
Abstract
Keywords
People who suffer from serious mental illness are at increased risk of increased morbidity and premature mortality from comorbid medical illness. Observations at the beginning of the twentieth century noted that physical morbidity and mortality were greater among psychiatric patients than in the general population. Other commentators have noted the lack of thorough medical evaluation and inadequate treatment of medical disorders among psychiatric patients.[1] Comorbid medical conditions are particularly prominent in patients suffering from schizophrenia. This is not surprising given the social isolation, problems with adequate housing and the lack of organization of proper meals and poor diet reported for this group of patients.[2], [3] High rates of tobacco and other substance use in this group also add to the disease burden.[4] Apart from the obvious issues of significant disability related to the illness process itself, there appear to be a number of medical and health system barriers to recognition and management of medical illness in people with schizophrenia. Such barriers include a reluctance of non-psychiatrists to treat people with serious mental illness, frequent changes of treating doctor, lack of adequate follow-up due to patients’ itinerancy, and lack of motivation and available time and resources for a review of medical issues for people who may be uncooperative or have trouble communicating their physical needs.[5] Higher rates of poverty in those experiencing severe mental illness,[6] along with the experience of stigma,[7] may be further barriers that patients with mental illness have in developing an effective relationship with a general practitioner (GP). The atypical antipsychotics may also lead to an increased prevalence of endocrine disorders such as type 2 diabetes,[8] thus necessitating increased medical vigilance in this regard.
As a way of attempting to improve the co-ordination of the care of medical illness in patients with serious mental illness, there has been a move to develop shared care models between psychiatric specialists and GPs. Such models include a consultation-liaison model,[9] collaborative case discussions between specialist psychiatrists and groups of GPs,[10] shared care projects with extensive education for involved GPs,[11] case conferencing and consensus guidelines such as the current RANZCP guideline for schizophrenia.[12] There have also been substantive improvements in remuneration for shared care in Australia with the Medicare Plus program encouraging a collaborative care mode.
Top End Mental Health Services (TEMHS) has responsibility for the provision of mental health care to the population of the Top End (the northern two-thirds of the Northern Territory). Darwin is the major population centre for the Top End and has a population of around 100 000. The remaining population of the Top End, approximately 60 000, are located in the regional towns of Katherine and Gove and in rural communities. The Top End Division of General Practice provides education and support for GPs in Darwin as well as for GPs and Aboriginal health workers who work in regional and rural locations.
There is a shortage of GPs in Darwin, with 2333 people per GP compared to 1419 per GP nationally.[13] This has led to a significant reduction in bulk billing available for medical management of patients case-managed by TEMHS. This led to a funding arrangement between the service and the Top End Division of General Practice to establish a GPs’ clinic at the main outpatient facility of the service in Darwin. As a result of this agreement, the Division organized for GPs with a special interest in mental illness and population health to attend the outpatient facility one morning a week. Appointments for the GP are made through the reception for the outpatient facility and in co-ordination with the patient's case manager. Medical records of the General Practice are kept separately from the patient's mental health file but may be shared between the GP and case manager/treating psychiatrist with the patient's consent.
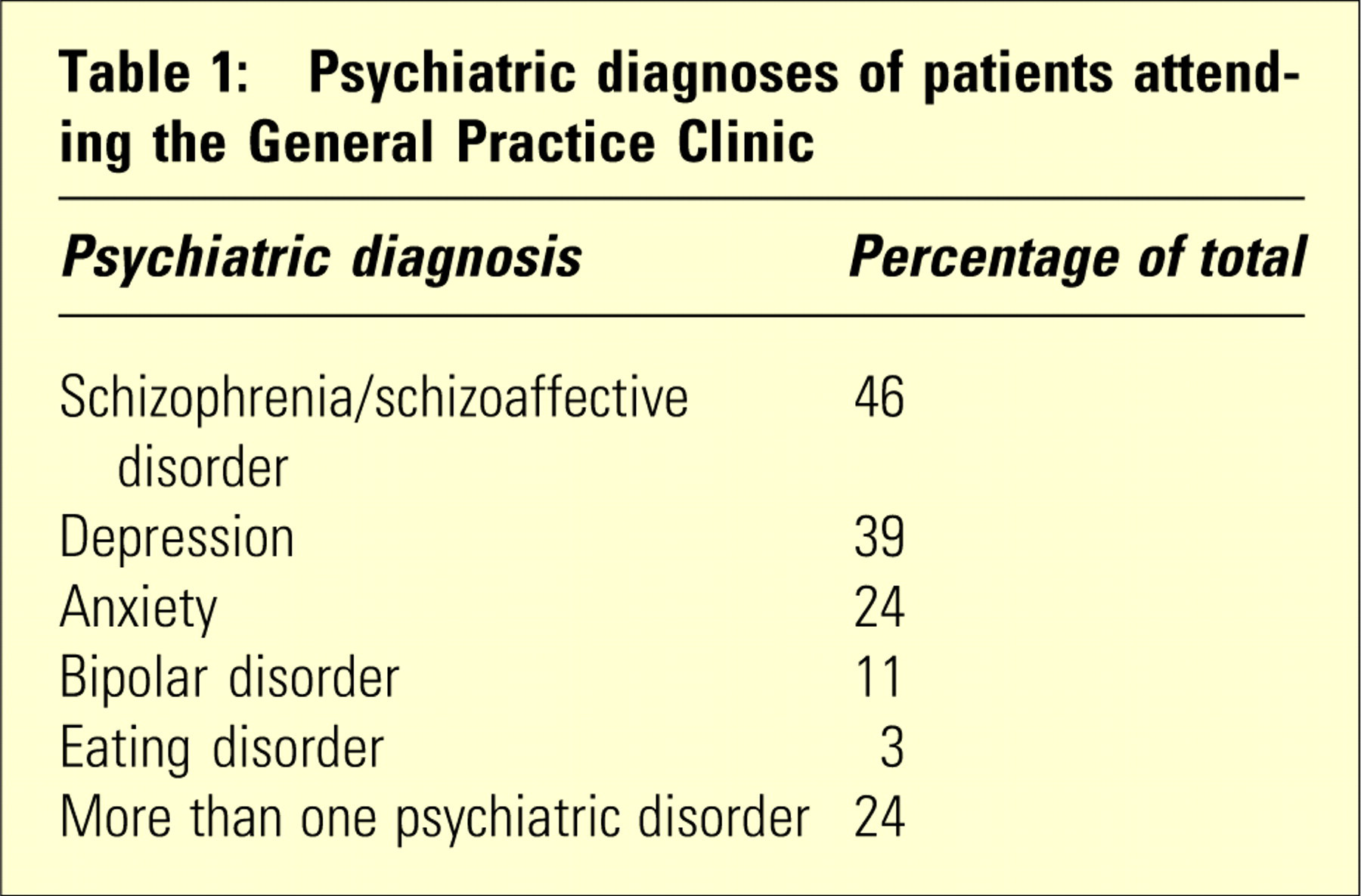
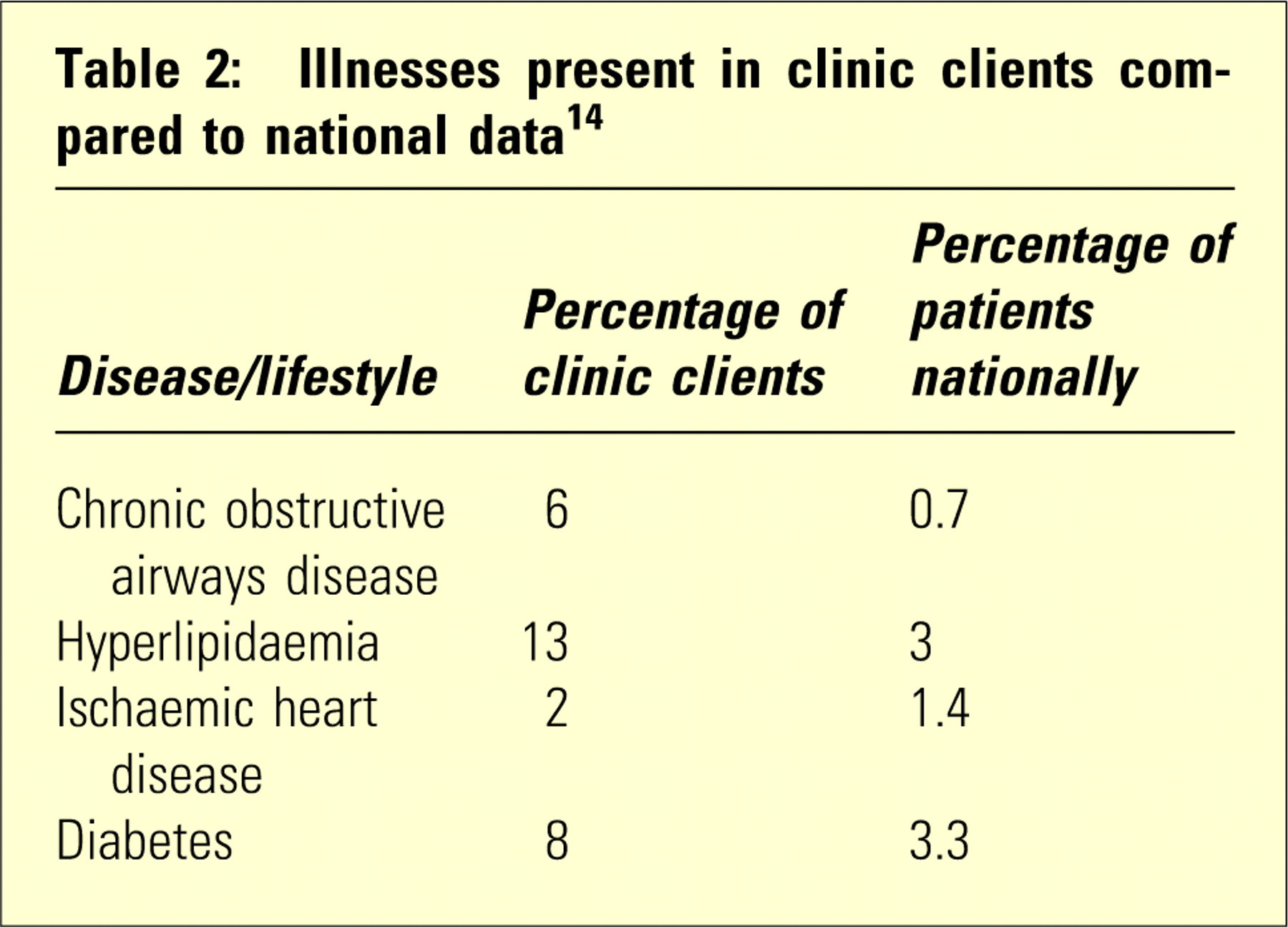
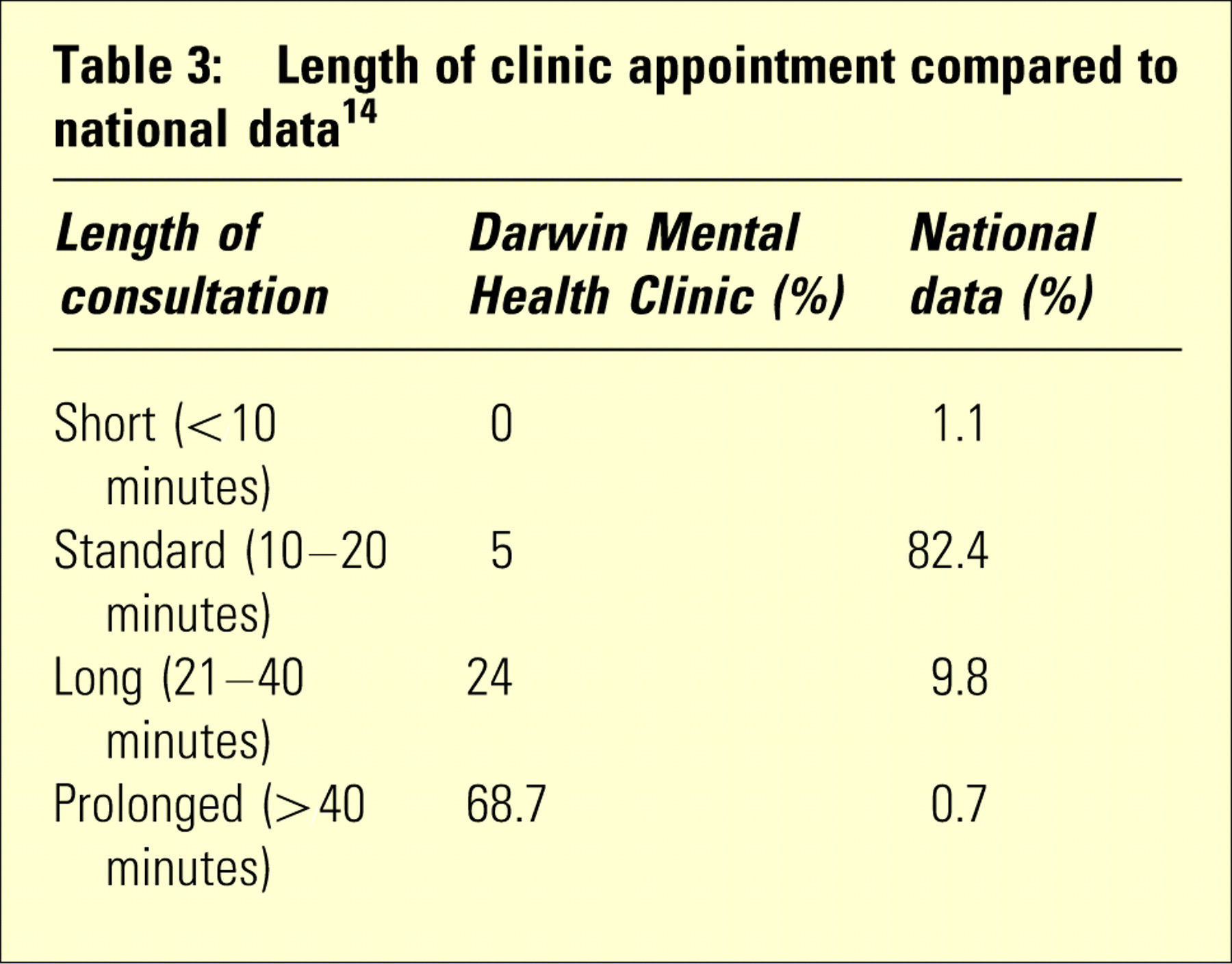
Between April 2004 and December 2005, the clinic was well patronized by patients; there were 86 clinical sessions and 160 patients attending in 470 clinical encounters. A significant proportion of the patients experienced serious mental illness (Table 1). The client group also appear to experience a significant burden of physical illnesses compared to the general population (Table 2). There was an average clinic attendance of 5.5 patients per week with a significant proportion of these appointments being of standard duration or more, longer than national data (Table 3). However, there continues to be a number of patients who do not attend. This is offset by the outpatient facility reception staff double booking through prior knowledge of the patient's reliability with appointments and also accepting ‘walk ins’ and urgent referrals from case managers/psychiatrists on the day. This provides access for patients with acute medical problems and makes optimum use of GP time. This is in stark contrast to non-attendance for a booked long appointment time in private general practice, with receptionist frustration and loss of income.
Psychiatric diagnoses of patients attending the General Practice Clinic
Illnesses present in clinic clients compared to national data[14]
Length of clinic appointment compared to national data[14]
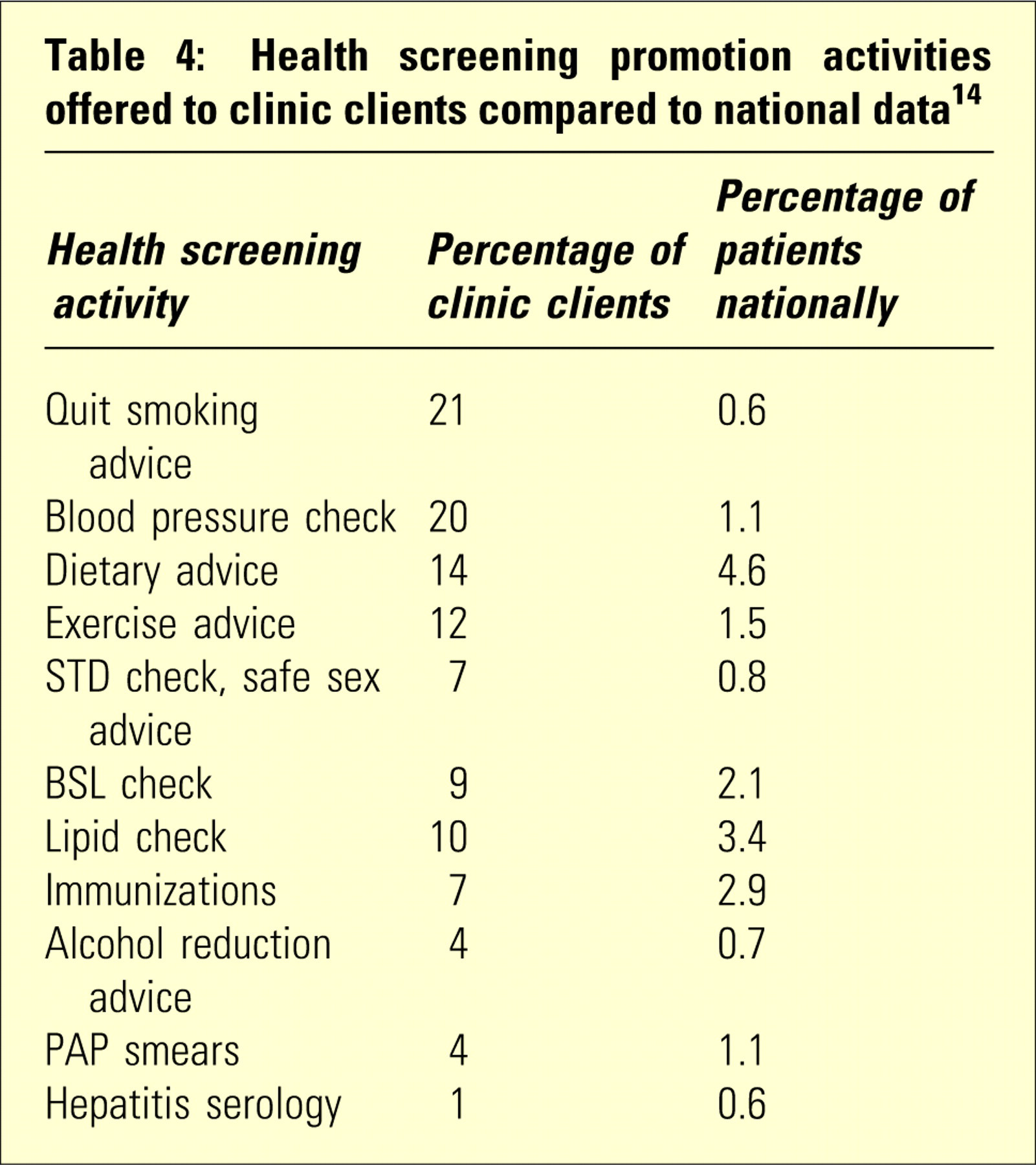
Co-ordination of patient care with TEMHS staff is high. The GPs in the clinic are having case conferences regarding patients 60 times more often than GPs nationally,[14] and instituting care plans and team care arrangements over 50 times more often.[14] The team care arrangements include the provision of physiotherapy, and dental and dietician care to the patients attending the clinic. The GP clinic has also worked collaboratively with Northern Territory Association of Relatives and Friends of the Mentally Ill (ARAFMI) in the recruitment of the clinic's patient group into the ARAFMI healthy living program. Given the increased time allowed for consultations in the clinic, the GPs have been able to perform a significant amount of health promotion activity (Table 4). Smoking advice and screening for hepatitis appear to be particularly relevant for the clinic clients. Sixty-eight percent of the clinic clients smoked (compared to 18% of the Australian population) and there were high rates of hepatitis C, 8% of clinic clients being hepatitis C antibody positive compared to 0.1% of the general Darwin population. Patients with hepatitis C with chronic active hepatitis are offered free hepatitis A and B vaccinations. The patients are also given advice on liver harm minimization.
Health screening promotion activities offered to clinic clients compared to national data[14]
Some patients with depression, anxiety and comorbid chronic pain syndromes were referred on to psychologists for cognitive behaviour therapy through the Better Outcomes in Mental Health Initiatives. This was a significant supplement to the psychological services offered by TEMHS.
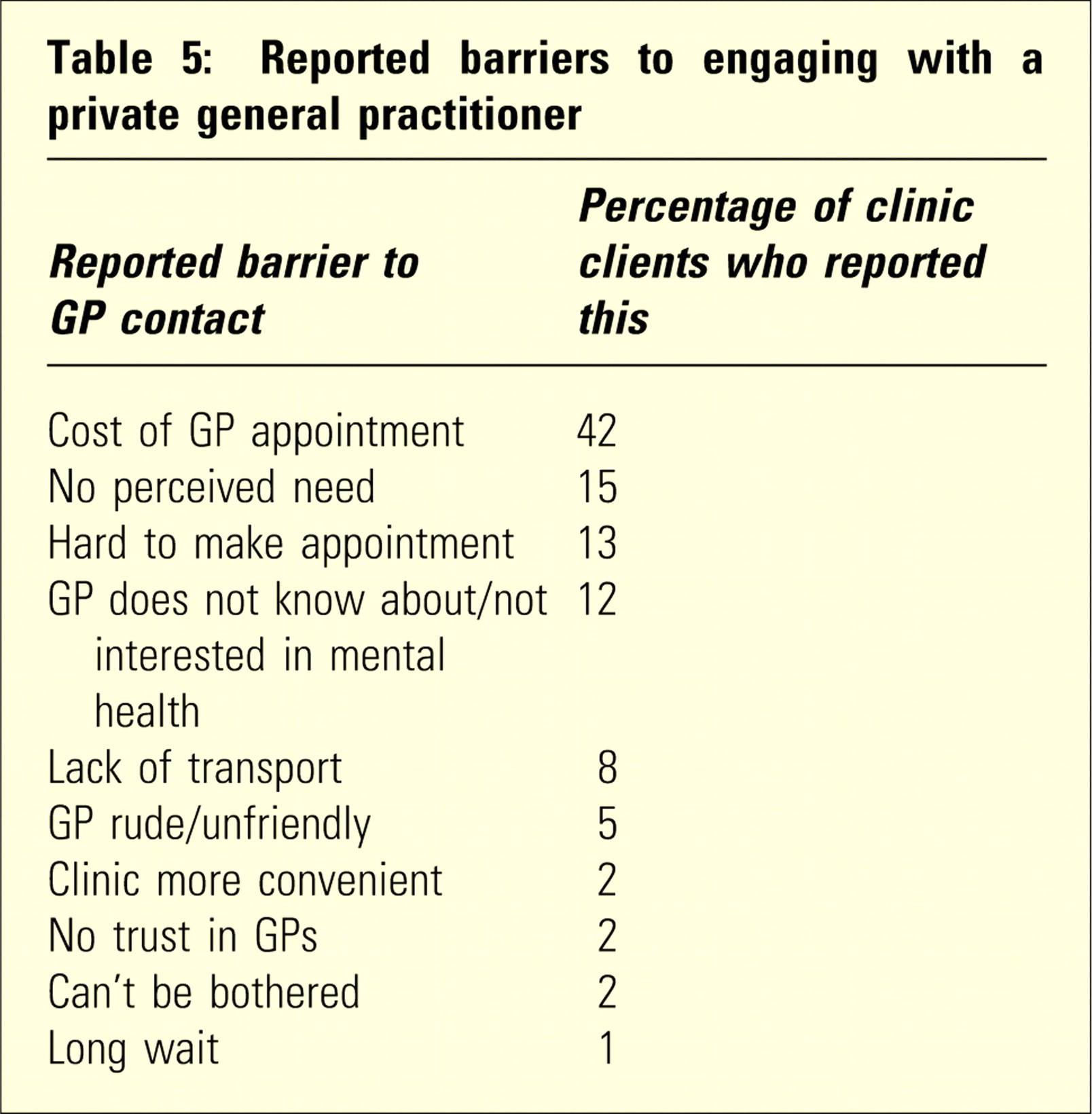
The General Practice Clinic appears to be popular with the patients and seems to have overcome a number of reported barriers to this group seeing a GP (Table 5). However, a significant barrier to linking patients with GPs in the community remains due to the cost of GP appointments. This was a factor for 42% of current clinic clients in comparison to only 16% of a client group surveyed in 2001 during a pilot program to establish the General Practice Clinic's viability. In 2001, 37% of the group surveyed had a preferred GP, compared to 24% in the current group.
Reported barriers to engaging with a private general practitioner
The above liaison between a mental health service and a division of general practice appears to be an innovative and unique program to improve the physical health of patients with serious mental illness in Darwin. The program seems to have been important in overcoming a number of barriers to effective engagement with a GP in this significantly disadvantaged client group, given the increasing cost of visiting GPs and insufficient time to address often complex medical needs and health promotion that is frequently required. Good care by a GP is considered to be an essential component of the cost-effective treatment of people concurrently suffering from severe mental illness.[15] The model discussed above may be an effective way of ensuring such quality care in a framework of limited organizational cost and may help bring about considerable individual health benefit.