
Abstract
Background: Caregiving for persons with substance use and/or mental health disorders (SU/MHD) and other conditions places significant strains on caregivers. Methods: The present study used Behavioral Risk Factor Surveillance System (a US health survey) data to (1) compare caregivers of recipients with SU/MHD to those of recipients with other conditions on demographic and caregiving characteristics and health outcomes and (2) examine demographic and caregiving characteristics that were associated with poorer health outcomes among caregivers of persons with SU/MHD. Results: Caregivers of people with SU/MHD were more likely than other caregiver groups (of recipients with medical, cognitive, developmental disability, and old age–related conditions) to report poor general health, physical health, and mental health, as well as activities limitations, having been diagnosed with depression, and binge drinking. Among the group of caregivers of recipients with SU/MHD, those caring for a parent were more likely to report poor physical health, poor mental health, depression, and binge drinking than those caring for a friend, relative, child, or spouse. In addition, caregivers who provided SU/MHD-related caregiving for a longer duration and for whom caregiving included household help were less likely to report poor mental health, depression, or binge drinking. Conclusions: Findings underscore the importance of the substance use disorder treatment system developing improved institutional and structural support for caregivers of recipients with SU/MHD.
Introduction
Caregivers are essential for individuals with substance use and mental health disorders (SU/MHD). Caregiving by family members and friends meets recipients’ needs such as safety, food, housing, and treatment engagement. 1 However, caregiving for persons with chronic conditions such as SU/MHD also significantly strains caregivers. 2 – 4 Studies of caregiving for persons with SU/MHD have generally examined caregiving for this type of care recipient in isolation from caregivers of other types, such that it is unclear how caregivers of persons with SU/MHD compare to caregivers of other types. The present study fills this gap by using Behavioral Risk Factor Surveillance System (BRFSS) data 5 from the US Centers for Disease Control and Prevention (CDC) to compare caregivers of persons with SU/MHD to other groups of caregivers on demographic, caregiving, and health status characteristics and to examine potential predictors of poorer health in this subgroup of caregivers. Poor health among caregivers needs to be identified and addressed to help caregivers in need. Indeed, caregivers’ needs have not been routinely addressed by the substance use treatment system in particular. 6 , 7 Identifying and meeting caregivers’ needs is also important because caregivers’ well-being may impact the outcomes of care recipients. 8
Caregiving for recipients with SU/MHD
Little research has compared caregivers of persons with SU/MHD to other caregivers. Gupta et al. 9 used data from a representative European sample to compare caregivers of persons with schizophrenia to non-caregivers and caregivers of adults with other conditions such as Alzheimer's disease, cancer, and stroke. Caregivers of persons with schizophrenia were more likely to experience poor quality of life and mental illness (depression, anxiety) and medical (sleep difficulties, pain) conditions. Another study found that caregivers assisting veterans with both posttraumatic stress disorder and dementia, compared to caregivers assisting veterans with dementia only, reported more difficulties understanding care recipients’ problems and more physical strain. 10
These comparisons are supported by studies examining only caregivers of persons with SU/MHD. Among caregivers of persons with opioid use disorder, burdensome aspects of caregiving were mental illness (depression, hopelessness, anxiety, worry, fear) and financial strains, family disruption, and work–life imbalance. 11 A review of studies of caregivers of patients with bipolar disorder found that a majority of participants reported mental illness symptoms, such as depression and anxiety, and increased mental health services utilization. 12 A review of caregiving for individuals with schizophrenia found that caregivers provided direct care, daily living assistance, and emotional, social, and financial support. 13 These caregivers felt overwhelmed, stressed, drained, burdened, frustrated, and angry; experienced depression and anxiety; and used more medical care resources than non-caregivers did. 13 Longer duration of illness and of care, severe or persistent schizophrenia symptoms, and financial strains intensified caregiver burden. 13 A synthesis of African qualitative studies of caregivers’ experiences caring for relatives with mental illness found that caregivers felt physically and emotionally burdened, stigmatized, and socially isolated and did not know how to seek help. 14
Despite this body of research, questions about caregiving for care recipients with SU/MHD remain. Accordingly, the present study examined how caregivers caring for persons with SU/MHD compared to those caring for persons with other conditions on demographic and caregiving characteristics and health outcomes. It also examined which demographic and caregiving characteristics were associated with poorer health outcomes among caregivers of persons with SU/MHD. These findings are important because they inform systems of substance use and mental health treatment regarding the need to provide services (and what types of services) for caregivers to improve their health and health practices.
Methods
Data source and sample
This study is a quantitative secondary data analysis of the 2019 BRFSS. The BRFSS is a cross-sectional and nationally representative telephone survey of the civilian, non-institutionalized population aged 18 years and older. It is conducted annually by the CDC with state health departments in the 50 US states and the District of Columbia. About 450,000 adults who are randomly selected for the survey each year are asked a core set of health-related questions. In addition, states have the option to include BRFSS-supported modules on specific topics. In 2019, 10 states included the BRFSS module on caregiving. This study focused on the subsample of participants who completed the BRFSS module on caregiving.
Measures
BRFSS respondents in the 10 states from which data were used in the present study were asked for demographic information: gender, age, race/ethnicity, marital status, children in the home <18 years old, education, employment, health insurance status, military veteran status, and urban/rural location.
The module on caregiving asked the following: During the past 30 days, did you provide regular care or assistance to a friend or family member who has a health problem or disability? Of 34,880 valid responses, 22.3% (n = 7781) said yes and 77.4% (n = 27,099) said no. Not included were 260 invalid responses from participants who were not sure, who refused to answer, or whose care recipient had died in the past 30 days.
Caregivers (those who had said yes) were asked the following: What is the main health problem, long-term illness, or disability that the person you care for has? For this study, 14 response categories were collapsed into 5 for ease of analysis and presentation: (1) SU/MHD (i.e., substance abuse/addiction/mental health disorders; n = 346), (2) medical (arthritis/rheumatism, asthma, diabetes, heart disease, HIV, other organ failure or disease, chronic respiratory condition, cancer, injury; n = 2657); (3) cognitive impairment (Alzheimer's disease, dementia, or other cognitive impairments; n = 1102); (4) developmental disability (n = 249), and (5) old age (n = 1005). Respondents who answered “other” or “do not know/not sure” or refused to answer were not included in this study.
Respondents who were caregivers were asked the following: What is the care recipient's relationship to you? For this study, the 16 response categories were collapsed into 5 for ease of analysis and presentation: parent (mother, father, mother-in-law, father-in-law), child or grandchild, spouse or partner, other relative (brother, brother-in-law, sister, sister-in-law, grandparent, other relative), and friend.
Caregivers were also asked, “For how long have you provided care for that person?” and, “In an average week, how many hours do you provide care or assistance?” Response options for these questions are listed in Table 1.
Caregiving characteristics and outcomes by recipient category: SU/MHD (n = 346), medical (n = 2657), cognitive (n = 1102), DD (n = 249), and old age (n = 1005).
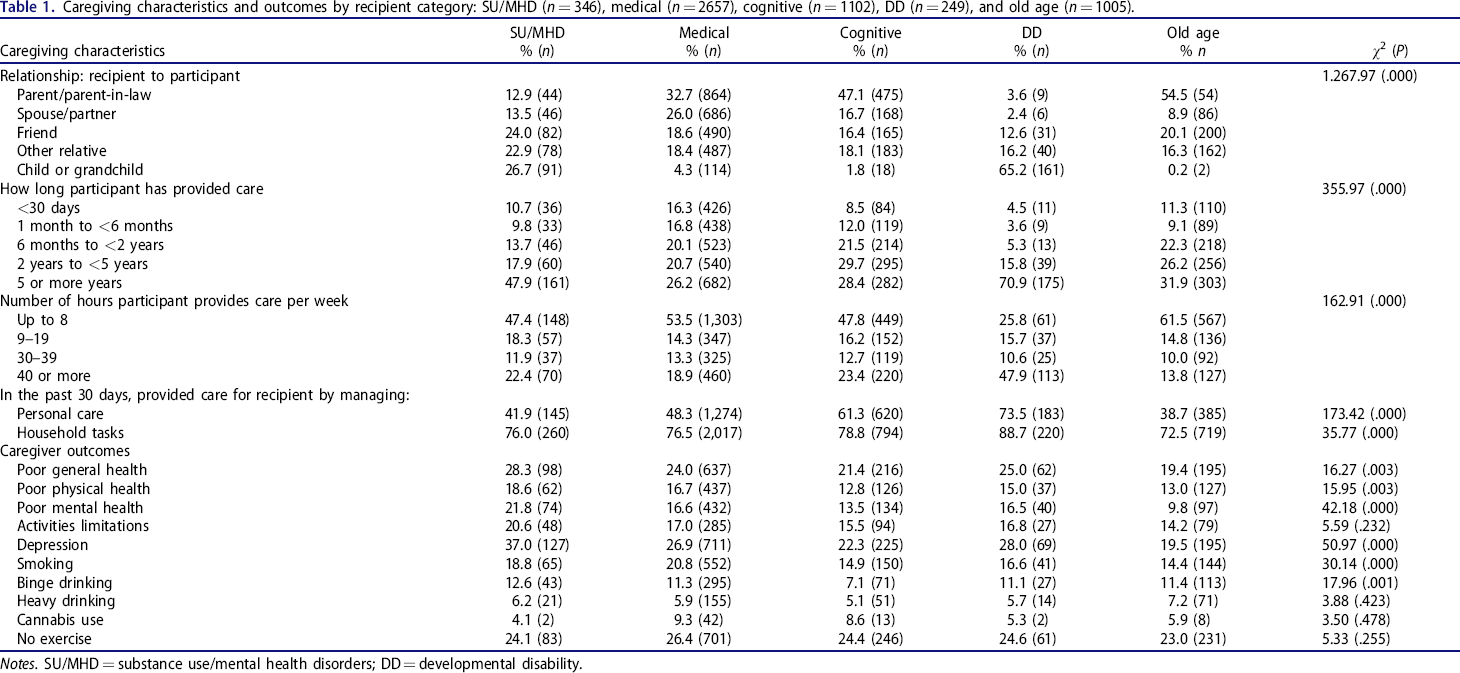
Notes. SU/MHD = substance use/mental health disorders; DD = developmental disability.
Caregivers were asked whether, in the past 30 days, they provided care by managing personal care (giving medications, feeding, dressing, or bathing) and, in the past 30 days, whether they provided care by managing household tasks (cleaning, managing money, or preparing meals). Response options were no or yes.
Respondents were asked to rate their health in general on a 5-point scale. Poor general health was indicated by respondents’ reports that in general their health was fair or poor rather than good, very good, or excellent.
Respondents were instructed to think about their physical health and for how many days during the past 30 days their physical health was not good. Using a BRFSS-created variable, poor physical health was indicated by reports that respondents’ physical health was not good for 14 days or more.
Respondents were instructed to think about their mental health (stress and emotional problems) and for how many days during the past 30 days their mental health was not good. Also using a BRFSS-created variable, poor mental health was indicated by reports that respondents’ mental health was not good for 14 days or more.
Respondents were asked how many days, out of the past 30, poor health kept them from doing their usual activities. Activities limitations were indicated by reports that respondents were kept from usual activities for 14 days or more.
Respondents were asked whether a health professional ever told them they had depression, major depression, dysthymia, or minor depression. Response options for depression were no or yes. Respondents’ smoking was dichotomized as no (do not smoke cigarettes at all) or yes (smoke cigarettes every day or some days). Respondents were asked: Considering all types of alcoholic beverages, how many times during the past 30 days did you have 5 or more drinks for men or 4 or more drinks for women on an occasion? Binge drinking was assessed as no (0 times) or yes (1 or more times). As calculated in the BRFSS, heavy drinking was men having >14 and women having >7 drinks per week. Respondents’ cannabis use during the past 30 days was assessed as no (used it 0 days) or yes (used it ≥1 days). Respondents were asked: During the past month, other than your regular job, did you participate in any physical activities or exercises? They were assessed as having no exercise when they answered no rather than yes.
Analyses
We conducted chi-square analyses to compare caregivers of persons with SU/MHD to caregivers of persons with medical, cognitive, developmental disability, or old age–related conditions. These analyses compared the groups on their demographic and caregiving characteristics and health outcomes. Next, we conducted logistic regressions to examine demographic and caregiving correlates of outcomes of caregivers of persons with SU/MHD. For these analyses, outcomes were limited to 4 key conceptual domains in the caregiving literature of poor physical health, poor mental health, depression, and binge drinking. Two logistic regression models were analyzed for each outcome. In one model, all demographic characteristics were entered simultaneously, thus adjusting for all demographics in the same model. In the second model, all caregiving characteristics were entered simultaneously, thus adjusting for all caregiving characteristics in the same model. For each model, adjusted odds ratios (AORs) were calculated, measuring associations between the independent variables and outcomes. Analyses were conducted with IBM SPSS Statistics (Version 27).
Results
Caregivers’ demographics, caregiving characteristics, and outcomes
Table 2 compares caregivers with different types of care recipients on demographic characteristics. We focus on how caregivers of recipients with SU/MHD compare to other caregivers. Like other caregivers, those caring for recipients with SU/MHD were likely to be female, 45–64 years old, White, married/partnered, and college graduates. Of those whose care recipient had SU/MHD, 34.1% had minor children at home, compared to 24.6% or less of the other groups (except for the developmental disabilities group). Over one-half of caregivers of people with SU/MHD (53.6%) or with developmental disabilities (61.4%) were employed, in contrast to other caregivers, of whom about 46% were employed in each group.
Demographic characteristics of caregivers by recipient category: SU/MHD (n = 346), medical (n = 2657), cognitive (n = 1102), DD (n = 249), and old age (n = 1005).
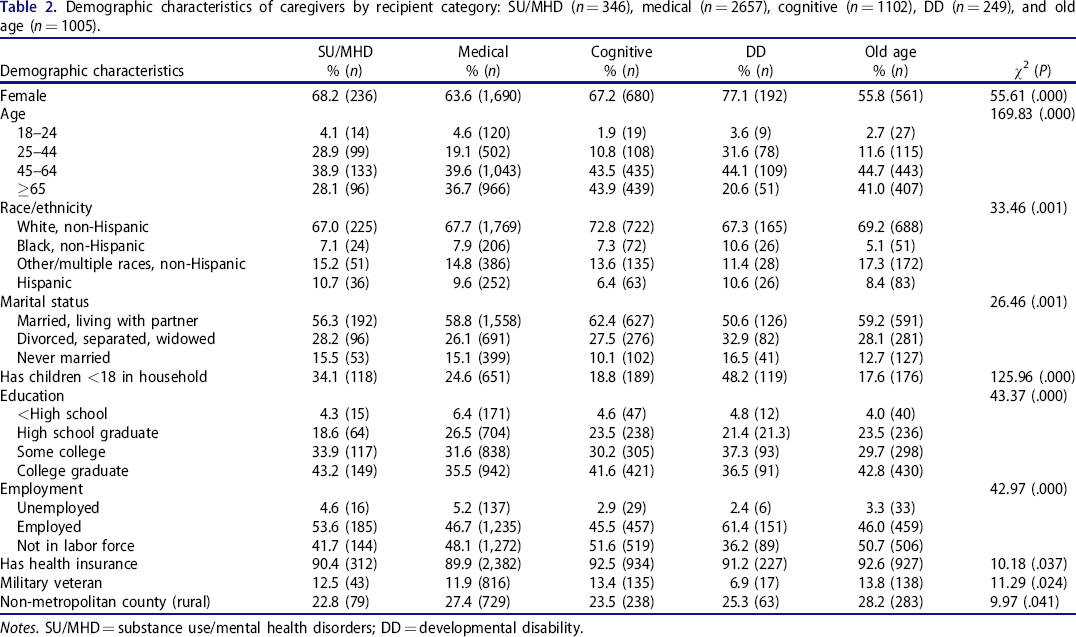
Notes. SU/MHD = substance use/mental health disorders; DD = developmental disability.
Table 1 presents comparisons of caregivers on caregiving characteristics. Among caregivers of recipients with SU/MHD, the recipient was most often a child or grandchild, followed by friend or other relative and then by spouse or parent. In contrast, for the medical, cognitive, and old-age groups, the recipient was most often a parent. Among the SU/MHD caregivers, 47.9% had provided care for 5 or more years, whereas lower percentages of the medical, cognitive, and old-age groups had done so. About one-half of caregivers in the SU/MHD (47.4%), medical (53.5%), and cognitive condition (47.8%) groups provided up to 8 hours of care per week, whereas 61.5% of caregivers in the old-age group did so. Caregivers for people with SU/MHD were relatively unlikely compared to the medical and cognitive groups to provide personal care, but similar to these and the old-age groups on managing household tasks; 76.0% of caregivers of people with SU/MHD managed household tasks. Caregivers of people with developmental disabilities appeared to be a unique group.
Table 1 compares caregivers on health outcomes. Caregivers of people with SU/MHD were most likely to report poor general health, physical health, and mental health; activities limitations; depression; and binge drinking. While 18.8% of this group smoked, smoking was more prevalent only in the medical caregiver group.
Correlates of poor functioning among SU/MHD caregivers
Table 3 presents regressions predicting poor physical and mental health from demographic characteristics among caregivers of persons with SU/MHD. Only being a college graduate was associated with a lower likelihood of poor physical health. A higher likelihood of poor mental health was associated with being female, not married, and a military veteran. A lower likelihood of poor mental health was associated with being older and Black or Hispanic, having children in the household and more education, being employed or not in the labor force, having health insurance, and living in a rural area.
Logistic regressions of caregivers of people with SU/MHD (n = 346) predicting poor physical and mental health.
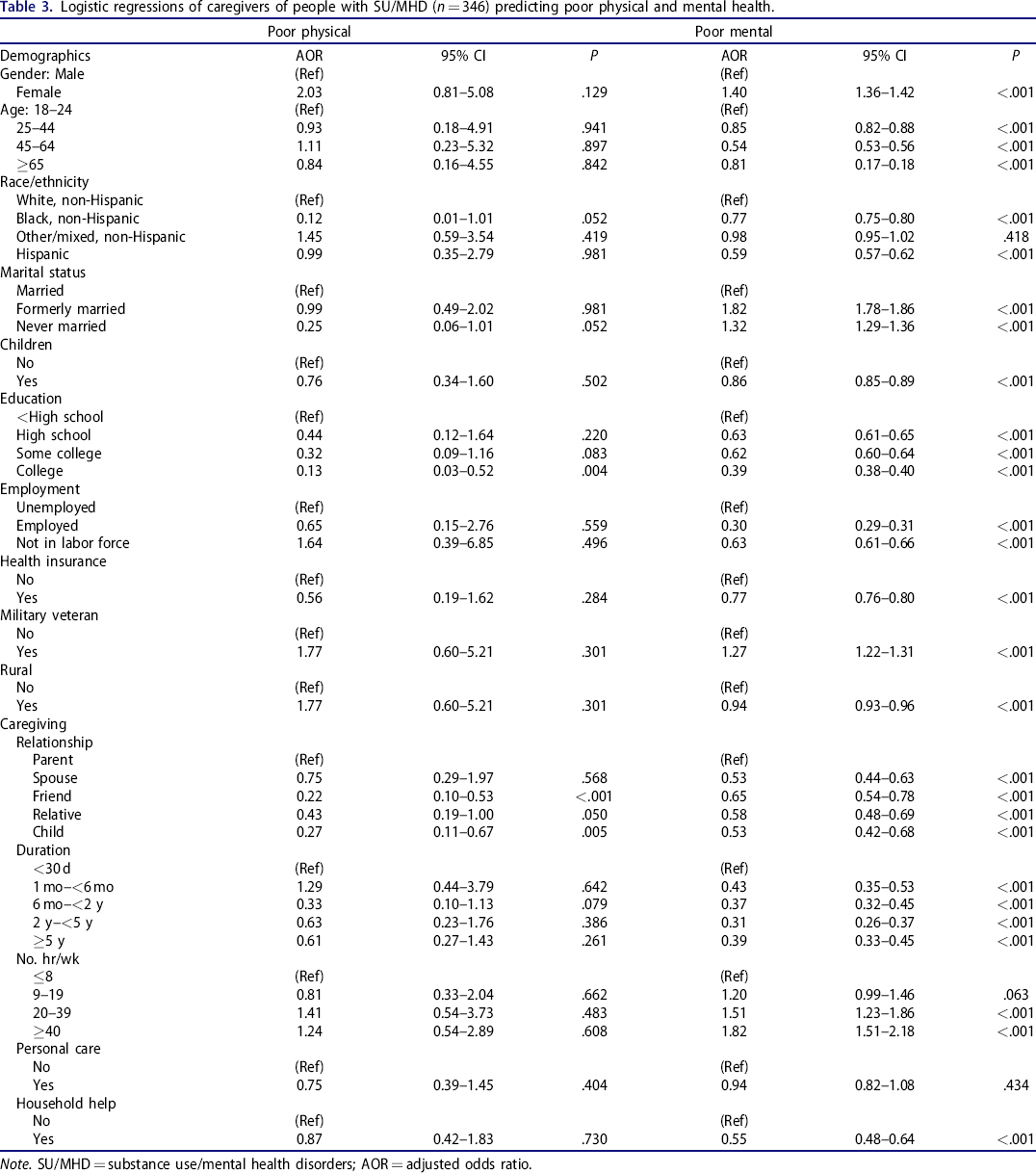
Note. SU/MHD = substance use/mental health disorders; AOR = adjusted odds ratio.
Table 3 also presents regressions predicting poor physical and mental health from caregiving characteristics among caregivers of persons with SU/MHD. Caregivers caring for a friend or child were less likely to experience poor physical health than caregivers caring for a parent. Caregivers of a spouse, friend, relative, or child with SU/MHD were less likely to have poor mental health than caregivers of a parent with SU/MHD. Caregivers who provided caregiving for a longer duration and for whom caregiving included household help were less likely to have poor mental health.
Table 4 presents regressions predicting depression and binge drinking from demographic characteristics among caregivers of persons with SU/MHD. Depression was more likely among respondents who were female and not married and military veterans. Depression was less likely among caregivers who were at least 45 years old and not White, had children in the household, were more educated and employed or not in the labor force, and lived in a rural area. Among caregivers of persons with SU/MHD, those who were not married were more likely to binge drink. In contrast, binge drinking was less likely among caregivers who were female, were older than 25 years, were not White, had children in the home, had more education, were not in the labor force, had health insurance, and lived in a rural location.
Logistic regressions of caregivers of people with SU/MHD (n = 346) predicting depression and binge drinking.
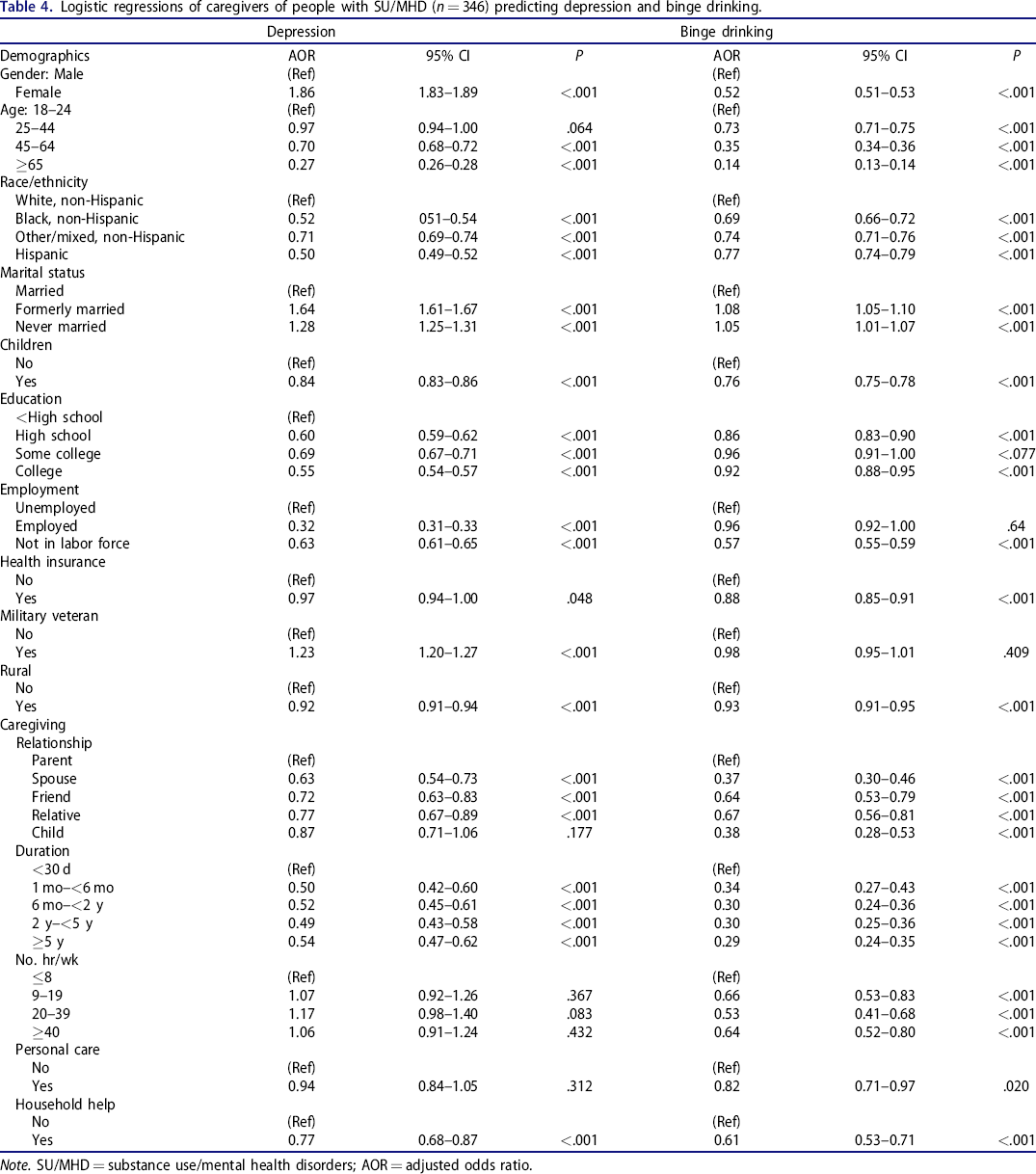
Note. SU/MHD = substance use/mental health disorders; AOR = adjusted odds ratio.
Table 4 presents regressions predicting depression and binge drinking from caregiver characteristics among caregivers of persons with SU/MHD. Similar to findings for poor mental health (Table 3), caregivers of a spouse, friend, or relative with SU/MHD were less likely to have depression than caregivers of a parent with SU/MHD. Caregivers who provided caregiving for a longer duration and for whom caregiving included household help were less likely to have depression. Consistent with results for poor mental health and depression, caregivers of a spouse, friend, relative, or child with SU/MHD were less likely to binge drink than caregivers of a parent with SU/MHD. In addition, caregivers who provided caregiving for a longer duration and for whom caregiving included household help were less likely to binge drink. Caregiving more hours each week was associated with a lower likelihood of binge drinking.
Discussion
This study found that caregivers of recipients with SU/MHD reported poorer health status than caregivers of recipients with medical, cognitive, developmental disability, or old age–related conditions. Poorer health status was reflected in caregivers’ general, physical, and mental health, including having depression diagnoses, and in binge drinking and activities limitations. Among caregivers of recipients with SU/MHD, caregiving for a parent was associated with poorer health status than caregiving for a child, spouse, relative, or friend. Caregivers of recipients with SU/MHD who provided caregiving for a longer duration and for whom caregiving included household help were less likely to have poor mental health or a depression diagnosis or to engage in binge drinking.
Caregiving group comparisons
Important to consider is why caregivers of people with SU/MHD were most likely to report poor health across several indicators. Among caregivers of recipients with SU/MHD, some stressors are more likely, and more likely to present as a crisis, than among caregivers of recipients with other conditions. Among caregivers of recipients with SU/MHD, difficulties included care recipients being arrested (33%) or homeless (20%) and fear of recipients’ self-harm (68%) or harm to others, including the caregiver (35%). 15 , 16 The lives of parental caregivers of young adults with substance use disorder were characterized by fear and anxiety about its negative consequences. 17 Caregivers provided their children with help with housing instability and money for bail and legal services and had an overwhelming fear of their child's death. 17 In addition to these fears, shame and stigma are associated with SU/MHD. 17 , 18 Adult children of parents with MHDs reported that stigmatization inhibited them from seeking support. 18
Possibly, among caregivers of persons with SU/MHD, who were more likely to be employed than caregivers of other recipients, poor health was exacerbated by managing both caregiving and job needs. In addition, compared to caregivers of other recipients, caregivers of recipients with SU/MHD were more likely to have provided care for 5 or more years, and the majority helped manage household tasks for the recipient. The negative health effects of accumulated and chronic stressors, in both family and job settings, are well documented 19 and help to explain the present study's finding that poor health was more common among the group of SU/MHD-related caregivers.
Caregivers of recipients with SU/MHD
Among caregivers of recipients with SU/MHD, caregiving for a parent was associated with poorer health status than caregiving for a child, spouse, relative, or friend. We consider 2 reasons for this finding. First, before taking on an adult caregiving role, caregivers of parents may have grown up in a household with SU/MHD, such that their childhood presented difficulties because of the parent. A study of adult caregivers of relatives with SUD found that growing up with parents with SUD involved insecurity, neglect, foster home placement, and violence. 20 Similarly, a study of adult children of parents with mental health disorders found that, as children, they took over responsibilities for the family (cooking, cleaning, caring for younger siblings and the parent) when the parent was incapable of caretaking. 18 Following a disrupted childhood for which the parent was responsible, the adult child may continue or begin the parental role as a caregiver for a long duration, which may be experienced as quite burdensome in adulthood. 21 , 22
A related reason that caregiving for a parent with SU/MHD has negative health correlates is that, while parents prioritize autonomy and self-sufficiency, adult children prioritize parents’ safety and convention 23 ; this difference in priorities may be particularly difficult in light of the lack of safety associated with SU/MHD. Among adult caregivers of parents, parents often kept information about their activities and well-being from their children to protect their autonomy, whereas adult children were vigilant about their parents’ well-being because they feared not providing adequate care. 23 Participants concerned about their parents’ substance use (drinking, pain medication) found talking about their concerns with parents frustrating, so took to hiding the alcohol or extra medications in secret from the parents. 23 Related to this tension between adult children and parents, adult children overestimate their parents’ problems, and parents underreport their own problems, which leads to undesirable exchanges between caregiving offspring and parents. 24 This gap in perspective may be widened when SU/MHDs are present. 25
Although it may seem counterintuitive that longer durations of caregiving and the provision of household help were associated with better health among caregivers of recipients with SU/MHD, this is consistent with findings that caregiving may impart benefits through feeling appreciated and having a sense of purpose. 26 In the case of caring for someone with SU/MHD, providing household help over time may give the caregiver routine opportunities to confirm that the recipient is not in potentially harmful situations and is still alive and maintaining or regaining the path to recovery. Confirming that the care recipient is safe and engaged in recovery may reduce fear or worry, positively affecting the caregiver's quality of life. Among caregivers of recipients with SU/MHD, devoting more hours each week to caregiving may be associated with a lower likelihood of binge drinking because caregivers have seen the destructiveness of substance use or feel like they need to be fit to respond to a crisis at any moment.
Limitations
One study limitation was that the BRFSS asked about caregiving for substance use and mental health conditions together, and so we could not examine separate groups of caregiving for these conditions. Also, the BRFSS was a cross-sectional survey such that we could not determine causal associations among demographic and caregiving characteristics and outcomes. Further, future investigations of associations of caregivers’ caregiving characteristics with caregiver outcomes should adjust for caregivers’ demographic characteristics, which was not possible in the present study due to statistical limitations. Finally, the BRFSS caregiving module was given in only a subset of US states, possibly limiting generalizability of findings. For SU/MHD in particular, variations by country and culture in sources and levels of stigma among caregivers, and how they affect care recipients, are in need of additional research. 27
Conclusions
The National Alliance for Caregiving 16 reported that 61% of caregivers had no education or training for their caregiving role for a loved one with SU/MHD. These caregivers wanted access to quality services for themselves, including education, peer support, and respite care. Assisting caregivers to better health is critical, because poorer caregiver health and functioning are associated with poorer outcomes for care recipients. 28 With improved resources such as mental health treatment, caregivers of recipients with SU/MHD could possibly experience less physical and emotional strain. 17 Such findings underscore the importance of developing improved institutional and structural support for caregivers. Support could include the 12-step program of Al-Anon, 29 family support groups offered by the National Alliance on Mental Illness, web-based interventions, 30 and programs for caregivers to improve stress management and coping skills. 13
Footnotes
Author contributions
CT: conceptualization, funding acquisition, methodology, project administration, supervision, writing original draft; MCL: data curation, formal analysis, software, writing review and editing; FR: conceptualization, methodology, writing review and editing; AP: conceptualization, visualization, writing review and editing; MC: conceptualization, funding acquisition, methodology, writing review and editing
Disclosure statement
No conflicts of interest are reported by any of the authors. The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or any of its academic affiliates.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.