
Abstract
Psychological investigations have found mental disorder to be present in greater than 90% of people who suicide[1], [2] and those with suicidal ideation.[3] However, there is a credible body of work indicating that normal human distress is being wrongly classified as a mental disorder.4–9 In 1801, Philip Pinel stated that “the ordinary powerful motives” driving suicide (independent of mental disorder) included “loss of honour and fortune”.[10]
The emotions motivate behaviour and can be divided into two broad categories: the positive/pleasant emotions (e.g. joy and excitement)[11] and the negative/unpleasant emotions (e.g. shame, guilt, grief and anger).[12] Physiological[13] and various neuroimaging studies[14], [15] have revealed that these categories have distinct neurologic features.
Shame and guilt (the ‘moral emotions’[16]) are closely related. Shame is experienced when we evaluate our actions and conclude that we have done wrong. It encompasses the whole of ourselves, we conclude that we are unworthy and prefer to hide or die. In contrast, guilt is experienced when we focus on our behaviour, and conclude that our behaviour has breached standards.[17] Guilt may be remedied by confession or penance.[18] In both, there is the anticipation of adverse reactions from others. While many see these as separate, Nathanson described shame as being at the heart of guilt.[19]
Grief is the unpleasant experience of loss. The term is usually applied when another person has been lost, but it is also reported with unfulfilled wishes[20] and loss of status. Anger needs little introduction, arising from conflict and injustice. It is also a response to rejection[21] and ostracism.[22]
The negative emotions, as distinct from mental disorders, have received relatively little attention as precipitants of suicide. The role of shame in suicide from the psychodynamic perspective has been described.23–25 Studies of suicide notes have indicated the desire to avoid anticipated rejection. A recent study of 42 notes[26] found the commonest theme to be ‘apology/shame’ in 74% cases.[27] A review of classical mythology[28], [29] examined accounts of 36 suicides and found shame, guilt and grief to be the most common psychological features. Clinical experience indicates that grief and anger are common symptoms of those who survive serious suicidal behaviour.
Lester wrote convincingly on the role of shame in suicide, touching on employment status, gender and culture.[30] He gave details from the public record regarding the recent suicides of Captain Ernie Blanchard and Admiral Mike Boorda.
We take as a given that actual or threatened reputation damage causes negative emotions. We explored the public record with a view to extending awareness and knowledge of the role of reputation damage in suicide.
Method
We examined the public record over the last 20 years. We have collected records of suicides that have appeared as newspaper, radio or television statements over this period of time. From these, we selected potential cases and collected any additional information available from the lay press and the web. We sought accounts of individuals with no known history of mental disorder who suffered actual or threatened reputation damage and suicided shortly thereafter. We excluded all cases in which there was a history of psychiatric disorder, including any mention of ‘depression’. We selected cases that were initially reported in leading (as opposed to local) newspapers. This increased the likelihood of readers of this paper having some familiarity with one or more of the cases.
RESULTS
RESULTS AND SUMMARY
From the public record of the last two decades, details were located of 15 people who appeared to have no psychiatric disorder who had suicided following actual or threatened reputation damage (Table 1). All were male, the average age was 55 years (range 40–76 years).
Details of 15 people who suicided following actual or threatened reputation damage.
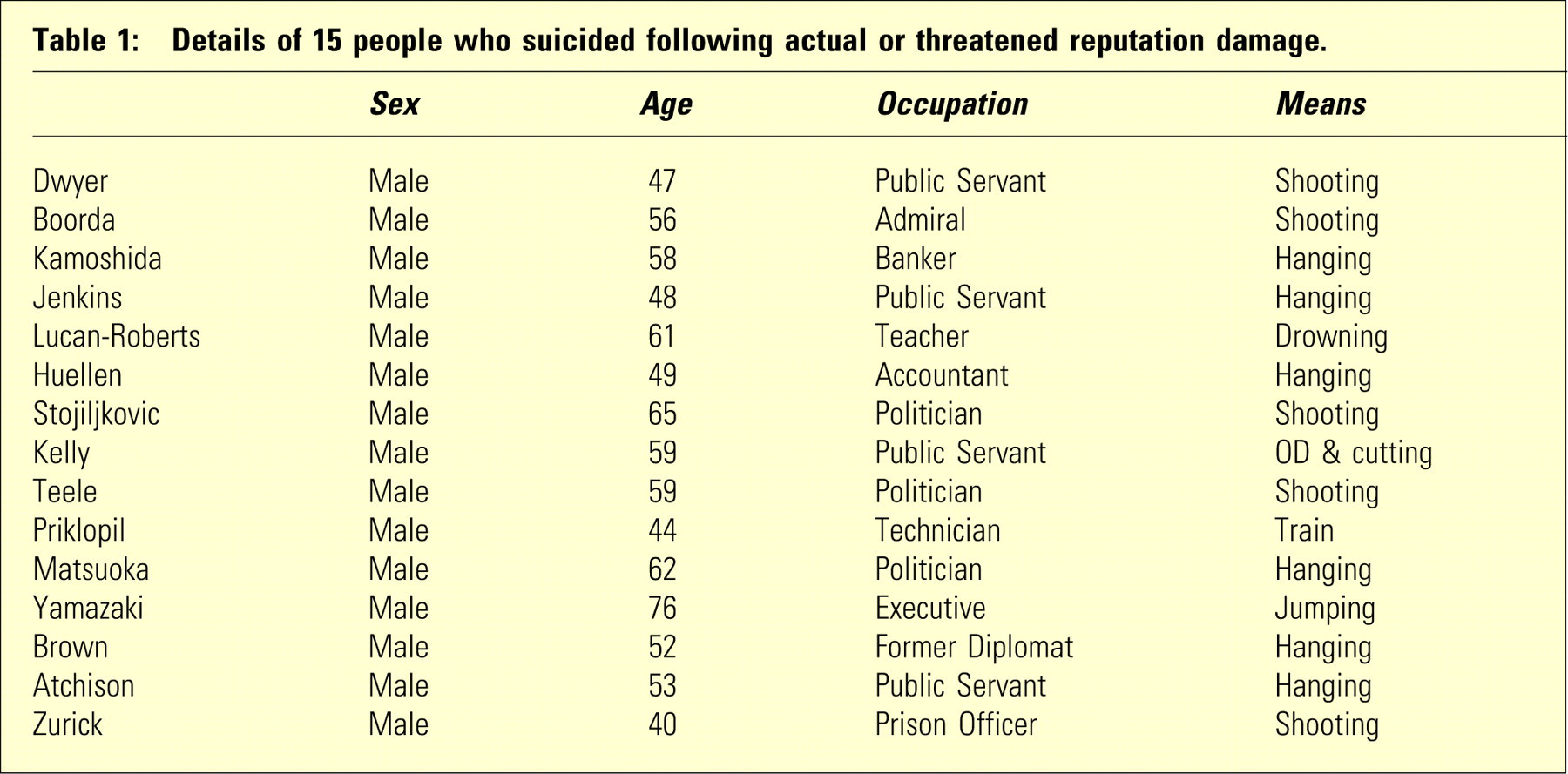
Less comprehensive details are available for 18 additional people who died in association with the Wood Royal Commission and Operation Auxin. Where gender was known (n = 12), all were male. Where occupations were known (n = 8), three were police officers; others were a prison officer, a plumber, an electrician, a former alderman and a retired judge. Where means were known (n = 4), two died by car exhaust, one by jumping and one by shooting.
Thus, there is evidence indicating that actual or threatened reputation damage may lead to suicide in middle-aged males.
DISCUSSION
We looked for individuals who had suicided following actual or threatened reputation damage. We make no claim regarding the degree to which actual or threatened reputation damage increases risk of suicide. Nevertheless, the presented data suggest that actual or threatened reputation damage may be accompanied by increased suicide risk.
We used the public record. Criticism can be made of this source of data, in that it lacks the precision of the psychological autopsy and evidence of mental disorder may be overlooked. The contrary view is that journalists are trained to report the facts and are quick to highlight any suggestion of ‘mental disorder’ (along with a perceived public duty to reveal any evidence of professional negligence). Supporting the use of lay data is evidence which suggests recent undue medicalization of human distress and behaviour.4–9, [36]
We excluded all cases where reports indicated a past or present mental disorder, including those with any mention of ‘depression’. In general, these were successful people, making a past history of severe mental disorder unlikely.
We agree that the public record provides insufficient details to categorically state that the selected individuals were totally free of mental disorder. However, the reporting journalists, who look for such things, and talk to family and any involved professionals, found no such evidence.
We excluded mental disorder (as best we could) as this would have complicated matters. We found evidence indicating that reputation damage increases the risk of suicide. This is consistent with the view of Pinel[10] who observed that, in the absence of mental disorder, suicide may follow “loss of honour and fortune”.
Suicidal intent in the absence of mental disorder raises clinical and legal difficulties. We have dealt with such cases on our ward, when high profile local identities have been investigated by police for serious matters. Mental Health Acts provide legitimate authority to retain people who are a danger to themselves in a safe environment, but these instruments require the presence of a mental disorder. As Horwitz and Wakefield[9] demonstrate, non-disordered normal loss responses are usually characterized by ‘symptoms’ which are the same as those of ‘major depressive disorder’ and, when taken out of context, this normal response may be diagnosed as disordered. Thus, to keep people safe, a mental disorder can be claimed. The appropriateness of this course of action is highly doubtful, but in this era of litigation and blame, clinicians may have the need to protect themselves as well as their patients.
The individuals reported here, and their circumstances, are not representative of the man in the street. There are many factors which determine whether a suicide will be reported on the public record, including public prominence (such as ‘Lord’ Such) or dramatic means, such as a bullet to the head in a public place (as in the cases of Dwyer, Stojiljkovic and Teele). However, ‘local’ public records (e.g. local newspapers) frequently carry reports of less prominent people taking their lives using unspectacular means, as a consequence of reputation damage. Highly ‘newsworthy’ examples are given in this article in the hope that readers may have some familiarity with one or more cases.
It has been argued that the three Japanese deaths do not belong in this sample, as they are of a different culture, one in which there is a long history of reputation damage (‘loss of face’) leading to ritualized suicide (harakiri). However, there has only been one performance of harakiri reported in the last half century (Yukio Mishima, in 1970), and in current Japanese culture, suicide, particularly ritualized suicide, is strongly discouraged.[37] If preferred, these three deaths could be withdrawn, but this would not alter our main thrust. Minor changes would be the lowering of the upper end of the age range from 76 to 65 years, and the lowering of the average age from 55 to 53 years. The finding that reputation damage may lead to suicide is not negated by belonging to a culture which has condoned, or condones, such practice.
We take as a given that actual or threatened reputation damage causes the negative emotions of shame, guilt, grief and anger. We have presented evidence suggesting that reputation damage may increase the risk of suicide in the absence of mental disorder. Some of the listed people were facing custodial sentences. It could be argued, therefore, that in these cases, suicide was the result of the negative emotions triggered by the prospect of penalty rather than reputation damage. We would not dispute this interpretation. However, it is probable that the prospect of penalty compounded rather than replaced the pain of reputation damage.
These data have relevance to what has become known as the ‘name and shame’ punishment. It is impossible to quantify the impact being publicly ‘named’ will have on an individual, and it is likely to differ from one individual to another. This paper suggests that loss of reputation increases the risk of suicide. Thus, ‘naming and shaming’ needs to be conducted with great caution.