
Abstract
Recruitment and retention of mental health specialists in rural Australia continues to be problematic. Isolation, lack of professional development and academic programs, and the lack of opportunity for peer consultation are some of the reasons identified in the National Rural Health Strategy.[1] The capacity to attract and retain medical specialists in rural Australia is an important concern for all regional centres, given that around 20% of the population is distributed across 95% of the land area.[2] The National Medical Labour Workforce Survey noted that of the 2954 psychiatrists and psychiatrists in training identified in a national survey, about 85% stated their main place of work to be a major city.[3] This unequal spread of psychiatrists in rural Australia translates into a ratio of 1:35 723 in non-metropolitan areas, compared to 1:8598 in urban areas.[4] At a recent national rural health conference, there was overwhelming agreement that the serious remote and rural health workforce difficulties will not be overcome merely by efforts to increase workforce supply.[5] Evidently, other initiatives are needed.
Specialists in rural and remote areas of Australia are disadvantaged when accessing continuing education and professional development, as their geographical isolation influences attendance at seminars, workshops and informal discussions with colleagues.[6] Lack of access to continuing professional education is believed to have a significant influence on recruitment and retention of healthcare professionals in rural areas.[7], [8] Advantages of synchronous exchanges, which happen in real time, include a more direct sense of collegial interaction, immediate resolution to questions and an effective contribution to team building.[9] Videoconferencing is one mode of synchronous exchange that has the potential to provide education and continuing professional development (CPD).[7], [10] The use of videoconferencing technology may be a suitable way to reach some of the more isolated communities with quality mental health information. Advantages of videoconferencing include greater convenience for people at remote sites, reduced travel expenses, and high levels of synchronous verbal interaction.[11] The value of an interactive videoconference is its ability to link a number of sites to a session at the one time, drawing together many people from remote areas as one group.
THE PROGRAM
The Rural Special Interest Group (RSIG) of the Royal Australian and New Zealand College of Psychiatrists (RANZCP) provided a program of educational meetings for psychiatrists and trainees in rural locations in an effort to decrease professional isolation and provide opportunities to obtain credit for CPD purposes. RANZCP members were surveyed prior to the program, for topic and speaker preferences, to identify and prioritize areas of training need. The national component was a series of six national videoconferenced seminars, designed to enable interactive participation between rural psychiatrists and specialists who were identified as prominent in the management of specific disorders in Australia. A second project targeted a perceived need for networking and peer review between isolated psychiatrists and a pilot peer review group by videoconference was also created separately for Western Australia. The Western Australian part of the project provided a series of six peer review group videoconferenced meetings of rural psychiatrists, for case presentations and discussion of supervision issues. Success in this project would demonstrate a way for the national body to obtain peer review opportunities. Fellows of the RANZCP are required to undertake a minimum of 50 hours of CPD activity per year. A form of peer review is a mandatory component. Linking the project through the RANZCP CPD program aimed to encourage rural psychiatrists’ attendance at the educational seminars. The West Australian group was registered with the RANZCP as a peer review group.
IMPLEMENTATION
National Program
To identify and prioritize Australian rural and remote psychiatrists’ areas of training need, psychiatrists registered as resident in rural and remote areas throughout Australia (n = 385) were contacted with a selection of topic areas available for education. Survey responses were compiled and topics selected based on those with the highest levels of endorsement. Leading specialists in each of the selected fields were approached to conduct the education sessions. Six seminars were conducted via videoconferencing with substantial time provided for interaction, enabling communication across all participating sites. Initially the program budgeted for an expected audience of 20 psychiatrists across 10 sites for each seminar. The demand for the first seminar exceeded expectation and 62 psychiatrists across 29 sites applied to attend. Additional funding to support the larger audience was obtained. To provide opportunities for rural and remote psychiatrists to obtain credit for CPD purposes in ongoing professional registration, the format of the education meetings fulfilled the RANZCP requirements for recognized CPD activities.
Western Australian Program
A West Australian peer review group, with six participants, was established to link physically distant rural psychiatrists. The group met on six occasions during the span of the project, providing further opportunities for networking. The group submitted the necessary paperwork to the CPD office of the RANZCP for official registration as required. The group aimed to develop a supportive framework with embedded professional values of courtesy and respect. The framework facilitated the frank exchange of knowledge, advice, constructive criticism and understanding. The format involved the presentation of difficult cases with subsequent discussion, and there was also discussion of ethical and service delivery problems. Every third meeting focused on supervision issues (regarding registrars in training). Meeting via multi-screen visual presentation to assist aspects of group relatedness was preferred.
PARTICIPATION
National Program
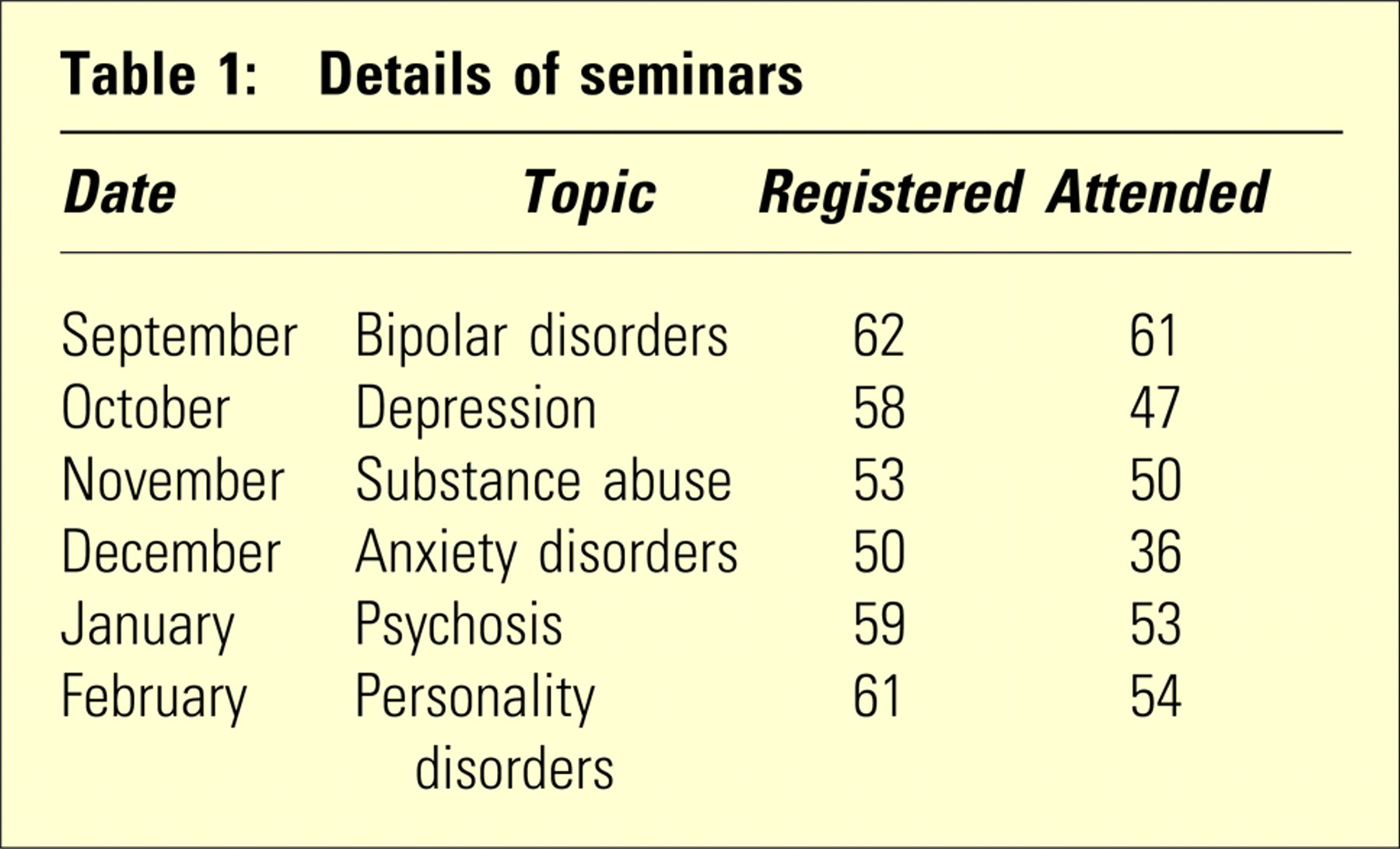
One hundred and six individuals participated in one or more of the seminars from June 2006 to June 2007, with 67% being consultant psychiatrists, 17% psychiatric registrars (trainees) and the remaining 16% allied health professionals. Figure 1 shows how participants were distributed across Australia. Further details about the seminars are presented in Table 1. Attendance at seminars was greater than recorded as additional, unregistered participants attended but were not counted via the pre-seminar individual registration process.
Distribution of participants in the National Program.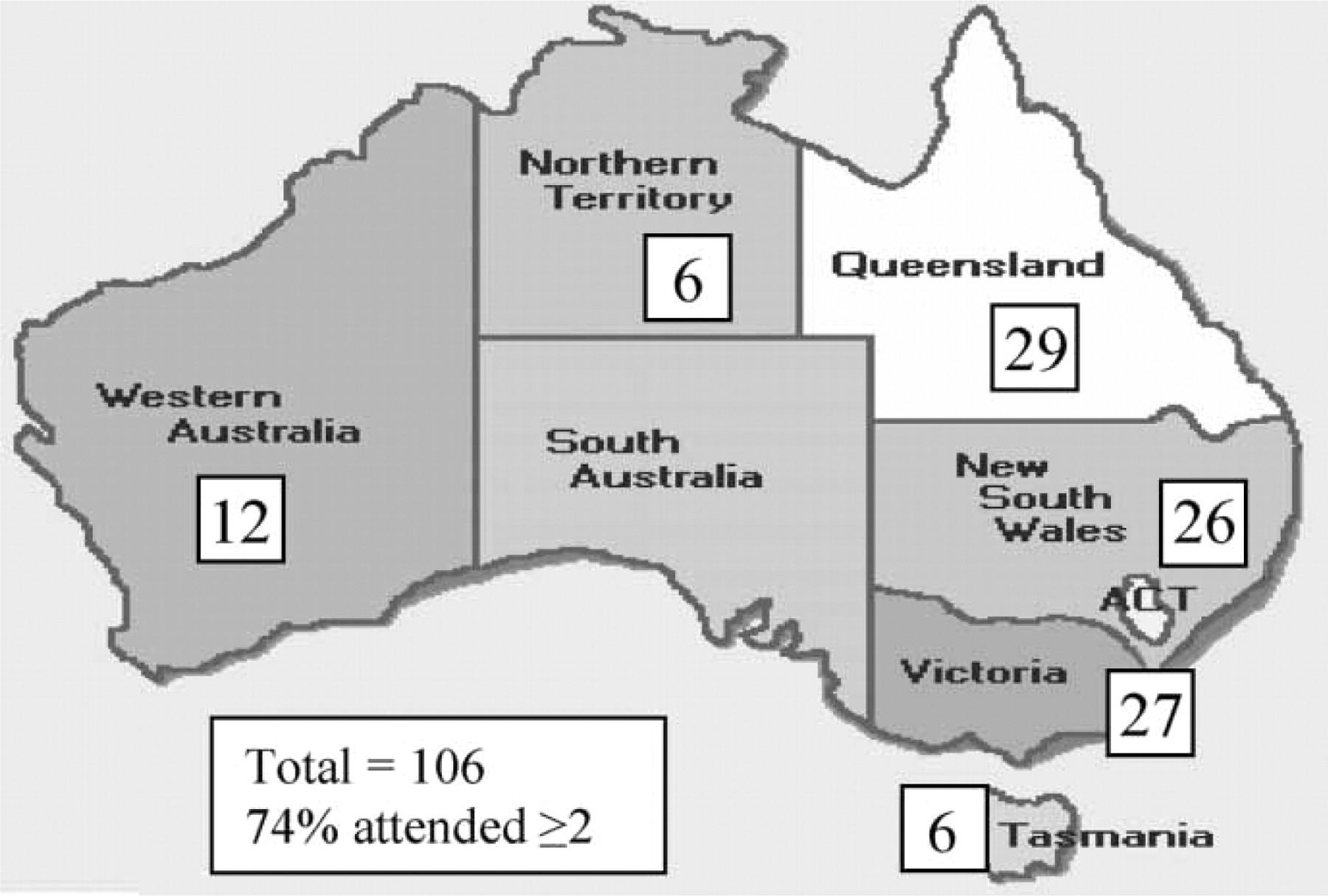
Details of seminars
EVALUATION
National Program
Evaluations were completed following each seminar and at the completion of the program. Both quantitative and qualitative data were collected via online surveys. Qualitative data were also obtained by telephone interviews with randomly selected psychiatrists from each State and Territory who fulfilled the participation criteria (two or more seminars). Evaluation demonstrated favourable views of the content and quality of the presentations throughout the program. Participants derived benefit from the clinical relevance of the seminars, backed by up to date research and coverage of practical issues. Seminars originated from both metropolitan and semi-rural areas, with no detectable difference in the experience of participants. This opened the possibility for future rural-origin educational programs with the potential of enhancement of rural practice. Qualitative results suggest that participants preferred to attend the seminars from remote sites than have to travel significant distances. The opportunity for academic and clinical skills building via videoconferencing was seen as invaluable in rural areas. The overwhelming majority (83%) of respondents found all six events beneficial. Most respondents agreed that the seminars contained the appropriate amount of information (75%), permitted interaction between presenter and audience (90%), and assisted their understanding of the topic (92%). Eighty-four percent of respondents agreed that participating in the seminars via videoconferencing reduced feelings of professional isolation via academic and collegial networking. In addition, the project appeared to foster a greater awareness of rural issues by city specialists. Thirty-two percent agreed that participating in the seminars improved networking opportunities, which, while not a specific project objective, was considered a useful adjunct. Eighty-eight percent of respondents agreed that the continuation of seminar provision to rural areas via videoconferencing should be an important priority for the RANZCP.
Western Australian Peer Review Program
Qualitative data were collected via phone interviews with the psychiatrists involved in the West Australian peer review group. Those interviewed reported that the group was a greatly beneficial initiative. The format appeared to work well and the process assisted networking between colleagues, who were addressing similar issues in comparable working situations. While it was suggested that four to five people seemed a good number for the group, it was proposed that it could work with as few as two or three. It appeared that the involvement of the metropolitan psychiatrist was a positive aspect. The metropolitan psychiatrist was well known to the rural members and often took their referrals. Peer review meetings provided a sense of connection between colleagues and assisted in the reduction of professional isolation.
FUTURE DIRECTIONS
Suggestions were presented by participants regarding potential future directions. It was suggested that educational information could be provided by a combination of metropolitan specialists, academics and rural practitioners covering systemic rural issues to foster and enhance sub-specialties and academic research outside metropolitan areas and assist recruitment to rural areas. It was mentioned that a useful extension could involve the inclusion of other specialties, trainees, medical officers and general practitioners as psychiatrists often work in teams in rural areas. Peer review groups that target geographically isolated psychiatrists were suggested, involving both topically based and geographically based groups. (This is now the subject of a current project funded br the SSRS for rural and remote psychiatrists provided by the Rural Special Interest Group of the RANZCP, and implemented by the authors.) Additional suggestions included the provision of workshops with written material; the recording of presentations to build a library to enhance training; a website for rural psychiatry which could be reviewed at psychiatrists’ convenience; greater availability using the internet and participation via ‘web-chat’, with psychiatrists able to converse about pertinent issues, and; onsite visits to rural units by specialists to explore the uniqueness of the rural situation. It was also mentioned that the growth of broadband internet across Australia may permit a low-cost framework and the potential for participation from home and office computers.
CONCLUSIONS
Attendance at seminars via videoconferencing provided rural psychiatrists with opportunities to obtain CPD time without the need to travel, providing a cost-effective alternative to accessing education. Involvement also enabled occasions to interact with their peers throughout Australia, generating networking opportunities. As access to seminars was not restricted to RANZCP Fellows, International Medical Graduates and trainees were provided with opportunities for further postgraduate education. The RSIG involvement meant that the education seminars were consumer-responsive, rather than centrally directed. It is recommended that the program continue as a means of reducing professional isolation in psychiatric practice. Videoconferencing is now a proven, effective and accessible training mode for the delivery of education to rural health practitioners. The technology enables live interaction and synchronous exchange and can also be utilized for case discussions, peer review, supervision and as a forum for meetings, involving both rural and metropolitan practitioners, as well as clinical activities.[7]
Footnotes
Acknowledgements
The authors acknowledge the support of the Commonwealth Department of Health and Ageing through the Support Scheme for Rural Specialists, the speakers, the RANZCP SSRS Steering Committee, the Rural Special Interest Group of the RANZCP and participants.