
Abstract
Clozapine is an atypical antipsychotic drug licensed for the treatment of resistant schizophrenia.[1] It has been shown to have superior efficacy in schizophrenia compared to other antipsychotics.2–6 Clozapine was funded in New Zealand on the Pharmaceutical Schedule in February 1999 (L Wellington, pers. comm., 2006). Prior to this date, funding had to be obtained from the budgets of individual hospitals.
Clozapine is associated with a relatively high risk of agranulocytosis (0.7%), with 80% of cases occurring within the first 18 weeks of treatment.[7] In New Zealand, clozapine can only be prescribed by a psychiatrist or by a psychiatric registrar, with strict monitoring protocols. The patient must be registered with the Clozaril Carelink™ program and submit to full blood counts weekly for 18 weeks and 4 weekly thereafter.[1]
Patients are initiated on low doses because of early hypotension and sedation. There is an increased risk of seizures with higher doses.[8] The target daily dose of clozapine in the treatment of schizophrenia ranges from 250 mg (female, non-smoker) to 550 mg (male, smoker).[7] Clozapine is metabolized mainly by the enzyme cytochrome p450 1A2 in the liver. Higher doses of clozapine are required in cigarette smokers because of an induction of cytochrome p450 1A2.[9] For the unlicensed treatment of psychosis induced by treatment of Parkinson's disease, the dose range is 6.25 mg to 250 mg per day.[10]
Drug concentration monitoring of clozapine is widely used but the therapeutic range is not well established. Monitoring is said to be useful for observing the effect of drug interactions, to assess compliance, and to assist in the management in drug overdose.[11]
The fact that it is a requirement that all patients on clozapine are documented in a database (Clozaril Carelink™, Dataware, Auckland, New Zealand) enables our entire local population of patients and their psychiatrists to be examined in terms of prescribing and monitoring practice.
Objectives
Within our local population of clozapine patients, our objectives were to describe the daily dose, age of the patients, length of current treatment and the use of clozapine plasma concentration monitoring; to detect any significant associations between clozapine plasma concentrations and daily dose, age or gender of the patients; and to survey the psychiatrists to ascertain their views on the indications for which they were prepared to prescribe clozapine, and of the utility of clozapine plasma concentration monitoring.
Method
Patients who were dispensed clozapine during December 2005 in Christchurch, New Zealand (a city of 374 800 people), were eligible for entry into this study. Over 90% of these patients (n = 353) received the drug from a single pharmacy (Hillmorton Hospital), and these patients were included in this study. All patients outside of hospital were followed up by their psychiatrist and a psychiatric district nurse. The remainder, who live in supported accommodation run by a community-based mental health trust, received clozapine from a community pharmacy within Christchurch. These patients were excluded from this audit because it was not possible to retrieve all relevant data.
Patients in the first 18 weeks of treatment were excluded as they may not have been on a stable maintenance dose. The daily dose was recorded for those patients that had been dispensed clozapine during December 2005 from the hospital pharmacy computer system (Windose™, IBA Health, Wellington, New Zealand). Data on the gender, age and the length of treatment of these patients were gathered from the Clozapine Carelink™ database.
The history of clozapine plasma concentration monitoring was collected for each patient from the Canterbury Health Laboratories pathology system (Eclair™, Sysmex New Zealand Limited, Auckland, New Zealand). Since all clozapine plasma concentrations in the Canterbury region are analysed by Canterbury Health Laboratories, these data were considered to be a complete record for these patients. Clozapine plasma concentrations, in those who had these measured during 2005, were matched with daily dose data from the pharmacy dispensing system (Windose™), and analysed for any association between clozapine plasma concentration, daily dose and age data from Clozaril Carelink™. Patients were excluded from analysis if: (i) they were not on the same daily dose in the preceding or following month, to ensure they were on a stable dose; (ii) the clozapine plasma concentrations were performed during an admission at Christchurch Hospital, thus excluding patients who may have overdosed; (iii) the clozapine plasma concentration was zero, thus excluding patients who were not taking their clozapine. Only one set of results was included per patient.
Consultant psychiatrists who cared for these patients were asked to complete a survey, which was undertaken in March 2006. Data collected included indications for clozapine prescribing, the reasons why clozapine drug concentration monitoring was being utilised, and how often the psychiatrists might make use of it.
All data were analysed using Excel™ (Microsoft, USA). Unpaired Student's t-tests and linear regression analysis were performed using Graph Pad Prism™ (Graph Pad Software, San Diego, USA).
Indications, weight of patients, smoking status and other medication being administered to these patients were not recorded as this information was not available in the databases used.
RESULTS
A total of 353 patients were studied. Of these, 63% (n = 222) were male and 37% (n = 131) were female. The mean age was 42.7 years (SD = 16.1 years, range 15–88 years). The mean daily dose was 325 mg per day (SD = 177 mg, range 12.5–900 mg). The patient population had been treated with clozapine for a median of 4 years but with a wide scatter. Fifty patients (14%) had been treated with clozapine for greater than 9 years.
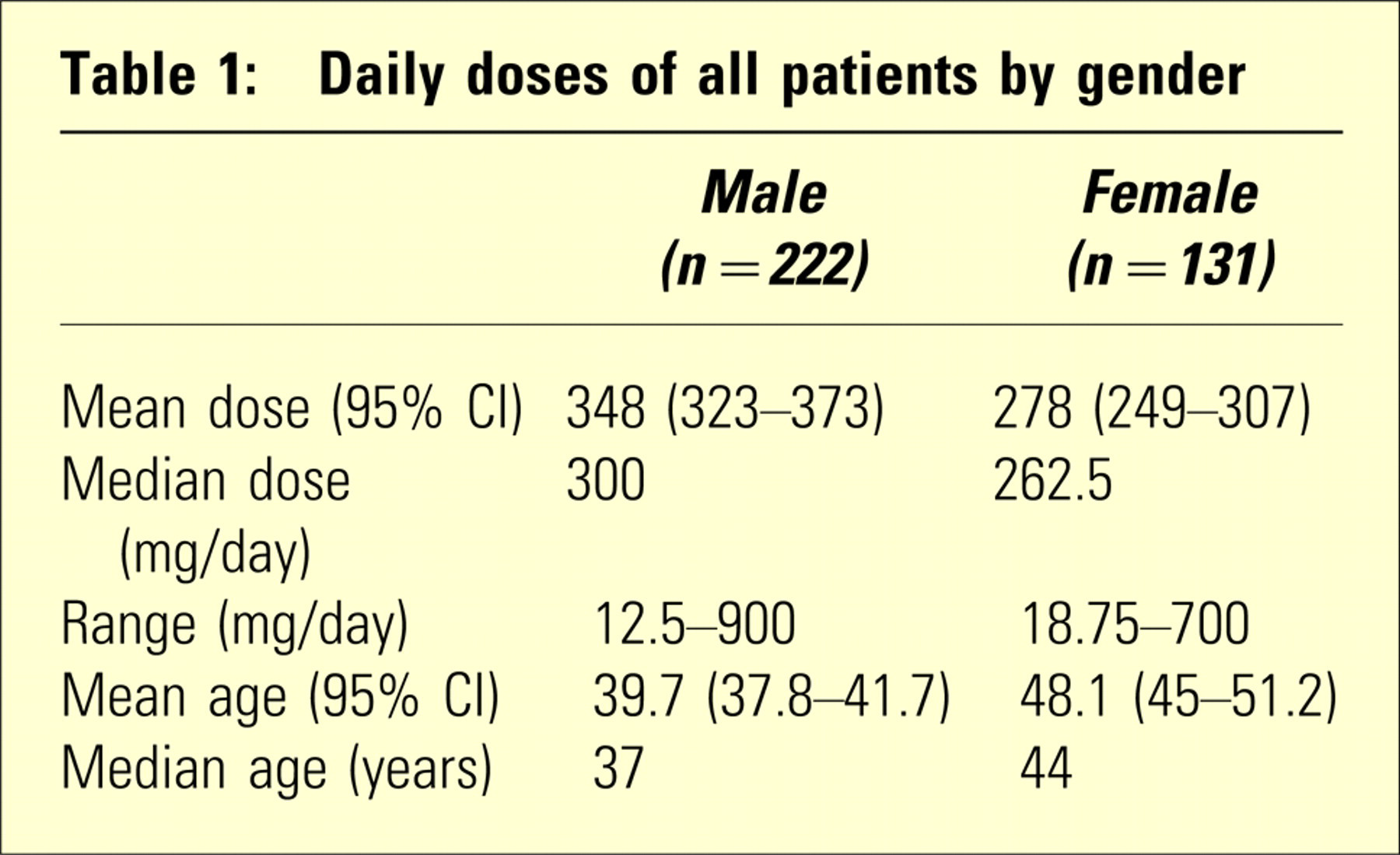
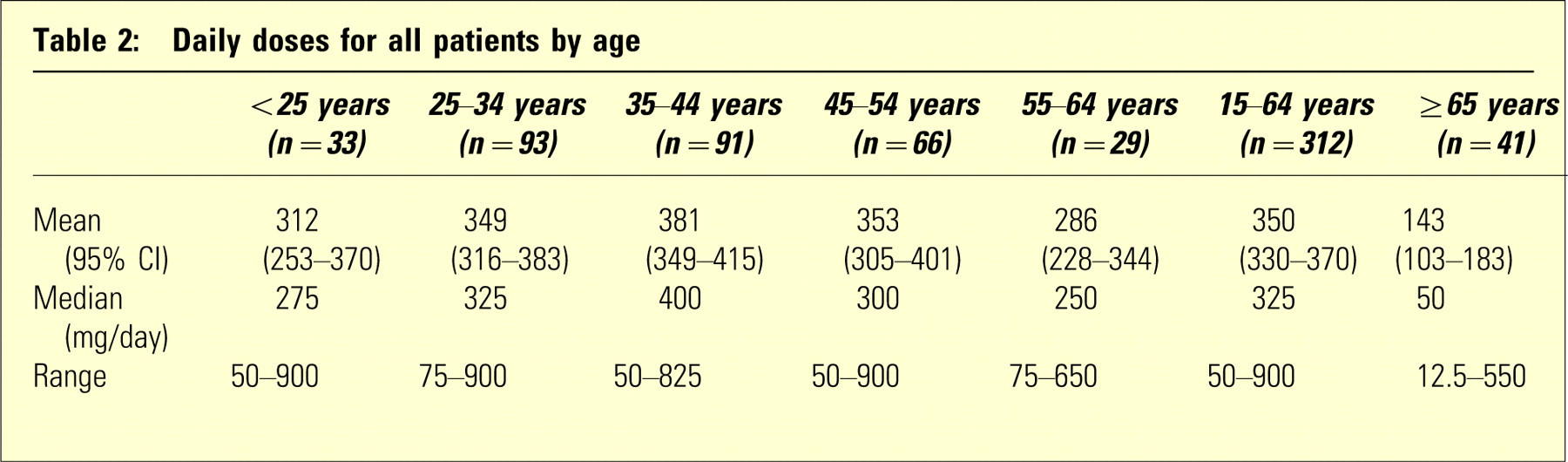
Daily doses for gender are shown in Table 1. The male patients had a significantly higher mean daily dose (348 mg) than the female patients (278 mg) (p < 0.001), but the mean female age (48.2 years) was significantly higher than the mean male age (39.7 years) (p < 0.0001). To correct for age, the mean daily doses for males and females were analysed in 10-year age bands. No significant difference was seen between males and females in any of the 10-year bands except for the 25–34 year age group, where the females were taking a lower mean daily dose of 276 mg (95% CI = 218–335) compared with the male mean daily dose of 369 mg (95% CI = 330–409; p < 0.05). There appears to be little change in dose under 65 years but a dramatic drop in dose thereafter (p < 0.0001) (see Table 2).
Daily doses of all patients by gender
Daily doses for all patients by age
Clozapine plasma concentrations, corrected for dose, were regressed against age (n = 25, females; n = 42, males). In females this demonstrated that increasing age correlated with increasing plasma concentrations/daily dose (r2=0.29, p < 0.001; Figure 1). This implies an age-related decrease in clearance in this group. No such correlation was seen in male patients.
Female clozapine plasma concentration/daily dose (Cp/dose) versus age.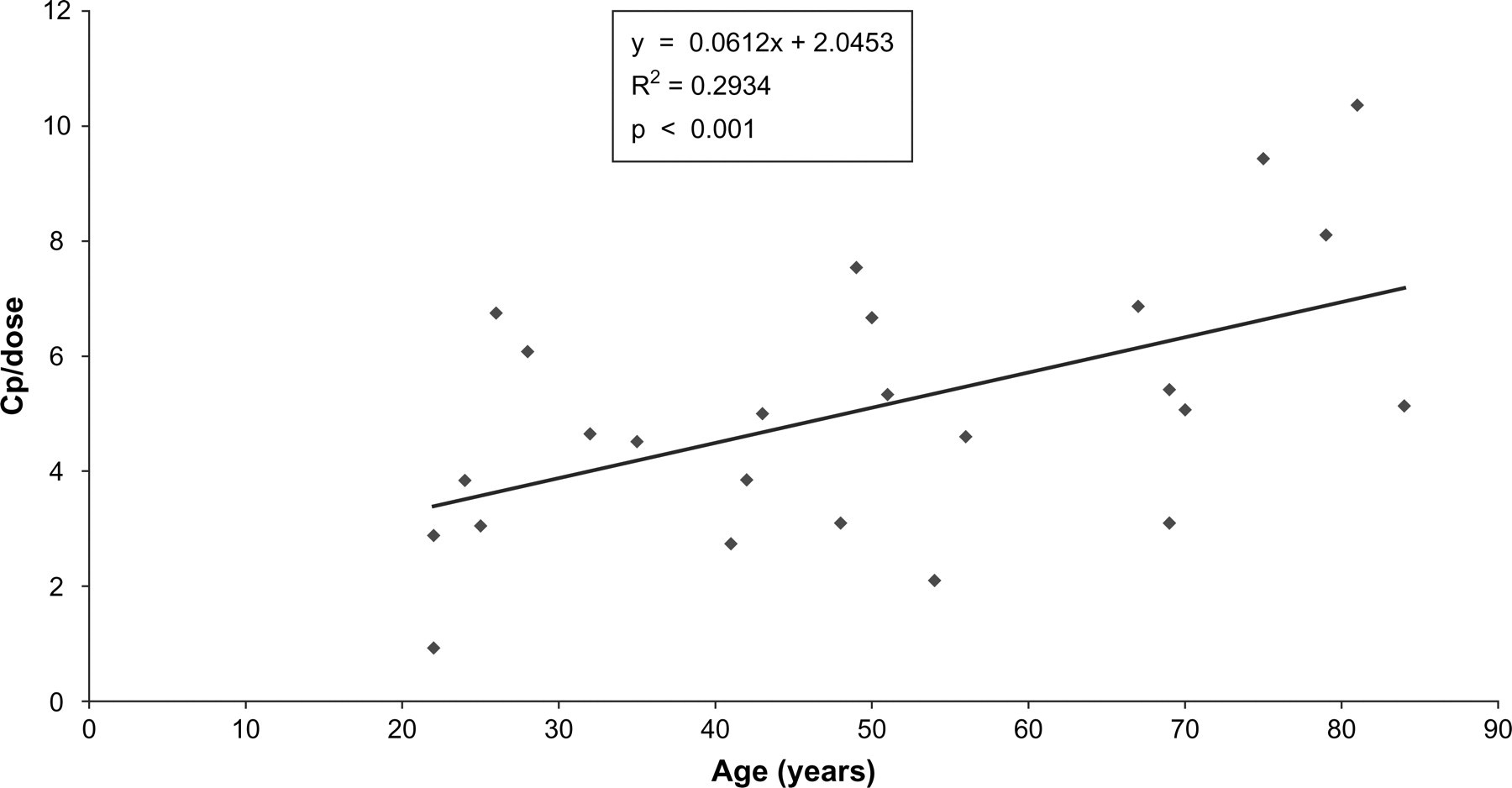
Thirty-four of 37 psychiatrists (91%) who were current prescribers of clozapine responded to the survey. Fifteen (44%) of these psychiatrists prescribed clozapine for unlicensed conditions, which included treatment-resistant bipolar disorder, treatment-resistant schizoaffective disorder and psychosis of Parkinson's disease.
Twenty-seven (79%) of the psychiatrists used drug concentration monitoring during clozapine therapy. Reasons for drug concentration monitoring were often multiple. Twenty-five (92%) monitored for compliance, 21 (78%) for toxic concentrations based on observed adverse effects, and 15 (56%) to compare the result with a desired therapeutic concentration range. Six (18%) used drug concentration monitoring on a regular basis (i.e. one to two times a month). Other psychiatrists commented that they might monitor concentrations intermittently or on a 6 monthly to annual basis.
Fifty-one percent of the population of 353 patients had a total of 825 blood samples assayed for clozapine plasma concentrations in the calendar year of 2005. Of these, 46% were monitored once or twice only and 47% were monitored between three and 11 times. A small minority of patients (9%) were monitored 12 or more times over the year and can roughly be split into two groups: (i) those monitored regularly (i.e. every full blood count taken on a 4 weekly basis was accompanied by a clozapine plasma concentration) and (ii) those admitted to Christchurch Hospital under the care of the accident and emergency or general medicine physicians. These patients had serial clozapine plasma concentrations measured over a short space of time (i.e. daily), perhaps to assess an overdose of clozapine.
DISCUSSION
It is useful to compare our results with others, both locally and from around the world. A study in Auckland and Northland looked at 954 outpatients on clozapine, aged between 15 and 64 years. The mean daily dose for all indications was 369 mg (SD = 153 mg), including 375 mg (SD = 150 mg) for the treatment of schizophrenia and 318 mg for the treatment of bipolar disorder (SD = 164 mg).[12] The mean daily dose in a British study in hospital inpatients was 450 mg for all indications.[7] The difference between these two results may relate to the populations studied, as the British study only included inpatients. Rosenheck et al. reported on the use of clozapine in the Veterans Authority health system in the USA[13] and found that the mean daily dose of clozapine for the treatment of schizophrenia only was 415 mg, and 207 mg for the treatment of bipolar disorder. Although we did not record indications for our patient population it would appear that our mean daily dose of 325 mg per day (SD = 177 mg) does not vary greatly from these studies.
The mean daily dose for the over 65 year group was 143 mg, which is significantly lower than that of the 15–64 year age group (mean = 350 mg). This could relate to increasing age, but more likely to indication. The psychogeriatricians often prescribe clozapine for drug-induced psychosis secondary to Parkinson's disease. There is good evidence that low-dose clozapine (less than 50 mg daily) is effective at treating this psychosis, without worsening motor control.[10] Unfortunately, indications were not available from the databases used.
The female patient data (Figure 1) demonstrated an apparent link between increasing age and decreasing clearance. The failure to observe the same effect in males was perhaps as a result of a clustering of patients aged between 25 and 35 years and an insufficient number of male patients greater than 35 years. This is worthy of further study.
Clozapine is only licensed for patients with treatment-resistant schizophrenia.[1] It would appear that prescribing for unlicensed conditions (i.e. other than treatment-resistant schizophrenia) is quite common, as 44% of psychiatrists were prepared to do this.
There were strong opposing views among the psychiatrists regarding the benefits of drug concentration monitoring, but the majority (79%) supported this practice.
There are several limitations to this study. The audit was retrospective. Medical records of patients were not reviewed, and thus the actual indications for patients who were on clozapine could not be assessed or compared to other data collected. Likewise, the patients’ weights were also unavailable. Clozapine is subject to drug interactions (including smoking), which may affect plasma concentrations and the daily dose of clozapine. It was not known what other medications patients were concurrently prescribed, nor the smoking status of the patients in this survey.
CONCLUSIONS
This study indicates that the daily doses of clozapine used for the 15–64-year-old Christchurch population are similar to that of the Auckland and Northland populations. The clozapine daily dose is much lower in patients over 65 years, largely due to different indications in this age group. There appears to be an age-related decline in clearance in females, which was not demonstrated in males. The use of clozapine for unlicensed indications appears to be common. Such indications included use in psychosis of dementia, psychosis of Parkinson's disease, and drug-induced psychosis of Parkinson's disease as well as other refractory conditions. Perhaps these indications should be formally licensed, in particular the use of clozapine in psychotic disorders occurring during the course of Parkinson's disease, which is a formal indication in the UK.[14] The use of drug concentration monitoring is widespread and used by around 80% of psychiatrists. Prescribing and monitoring would appear to be in line with normal practice elsewhere.