examine stigma change. Methods: This longitudinal cohort study utilized a pre-survey administered before the training program, a post-survey immediately upon completion of the training program, and a delayed post-survey, administered 12 months after the training program. Co-primary outcomes were changes in social distance scale (SDS) total score from baseline to post-survey and from baseline to 12 months. Secondary outcomes included change in SDS question scores and change in negative attitudes. One hundred eighty-seven of the 1211 eligible pharmacists in the state completed the training. Matched responses of forty-four pharmacists who completed all three surveys were examined. Results: The mean total SDS score was significantly lower in the immediate post-training survey than the pre-training mean (14.75 vs. 16.57, p = .000). The 12 months mean total SDS score was also significantly lower than the pre-training mean (15.32 vs. 16.57, p = .017). Significant changes in negative attitudes from baseline to post-survey and from baseline to 12 months were seen. Conclusion: Stigma reduction components integrated into opioid training decreased pharmacist social distance preference and negative attitudes toward patients who misuse opioids immediately after the training and, most notably, were sustained for 12 months.
Introduction
Stigma is defined as a “mark” that is associated with the attribution of negative characteristics, discrediting, and unjust rejection. 1 It involves stereotypes (harmful and disrespectful beliefs about a group), prejudice (agreeing with the stereotype leading to emotional and evaluative consequences), and discrimination (the behavioral result of prejudice). 2 Health-related stigma occurs when individuals or groups are devalued based on a socially discredited health condition. 3 , 4 Among the most discredited conditions are substance use disorders (SUDs), also known as the stigma of addiction. 5
When healthcare professionals carry stigma 6 – 8 the care they provide is associated with poorer access, poorer quality, early care discontinuation, decreased patient safety, and decreased help-seeking behavior. 9 – 11 Healthcare provider stigma toward addiction is particularly concerning given the opioid crisis and increase in fatal drug overdoses during the COVID-19 pandemic. 12 , 13 Reduction of stigma is critical to remove barriers to high-quality care for individuals who misuse substances.
Prior research has shown it may be possible to reduce the stigma of addiction amongst healthcare providers. 3 , 14 , 15 Yet, just three studies have examined stigma change beyond the immediate post-intervention period. 14 , 16 , 17 A larger body of literature has illustrated reductions in stigma among healthcare providers related to other mental illnesses and it is possible those lessons can be applied to the reduction of the stigma of addiction. 18 Approaches that include the provision of factual information, contact with and portrayal of persons as successfully treated, and encourage non-stigmatizing language, motivational interviewing, and sub-conscious bias examination may hold promise. 18 – 23
The Social Distance Scale (SDS), measures stigma via the assessment of preference for separation from an individual with a particular characteristic. 1 , 24 Social distance preference is a central element of stigma. 25 Unlike recent social distancing measures employed as COVID-19 mitigation strategies, in this context social distance preference indicates attribution of undesirability leading to separation and/or rejection of individuals or groups. The SDS has been used to measure stigma among healthcare providers 26 , 27 with excellent reliability and validity. 1 , 28
The ONE Program [Opioid and Naloxone Education; formerly (ONE Rx)], a grant-funded non-profit program, equips pharmacists to screen patients for opioid misuse and overdose risk, deliver opioid-related interventions, and reduce opioid-related harms. 29 – 31 It was implemented with a training for pharmacists. 32 Researchers identified stigma of pharmacists as a potential barrier to program implementation. Thus, components were added to target stigma reduction and measure stigma change. The hypothesis was the training would reduce social distance preference and negative attitudes toward persons who misuse opioids but those reductions would disappear by 12 months.
Methods
This study utilized a longitudinal cohort design and pre-, post-, and delayed post (after 12 months) surveys. The co-primary outcomes changed in SDS total score from baseline to post-survey and delayed post-survey. Secondary outcomes included change in SDS question scores and negative attitudes from baseline to post-survey and delayed post-survey.
Sample
The sample consisted of licensed pharmacists enrolled in ONE Program training (https://one-program.org/). 33 All practicing pharmacists in North Dakota (n = 1211) were invited by email to participate in the training in person or on-demand online between October 2018 and August 2019. No incentives were used to encourage participation, however, the training and associated 3 h of continuing education were provided at no cost.
Training
Objectives, educational topics, methods, and practice-based outcomes of the ONE Program training have been previously published. 29 , 34 Nine training modules (Online supplement 21 , 23 , 32 – 37 ), were completed all at once if in-person, or at a self-directed pace if online.
Stigma reduction focus areas of the training included: biopsychosocial aspects of opioid misuse and opioid use disorder (OUD); depiction of opioid misuse and OUD as preventable, treatable conditions; and modeling of communication approaches, such as stigma-free language use. The content was designed from the integrative pedagogical perspective, 38 encouraging participants to make connections between new concepts and previous experiences with application to situations in their professional lives. Verbal explanation and diagram representation of information, application exercises, self-reflection/examination, drawing analogies, role-play, and video demonstration were used in content delivery. Stigma reduction content encompassed 1.25 h of the 3 h training.
Survey design
The 26-item pre-survey assessed baseline stigma, current practice behaviors, and attitudes of pharmacists. Six of these questions were derived from the original 7-item SDS. We eliminated the question: “How would you feel about being a worker on the same job as someone like _____?” to arrive at six SDS questions. This was done to avoid confounding that could be associated with an impaired colleague working in a pharmacy environment. Also, 2 SDS questions related to conversing with a vignette person were modified to represent pharmacist-patient interactions for relevance to participants. For the SDS survey questions, a vignette of an individual displaying opioid misuse was designed by author 1 (Table 1) based on previously published vignettes. 20 , 39 A 5-point Likert scale was utilized; 1 = definitely willing to 5 = definitely unwilling. The 6 SDS question scores were added to give a total SDS score (maximum of 30) with higher scores, especially those above the midpoint (>15), representing a greater preference for social distance from patients with opioid misuse. 40 – 42
Social distance scale scores before (pre-training), immediately after (post-training), and 12 months after (delayed post)training (n = 44 matched respondents).
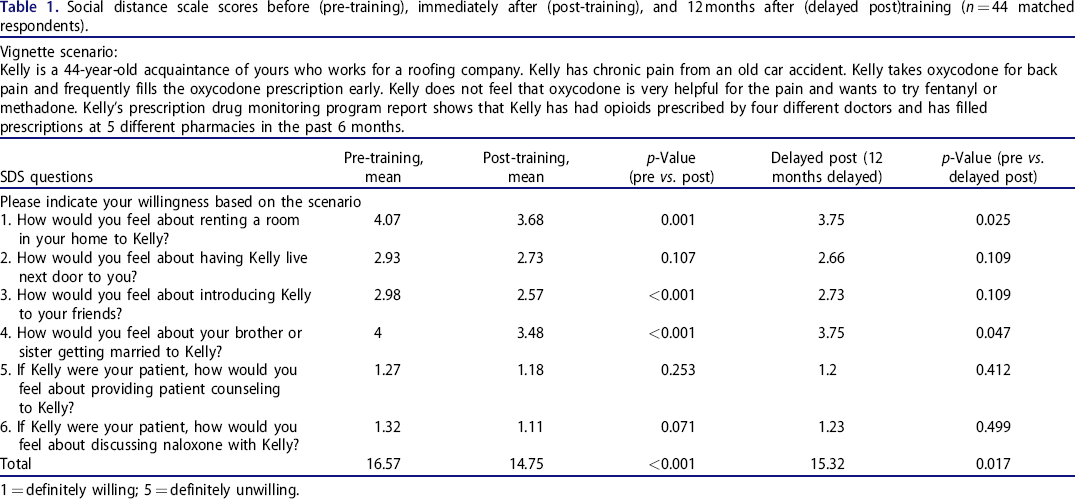
1 = definitely willing; 5 = definitely unwilling.
Thirteen questions assessed pharmacists’ demographics, experiences, current practice behaviors, and attitudes toward opioids/naloxone and patients who use them. Only the 6 questions pertaining to attitudes are reported here; those pertaining to experiences and practice behaviors are reported elsewhere. 34 A 5-point Likert scale was utilized; 1 = strongly agree to 5 = strongly disagree. This portion of the survey was based on a previously developed and validated survey. 29
The post and delayed post-surveys were identical to the pre-survey with the exception of demographics questions, which were asked only in the pre-survey. Results of the pre-survey, including baseline social distance preference, have been published in detail. 43
Survey administration
Pharmacists who enrolled in ONE Program training completed the pre-survey before the training. The post-survey was administered immediately upon the conclusion of the training. Pharmacists attending one of the three live sessions completed pre-post surveys on a paper form. Pharmacists completing online training completed the pre-post surveys electronically using Qualtrics; they were granted a link only after completing the training in its entirety, ensuring all modules were completed before the post-survey was initiated. Twelve months following the last live training session delayed post-survey invitations were emailed to training completers. Three email reminders were sent at 2-week intervals and a paper copy was mailed one month after the final email reminder. Survey participation was voluntary and all survey procedures were approved by the Institutional Review Board at North Dakota State University.
Data analysis
Survey results were matched by participant identifier. Students, retired pharmacists, and pharmacists practicing outside of North Dakota were excluded from the analysis to ensure results reflected practicing pharmacists participating in direct patient care. Participants not consenting to research participation, duplicated entries, those missing a name, and those with <75% survey completion were also excluded. Paired two-tailed two-sample t-tests assessed the significance of changes from pre-survey to post-survey and pre-survey to delayed-post-survey across the matched participant responses. Statistical significance was set at alpha <.05.
Results
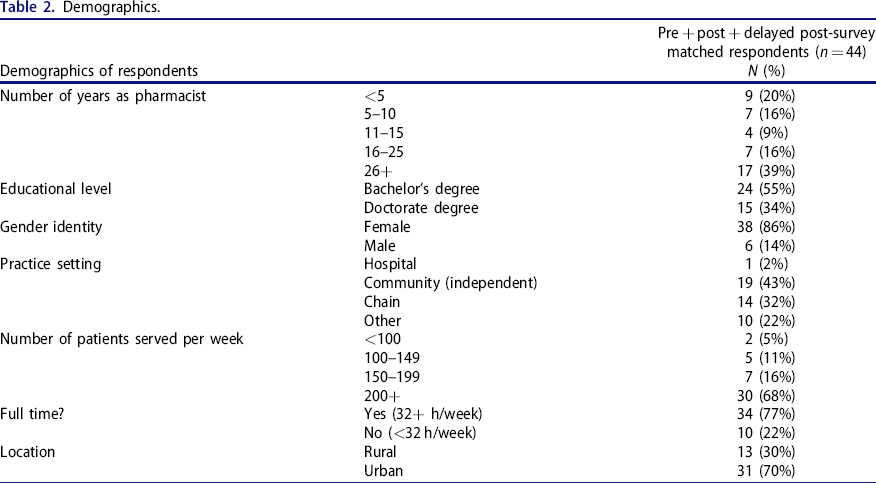
Forty-four pharmacist participants completed all three surveys and their responses were matched across time points. No exclusions were required due to retired or student participants. The majority of these 44 participants were female, had been in practice for more than 15 years, and practiced in urban community or chain pharmacy settings (Table 2). These 44 participants were representative of the larger sample of pharmacists who completed at least 1 survey (n = 187), with no statistically significant differences in demographics from the original sample except for among respondents completing all three surveys, a greater proportion of doctoral degrees (p < .001) and community practice setting (p = .020).
Demographics.
The mean total SDS score was significantly lower in the immediate post-training survey than the pre-training mean (Table 1). The delayed post-survey mean total SDS score was also significantly lower than the pre-training mean. The effect size for the pre- to post-training difference in means was Cohen's d = 0.64, and the pre- to the delayed post-training difference in means was 0.40, which are moderate effect sizes. Mean scores for 3 of the 6 SDS questions were significantly lowered from pre- to post-training surveys. Pre-training to delayed post-training comparisons indicated statistically significant reductions in scores for these same questions with one exception (Table 1).
Responses to some attitudinal survey items showed statistically significant change in the direction of improved attitudes from pre to post-survey and delayed post-survey (Table 3).
Responses to attitude survey questions (n = 44 matched respondents).
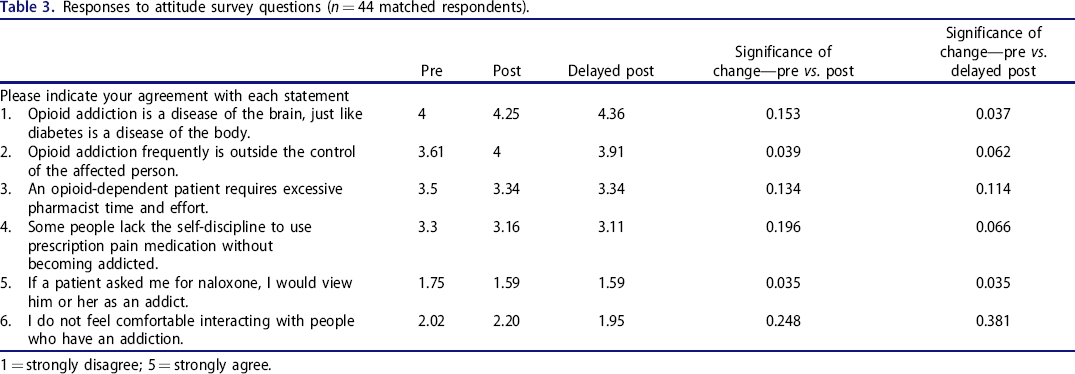
1 = strongly disagree; 5 = strongly agree.
Discussion
This is the first report of reductions in social distance preference of pharmacists in relation to opioid misuse and the first to report a sustained reduction in social distance preference and negative attitudes persisting after 12 months. The significant reduction in SDS mean total scores is an important marker of the pharmacists’ increased willingness to engage with the patient with opioid misuse immediately after completing the training, but perhaps more importantly, extending 12 months after the training.
Patient-centered care requires pharmacists to exhibit open attitudes and behaviors for continued trust development with the goal of improving patients’ well-being. 44 Thus, a significant reduction from baseline immediately after the training and 12 months later suggests a sustained adjustment in the pharmacists’ willingness to engage with, form relationships with, and care for patients with opioid misuse. Significant changes in attitudes immediately after, and 12 months after the training further support this. Individual SDS question scores and attitudinal items that were not associated with significant change after the training (Table 1) tended to have a lower endorsement of social distance preference or negative attitude at baseline and thus were, perhaps, less likely to respond to the interventions in the training.
The design and findings in this study stand out from other interventions aimed at reducing the stigma of addiction among healthcare providers. The focus on stigma toward opioid misuse among pharmacists and examination of attitudes and stigma in healthcare professionals after 12 months are unique. Also, the design of the training in this study did not include contact-based intervention, yet was still associated with lowered social distance scores and improved attitudes. Furthermore, the design of the current study featured stigma reduction training incorporated within other skills training. Perhaps this helped pharmacists to directly apply the stigma reduction principles to their practice. This is consistent with the integrative pedagogical perspective 38 employed in this study and is supported by previous reports from police officers and certified alcohol/drug abuse counselors. 17 , 28 Future work aimed at reducing health professionals’ stigma could consider stigma reduction training coupled with other role-related skills training when the environment is not optimal for contact-based interventions.
This study has limitations. It was designed to study stigma toward a patient with opioid misuse rather than OUD. Some items assessed attitudes toward addiction (i.e., OUD) rather than opioid misuse. Though the differences between opioid misuse and OUD were explained during the training, pharmacists may have confounded the two conditions, which could have impacted the survey results. Potentially stigmatizing terms (e.g., addict) representative of common vernacular in the local community were used in the surveys to avoid confusion with undefined/unfamiliar language (e.g., the person with a substance use disorder) when the pre-survey was administered. This was justified given that in subsequent iterations of the survey, pharmacists would have been trained to recognize the negative attitude as well as the stigmatizing language present in the survey questions. Thus negative attitudes and stigmatizing language use would be expected to change in the same direction. The use of a small convenience sample of pharmacists likely interested in the topic of opioids introduces bias and may mean these data are not representative of less interested pharmacists. Future work may consider the use of a control group, which would allow for longitudinal assessment of attitudinal and/or stigma change in a usual practice environment, clarifying the impact of training itself on these parameters. This study also did not include an evaluation of patient perspective or patient-level outcomes based on pharmacist stigma change; which are important future directions.
In summary, we found stigma reduction components integrated into opioid misuse and OUD training decreased pharmacist social distance preference and negative attitudes toward patients who misuse opioids. These reductions were noted immediately after the training and were sustained for 12 months.
Footnotes
Author contributions
MS and HE conceived of the continuing education and upstream opioid prevention initiative. AW conceived of the idea of measurement of pharmacist stigma within the larger initiative. MS, HE, ES, AW, JS, and OF managed and contributed to the operation of the initiative as well as data collection and analysis. AW took the lead in writing this manuscript. AW, MS, HE, ES, JS, and OF provided critical feedback and contributed to the writing of the manuscript.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.