
Abstract
Patient satisfaction derives from the patient's evaluation of how well their personal, emotional and physical needs are met by an organization, thus providing a valuable and valid outcome indicator of the quality of service provided. Informative, friendly and sensitive staff, feeling ‘listened to’ and understood by assessing clinicians, and being provided with adequate information are important factors that determine judgments about the quality of care received.[1] Patient perception of quality of care can potentially impact on treatment outcomes. Of note, effective provision of information from assessing clinicians has been linked to increased compliance with treatment recommendations.[2] Assessment of patient satisfaction provides integral information to help shape further service development. Thus, the aim of the current study was to evaluate patient perceptions of quality of the service at the Black Dog Institute Depression Clinic, satisfaction with the service and elements of the assessment process, and to gauge the likely implementation of treatment recommendations.
THE BLACK DOG INSTITUTE
Formed in 2002, the Black Dog Institute builds on clinical services and research undertaken at the Mood Disorders Unit (established in 1985), where outpatient assessments were offered to those with persistent and/or treatment-resistant mood disorders. The Black Dog Institute Depression Clinic has operated as a tertiary referral service since 2005, providing expert treatment advice to managing clinicians seeking a second opinion regarding diagnosis and management strategies. The Clinic adopts a diagnostic sub-typing model,[3] whereby clinical definition of separate mood disorders is posited as a key driver for more rational and specific treatments. Our structural model for depressive disorders[4] identifies three principal mood disorder sub-types: psychotic depression, melancholic depression and non-melancholic depression (the last proposed as a heterogeneous group in which personality style and life event interactions are of relevance). Structural and functional aspects of the three-class model have been explored in detail elsewhere.[5]
Patients attending the Clinic undergo three stages of assessment. The first involves completion of the computerized Mood Assessment Program (MAP), a data collection tool[3] that produces a summarized report detailing relevant patient information. These data are utilized by the consultant psychiatrist during the second stage of assessment, in which a full clinical history is gathered and later presented at a clinic consensus meeting. Consensus meetings serve to consolidate diagnostic information and formulate treatment recommendations, with input from the senior psychiatrist. Patients (often accompanied by relatives) attend this meeting to discuss diagnosis and management strategies, followed by a debriefing session. The MAP report is sent to the referring clinician, accompanied by a detailed letter outlining specific treatment recommendations. The third stage of assessment constitutes a follow-up appointment assessing treatment outcomes, 3 months following initial consultation.
METHOD
The sample consisted of 321 patients referred to the Depression Clinic during 2006–2007, who agreed to participate in research conducted by the Institute. Patients were informed that they would receive research questionnaires by post and be provided with the opportunity to evaluate Clinic services received.
Questionnaires were sent to all 321 patients, of whom 114 (35%) replied. The following aspects of the service were rated: (i) overall quality, (ii) satisfaction with the overall service, (iii) perceptions of the staff, including the assessment provided by the consultant and senior psychiatrist, (iv) satisfaction with the information provided, and (v) satisfaction with the treatment plan. Other questions explored whether patients would be likely to recommend the service to others, whether their expectations of the service had been met, and the likelihood of implementing management strategies recommended by the Black Dog Institute clinicians within the 3 months following assessment.
RESULTS
Four patients were excluded from the responding sample due to revoked consent for participation in research (n=3) or language difficulties (n=1). The responder sample comprised 110 participants, the remainder (‘non-responders’) comprising 207 participants.
Initial comparison analyses were conducted to determine any differences between responder and non-responder samples (Table 1) on age, sex and depressive sub-type (unipolar vs bipolar, melancholic vs non-melancholic). Also examined, were mean baseline depression severity scores as assessed by the patient-report DMI-10 measure,[6] and clinician-rated functional impairment scores (functioning assessed over the month prior to attending the clinic). Despite similarities between groups, responders were slightly older, with females over-represented, and presented with less severe depression as indicated by slightly lower mean scores on the DMI-10 measure.
Sample characteristics
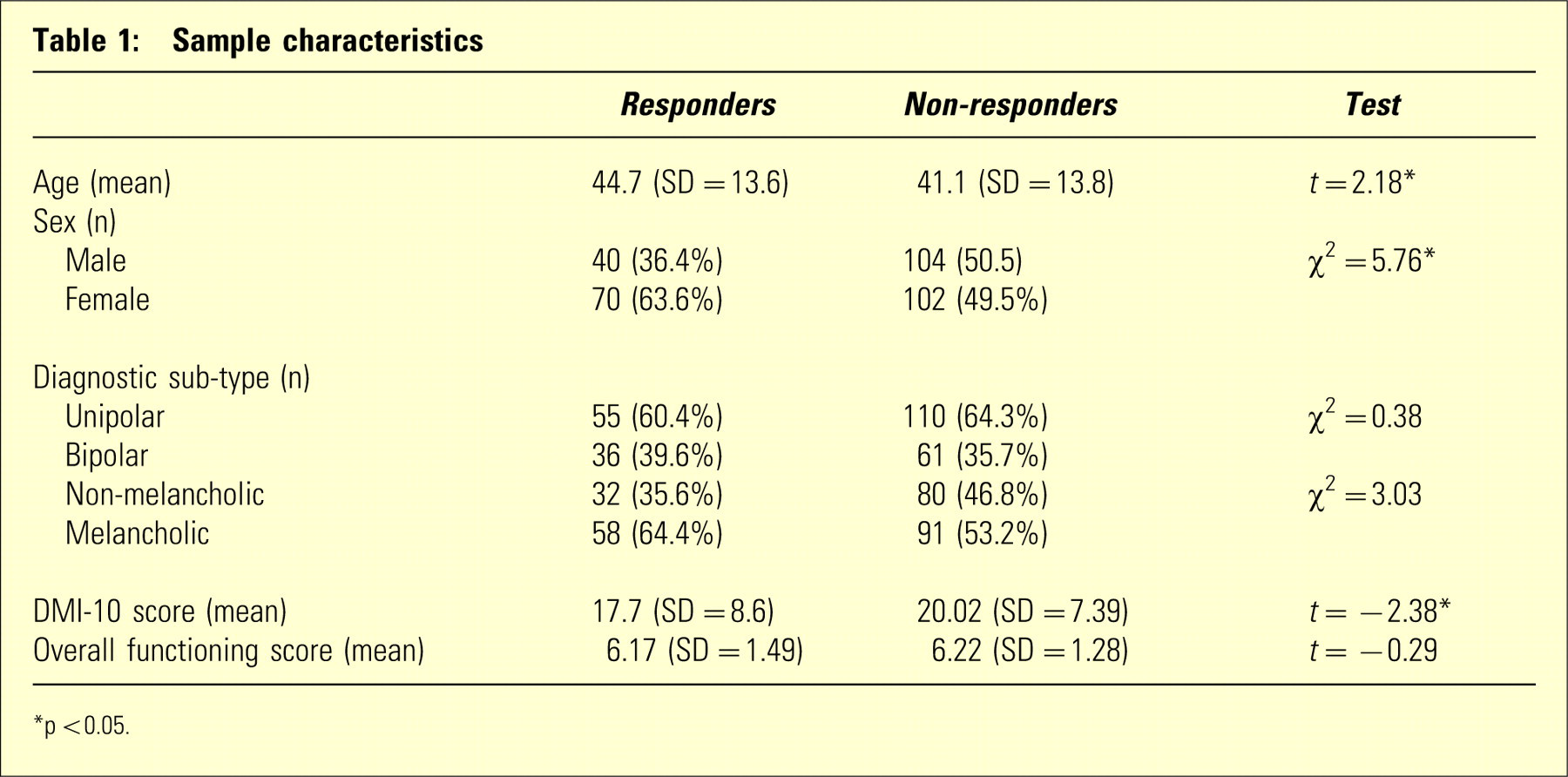
∗p <0.05.
Satisfaction with service components
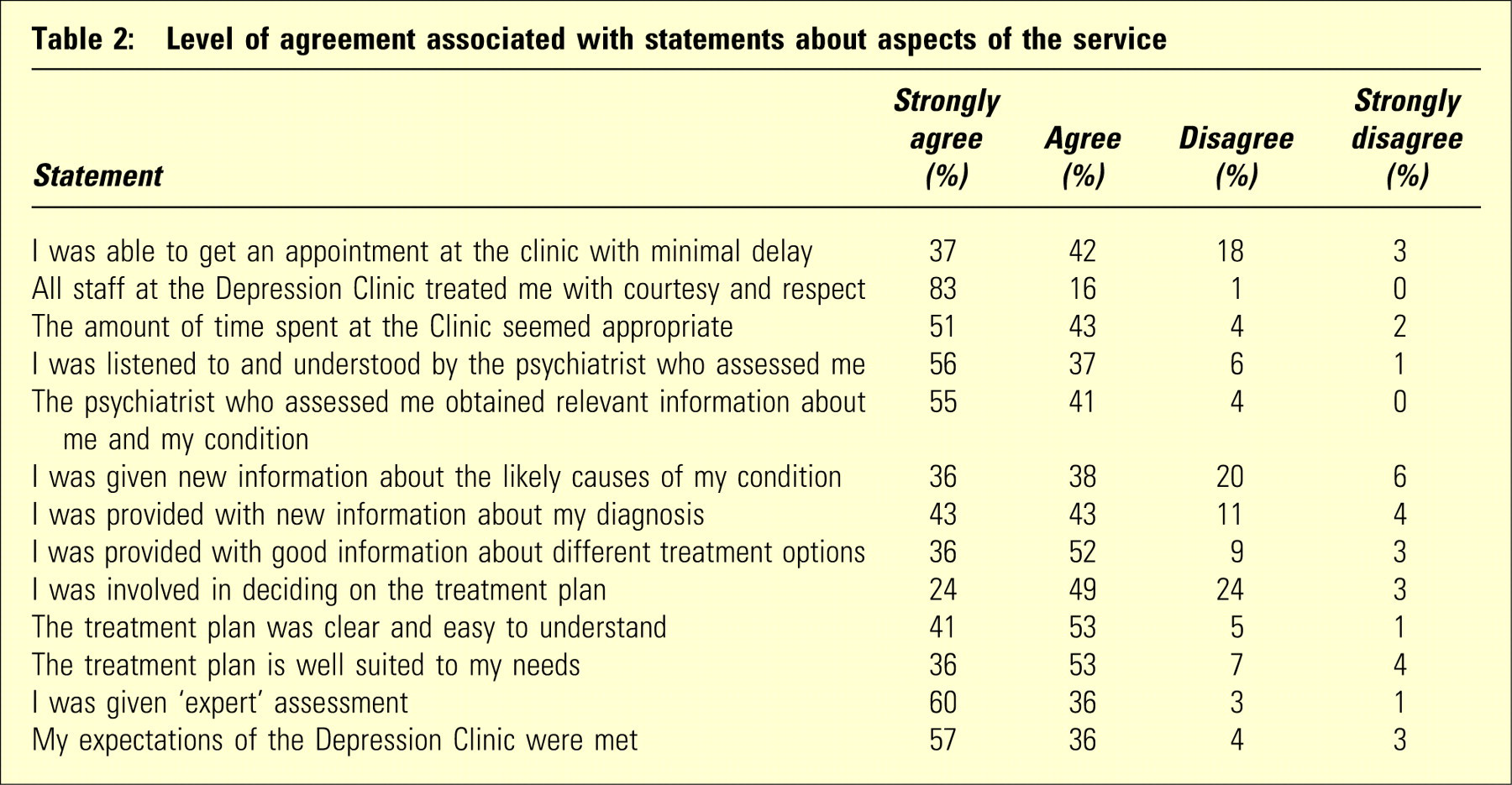
Overall, the majority of patients rated service components positively: 77% rated the ‘overall quality of service’ as ‘excellent’ and 20% as ‘good’. In terms of satisfaction with the overall service, 84% were either ‘extremely satisfied’ or ‘very satisfied’. Satisfaction with the assessment received from clinicians was also high, with 70% ‘extremely satisfied’ or ‘very satisfied’ with the consultant psychiatrist, and 72% for the senior psychiatrist. Table 2 outlines patient ratings of specific components of the service.
Level of agreement associated with statements about aspects of the service
A ‘priority’ index[1] was calculated (Table 3) to determine areas for improvement of service quality and overall satisfaction. This index was calculated by obtaining mean scores for each statement from Table 2 (converting responses on a 1–4 scale: strongly disagree, disagree, agree and strongly agree to scores out of 60; 1=0; 2=20, 3=40, 4=60 to increase the sensitivity of the score), aiding later interpretation and allowing examination of relationships between service aspect scores and patient satisfaction. Statements were ranked by score and assigned a ‘weight’. Those with the lowest scores attracted higher weights, indicating priority areas.
Priority index: statements about aspects of the service and overall satisfaction
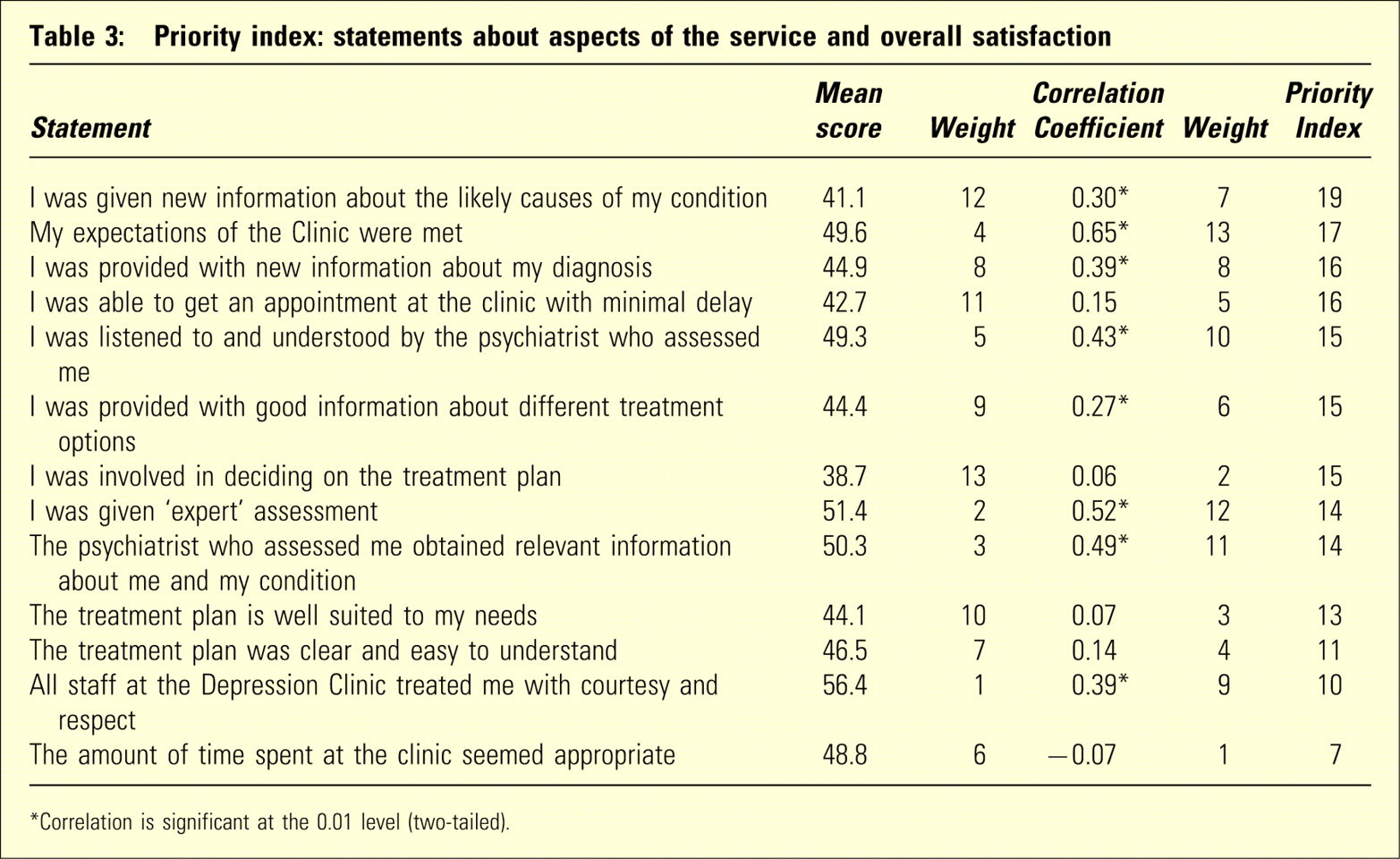
∗Correlation is significant at the 0.01 level (two-tailed).
Correlational analyses were next undertaken to assess the relationship between the ‘satisfaction with overall service’ item and the 13 statements in order to determine the most salient aspects of service. Statements were ranked by correlation coefficient, with highest weights assigned to statements that were most highly correlated with overall satisfaction. Both weights were then added to obtain the priority index. Higher priority index numbers represent issues that have the most impact on a patient's overall evaluation of a service, reflecting a combination of dissatisfaction and importance.[1] Attention to these issues is integral in increasing satisfaction. As shown in Table 3, priority issues tended to focus around the need for detailed information about causal factors, diagnosis and treatment options. Improved communication between patient and assessing psychiatrist, in addition to patient involvement in decisions around the treatment plan, were also rated highly. In terms of general service issues, delay in accessing clinic appointments was an important aspect requiring attention.
Other aspects of service
Other important factors reflecting patient satisfaction include the likelihood that the patient will recommend the service to others, and comparisons to previous experiences of healthcare facilities. Patient satisfaction was significantly correlated with the likelihood that they would recommend the clinic to others (r=0.59, p=0.01), with 82% of patients maintaining that they would ‘definitely’ recommend the service. Over 80% of patients rated their experience at the Depression Clinic as being ‘superior’ to previous experiences where a health professional provided mood disorder assessment.
In terms of treatment, the majority of patients (92%) were satisfied with recommendations suggested by the psychiatrist. Furthermore, 93% rated the take-home treatment recommendations list as being ‘useful’. Three-quarters of patients maintained that they would be ‘very likely’ to implement treatment recommendations within the following 3 months, indicating high acceptance of advice provided. In addition, 73% of patients believed that there would be ‘moderate’ or ‘significant’ improvement in mood over the subsequent 3 months as a direct result of implementing such recommendations.
Open-ended feedback
General comments about the Depression Clinic were obtained from 60 patients. The main themes included positive comments about clinic staff and professionalism of the service. Negative comments focused on the length of time spent with the psychiatrists (“I felt rushed with the psychiatrist, trying to answer questions in such a short space of time, especially when I have trouble concentrating …”), and not being provided with enough information concerning treatment recommendations (“The treatment options could have been explained more, plus side effects of medications recommended discussed in light of the varied medication I am on …”), again emphasizing the need for a psychoeducational component as part of the assessment process.
Suggestions for further improvement were obtained from 50 patients. Generally, patients noted the need for wait-list times to be minimized, and for more time to be made available with the psychiatrists. Other comments included the need for the Clinic to be more highly publicized and to provide information to patients about alternative managing clinicians (specifically, psychologists who have more detailed knowledge about depression and who are familiar with the Black Dog Institute model). A number of patients expressed the need for post-assessment support, particularly when given a new and unexpected diagnosis such as bipolar disorder (“I was diagnosed with Bipolar II disorder. I had no idea that's what I had. I felt quite distressed afterwards and would have liked someone to talk to …”).
DISCUSSION
In general, patients attending the Depression Clinic were very satisfied with the overall service provided and rated the service highly in terms of quality. However, a number of priority areas for improvement were identified. Provision of information about likely causal factors and diagnosis are aspects that require further attention. A psychoeducational component, built in to the assessment process, may be of use in terms of increasing patient understanding about their condition. Previous research[7], [8] indicates that provision of adequate information relates strongly to patient satisfaction. Furthermore, patients who are provided with information about prognostic and treatment options are more likely to adhere to treatment.[9] Provision of brochures or other educational resources, in addition to directing patients to the Black Dog Institute website are options that will be considered in light of the current findings.
A second issue for consideration is patient expectations of the service (Table 3). A realistic understanding of the limitations of care is necessary to ensure that expectations will be met.[1] In our case, patients are provided with an information sheet clearly outlining the limits of the service provided by the Clinic (specifically, that ongoing clinical management is the responsibility of the referring practitioner and that the service aims only to provide a ‘second opinion’ along with specific treatment guidelines and recommendations). Patient expectations (and indeed those of referring clinicians) of the service are expectedly high in light of the Depression Clinic being positioned as a specialist service with expertise in mood disorders. Patient hopes and expectations should be elicited prior to any assessments, prognoses or discussions of clinical management, allowing any misconceptions to be dealt with along with clarification of the limitations of service.[1] Furthermore, knowledge of patient expectations regarding their clinical experience enables healthcare facilities to modify technical, informational and organizational performance, thus increasing satisfaction levels.
A third issue to address is the nature of patient contact with the assessing psychiatrists. Patients' ‘explanatory model’ for an illness[10] constitutes their beliefs about diagnosis, causal factors, personal factors and possible outcomes. These ideas serve to frame the illness as more tangible, more treatable, and therefore less frightening, thus influencing clinical management and outcome.[1] Clear communication and explanation from the healthcare provider is therefore essential in shaping the already-established explanatory model held by the patient. Involving patients in discussions about diagnosis, treatment and prognosis are therefore important components for effective patient management. By engaging patients as informed and active collaborators in treatment, compliance with treatment recommendations can be increased. In order to achieve this aim, patient expectations, their explanatory model for illness and satisfaction with service must all be considered.
Study limitations
Non-responders were not re-contacted following the mail-out, perhaps resulting in over-inflated satisfaction ratings due to the possible bias of the responder sample. Indeed, patient satisfaction research suggests that those who are most satisfied are more likely to respond than those who are less satisfied.[11] Furthermore, a number of factors influence positive ratings, including social desirability bias, reluctance to express a negative opinion, and the structure and wording of the survey itself.[12] In order to address these issues and determine true generalizability of findings, active follow-up of non-responders is indicated. Nonetheless, our response rate (35%) is comparable to other research studies adopting single mail-out methodology,[1] and more specifically, comparable to a similar study examining satisfaction among patients with mood disorders where an initial response rate of 33% was reported.[7] A second mail-out or telephone call may have increased response rates slightly, yielding more representative responses. However, previous research suggests that two-wave mail-outs increase response rates by a negligible 3–4 percentage points.[1] In addition, given that treatment recommendations are generally implemented within a few weeks of assessment, our aim was to gauge satisfaction levels immediately following assessment, thus factoring out any changes in satisfaction that may be due to improved mood levels or other changes over time. Response rates in surveys assessing patient satisfaction with psychiatric services are generally low,[13] and in light of this, our sample cannot be presumed to be representative of all Clinic patients. Encouragingly, however, responder demographic and diagnostic profiles were similar to those of non-responder profiles, apart from differing depression severity levels, which may have influenced satisfaction ratings. Indeed, there is some evidence to suggest that non-responders are likely to have poorer health status and be less satisfied with medical care.[14]
Future directions
Although our results are positive and encouraging, the study highlights a number of areas that need to be addressed to ensure that the highest quality of service is provided; specifically:
providing detailed information to patients following assessment as part of a broader psychoeducational approach;
ensuring that patients receive adequate debriefing, whether undertaken by an in-house psychologist or the consultant psychiatrist, particularly for those who have received an unexpected or differing diagnosis (e.g. bipolar disorder);
formally assessing links between patient expectations, patient satisfaction and treatment outcome at 3 months.
To ensure adequate representation of patients attending the Depression Clinic, future satisfaction assessments will aim to target non-responder groups. Recruitment and data collection procedures have been suggested as important variables influencing response rates.[14] Thus, use of differing methodologies (face-to-face recruitment vs mail-outs) to boost response rates will be considered.
When patients are satisfied, clinical management and treatment outcome are enhanced. Thus, the Clinic aims to work to develop an orientation toward patient satisfaction. Results from the current study have initiated the appointment of an in-house clinical psychologist to address the impact of a new or unexpected diagnosis, and to provide psychological services with the aim of reducing the dissonance between clinic recommendations and actual therapy received by patients. In terms of patient expectations, strategies are in place to meet such expectations or explain why they cannot be met. Specifically, we will seek to undertake more detailed debriefing interviews with patients following assessment to gauge patient understanding and acceptance of treatment recommendations. To complement these strategies, we aim to extend on previous work[15] assessing treatment recommendation implementation and outcomes of patients attending the Clinic.
Footnotes
Acknowledgements
This study was supported by an NHMRC Program Grant (222708), an Infrastructure Grant from the NSW Department of Health, and by the Black Dog Institute.