
Abstract
Throughout history, preferred settings for the treatment of mental illness have often changed as paradigms for mental illness and its management have changed. In recent decades, in developed countries, many of the older asylums have closed, or downsized dramatically, and new services in the community have been established in their place. 1 – 3 Several studies have reported on the consequences of this transition from hospital to community 4 – 6 and intra-hospital transfers between wards 7 – 13 on patient outcomes. Surprisingly few studies have compared the attitudes of patients and staff who have moved from one large psychiatric inpatient setting to another, given that physical settings and the hospital milieu are important variables in recovering from mental illness. 14 Two studies examined patient transfers between existing hospitals 15 , 16 and another assessed staff reactions to relocation in a new building. 17 In this paper, we report on patient and staff satisfaction ratings on the relocation of one of Australia's oldest and largest psychiatric hospitals, Sydney's Rozelle Hospital, to its new location.
In May 2008, a new purpose-built mental health facility was opened within the grounds of a General Repatriation Hospital in Concord, NSW, Australia. The new facility (“Concord Centre for Mental Health”) with 174 beds provides a setting whose physical characteristics – as other authors describing psychiatric centres or institutions champion 18 , 19 – are complementary to the therapeutic process offered within. In contrast to the old site, patients now have their own rooms within single storey units and are allocated to wards based on their phase of illness and treatment requirements. Patients are assessed and grouped into four general care models: those with recent onset of illness; those with relapsing illness requiring continuing care; patients with treatment-resistant illnesses; and recovery for those with persistent and enduring illness. Another major change in policy at the new facility is the mandatory requirement for a smoke-free environment within hospital grounds. Reduced smoking opportunities presents a particularly difficult issue for patients with mental illness. 20 , 21
Routine assessments of service satisfaction within the clinical setting may help to determine strengths and weaknesses of current service systems, and inform strategies and priorities for further service enhancement. 22 Thus, the relocation provided unique opportunities for the health service to create a better experience for both staff and patients. It is against this background that the current project was developed. The principal aims were to assess patient care delivery and to ascertain patient satisfaction levels and staff attitudes regarding their expectations, views and workplace satisfaction with the new premises.
METHOD
The study was conducted in July 2008, about 2 months after the relocation, to minimize the effect of any initial problems or frustrations likely to result from the move itself. 15 All patients admitted to the adult facilities were invited to complete a face-to-face survey until a sample size of 100 was achieved. Inclusion criteria were English speaking patients, age between 16 and 64 years, and absence of significant cognitive impairments or dementia.
During the same period, a modified version of the patient survey was sent by mail to all clinical nursing, medical and allied health staff at the new facility. To ensure confidentiality of responses, questionnaires were not coded. The study was approved by the Executive of the Hospital Human Research Ethics Committee.
The Inpatient Evaluation of Services Questionnaire was used in this study. 23 The instrument has good psychometric properties and contains five dimensions: (i) patient characteristics, (ii) service dimensions, (iii) patient expectations of treatment, (iv) patient intent to use services again, and (v) suggestions on improving the service. The items are rated using a five point scale: 1 = poor, 2 = fair, 3 = good, 4 = very good, and 5 = excellent. The 22 service dimension items were grouped into nine subscale scores with similar themes. Additional questions, constructed by the research team, included general questions about the new facility.
The survey that was sent to staff was similar to the patient questionnaire, with minor adjustments to account for contextual variations. Additional questions covered a range of aspects at the new workplace, such as access to professional supports, career, research and education opportunities, and staff safety.
Returned evaluations were analysed using the Statistical Package for the Social Sciences (SPSS) version 14 and are presented mainly as observed rates and simple frequencies. Comparisons were made between patient and staff ratings. Categorical variables were analysed using the Pearson chi-square test for independence, and group differences for continuous variables were analysed using one-way analysis of variance. Cronbach's alpha was used to assess internal consistency (reliability) of the patient and staff satisfaction scales.
RESULTS
Participant characteristics
Of 221 surveys sent to staff, 123 (56%) were returned. Nursing achieved a response rate of 59% (161 sent), medical staff 28% (29 sent) and allied health a response rate of 65% (31 sent). Over two-thirds (69%) of staff respondents had worked in mental health for more than 5 years (15% < 2 years, 16% 2–5 years). Of these, over half (55%) of the staff respondents had worked at the old facility for more than 5 years (3% never worked there, 18% < 1 year, 24% 1–5 years). Subgroup analyses indicated there were no significant differences between staff responses on any of the items below, based on professional background or years working in mental health, unless indicated in the text.
Of the 100 patients surveyed, 60% were male, 26% were 30 years or younger, 34% were aged 31–40 years, 20% were 41 to 50 years old and 19% were 51 to 64 years of age. About half (49%) of the patients had previously been admitted to the old facility one to five times, 15% of patients had more than five admissions to hospital and 36% had no previous admissions. Subgroup analysis indicated there were no significant differences between patients’ gender and number of previous admissions to the old hospital on response profiles, so the data were pooled prior to analysis for all patients.
Service dimensions
Table 1 presents the results of patient and staff ratings of items relating to services. Across most items, staff ratings were generally higher than those of patients and for four of the items ratings were significantly higher than patient ratings. For one item, availability of a primary nurse, patients’ ratings were higher (p = 0.002) than those of staff. Internal consistency (Cronbach's alpha) of the 22-item satisfaction survey was very high for both surveys (0.93 for staff and 0.96 for patients).
Patient and staff satisfaction responses for individual survey itemsa
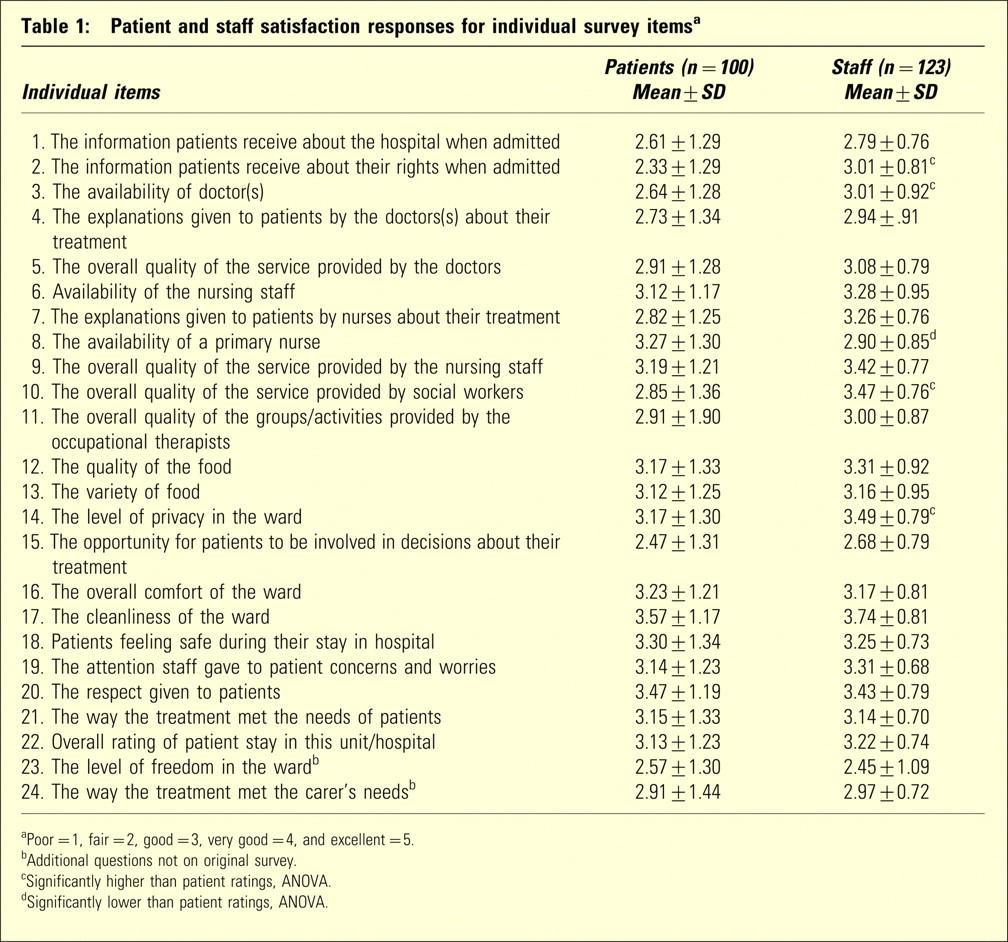
aPoor = 1, fair = 2, good = 3, very good = 4, and excellent = 5.
bAdditional questions not on original survey.
cSignificantly higher than patient ratings, ANOVA.
dSignificantly lower than patient ratings, ANOVA.
Table 2 shows the mean scores of service dimensions. For most dimensions, the mean scores of staff were slightly higher than those of patients, and for two dimensions (allied health and patient information) patients’ ratings were significantly lower than those for staff. Both staff and patients rated the ward environment the highest and doctor/medical services and patient information as the lowest.
Patient-ranked satisfaction scores of items grouped by service dimensiona
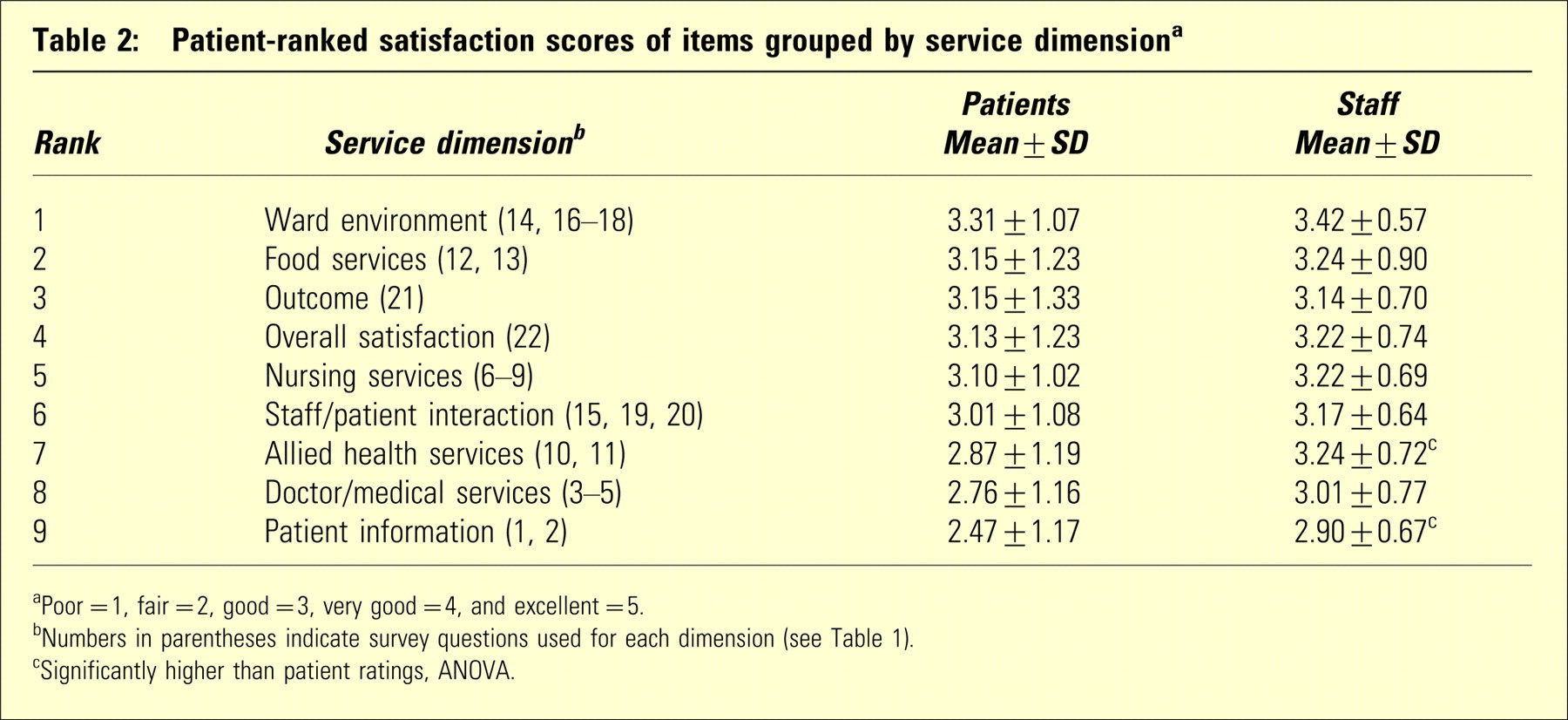
aPoor = 1, fair = 2, good = 3, very good = 4, and excellent = 5.
bNumbers in parentheses indicate survey questions used for each dimension (seeTable 1).
cSignificantly higher than patient ratings, ANOVA.
Expectations of services and treatment (patients and staff)
Expectations of services provided by doctors, nurses and allied health workers were significantly different between staff and patients. Perceptions of the service provideed by doctors was better (patients 39%, staff 24%), the same (patients 40%, staff 70%), and worse (patients 20%, staff 6%), than expected. The service provided by nurses (patients 47%, staff 25%; patients 43%, staff 71%; patients 10%, staff 4%), and alied health staff (patients 31%, staff 18%; patients 47%, staff 78%; patients 12%, staff 4%)rated better, the same and worse, respectively. The hospital food was rated better than expected by 66% of staff and 42% of patients. Forty-four percent of the patients rated their overall stay in hospital as better than expected, 39% that it was what they expected and 17% that it was worse than expected. The majority of staff (71%) rated the patient's hospital experience about the same as expected, 25% rated it better and 4% worse than expected.
Over half (58%) of the patients interviewed stated they would advise a friend with similar problems to come to the hospital, one-quarter (26%) would not and 16% were unsure. Fifty-five percent of the patients indicated that if they had to go into hospital again, they would like to return to this hospital. A quarter (24%) indicated that they would not wish to return to this hospital, and one-fifth responded they were unsure (21%).
Smoking
Fifty-nine patients (37 males, 22 females) identified themselves as current smokers and on average smoked 17 (SD 9.8) cigarettes per day prior to admission. Of the current smokers, 48 (83%) had reduced or quit smoking during their stay in hospital, 28 could recall being given information from staff about the hazards of smoking, 36 were given information about how to stop smoking and 50 were offered free nicotine replacement therapy. Only two (3%) stated they intended not to smoke following discharge from hospital and 11 (19%) others were unsure. About half the staff (51%) reported that patients had handled the no smoking rule better than expected, 31% said the response was about the same and 18% stated that the response was worse than expected. They also considered that staff had handled the no smoking rule better (31%), the same (52%), and worse (17%) than expected. There were no significant differences in patient response profiles between smokers and non-smokers.
Staff satisfaction with various aspects of the new facility
The majority of respondents (78–90%) were moderately or very satisfied with various aspects of the new facility, including the degree to which patients are helped effectively, job satisfaction/enjoyable work, support from colleagues in their work area, patient access to medical services, quality of care, teamwork, unit routines, and staff safety. Over two-thirds of respondents were satisfied with the time available to spend with patients and their families, continuity of care for patients, access to training and continuing education, support from management, access to professional supports, and career opportunities.
Staff were least satisfied with their prestige among the general medical community, dedicated staff facilities, information technology, staffing levels, research opportunities, and prestige among the psychiatric community.
Subgroup analyses indicated that medical staff were more critical of unit routines and quality of care, while allied health workers were least satisfied with staffing levels and teamwork compared with the other two groups.
Seventy percent of staff respondents considered the difficulties faced in delivering care at the new site to be the same or less difficult than at the old facility. About half of the staff considered the reality of the site to be about the same as their original expectations. Three-quarters (73%) said they felt proud about working in the mental health field and 86% said they would recommend the new facility to others as a place of work.
DISCUSSION
Findings show that patients were satisfied with several key aspects of the new facility, including comfort, safety, cleanliness, privacy and food. Many patients expressed dissatisfaction with information about the hospital, including information about rights and explanations about care. These findings resonate with other research on the topic, 24 and warrant further research attention. The provision of information has been linked to increased patient satisfaction 25 and increased treatment compliance. 26 It is important that the delivery of information is ongoing, as some patients may initially be unable to recall information about their care and treatment. 27 Information should also be user-friendly, as an absence of understanding of treatment impedes the opportunity for patients to be involved in decision-making, an area that achieved poor satisfaction ratings from both patients and staff in this study. Opportunity to be involved in decision-making is undoubtedly an important aspect of care, and there is a continued need to examine ways in which consumer information and opportunities to participate in treatment decisions can be improved. 24
The level of freedom on the ward was a source of dissatisfaction for patients and staff. In the new facility, acute wards are locked, so patients are not free to leave of their own accord, in contrast to some of the acute units at the former site. Combined with the introduction of the non-smoking policy at the time of relocation, this has been one of the more controversial aspects relating to care at the new facility. Ascribed benefits of locked units include decreased absconding rates, decreased need for high levels of close observation, increased security (enhanced patient safety), prevention of illicit contraband on the unit, ability to monitor unwelcome visitors, and provision of a level of control for staff. 28 , 29 It was reassuring to see that respect achieved high ratings within the new environment.
Staff expectations were generally met or exceeded in relation to the way patients and staff themselves had handled the no smoking rule; about one-fifth considered expectations to be worse. Over half of the patients smoked prior to their hospitalization, and while the vast majority had reduced or quit smoking during their stay in hospital with information and nicotine replacement therapy, only two patients intended not to smoke after discharge. There is opportunity to review incentives and support for this cohort to encourage continued abstinence following discharge.
For both patients and staff, expectations were mostly met or bettered. This meeting of expectations is reflected in the patients’ intent to use the service again (or recommend it to a friend) if admission should be required. About one-quarter of patient respondents did not wish to return to this hospital nor would they recommend it to others. Assessment of patient and staff satisfaction provides an indication of how well personal, emotional and physical needs are being met, 25 , 30 and there is further opportunity to evaluate other stakeholders’, such as carers’, views about the new facility.
The majority of staff respondents were satisfied with the degree to which patients are helped effectively, job satisfaction, the amount of support they receive from workplace colleagues, patients’ access to medical services, the quality of care provided, available parking facilities, teamwork, unit routines, and staff safety. Staff satisfaction depends on several factors, including opportunities for continuing professional education and professional supports. Over one-quarter of staff respondents were dissatisfied with resources, such as information technology, staffing levels, dedicated staff facilities and office space, and time available to spend with patients and their families. Similarly, prestige in both the medical and psychiatric community was a key area of dissatisfaction.
Feedback from the coalface of clinical work is important. Staff who are engaged in problem solving may reduce barriers to change 31 and contribute to enhanced services. Potentially, this may result in staff who are motivated, confident, and know that their input is valued. It was encouraging to see that the majority of staff respondents were proud about working in the mental health field and that the vast majority would recommend the new facility to others as a place of work. For staff, the reputation of a place as desirable in which to work is important and the associated high levels of staff satisfaction may contribute to retention and discourage absenteeism. Further research could explore personnel trends, such as sick leave, recruitment and attrition rates.
The study had some limitations. Although the overall response rate was satisfactory, there were fewer returned surveys for medical staff and thus not all disciplines were equally represented, an inherent problem in hospital-based studies with uneven staffing ratios of doctors and nurses. 32 The study was conducted a few months after the relocation and therefore could not compare attitudes before and after the move. Nevertheless, the study also had several strengths. These included a high internal consistency for both staff and patient satisfaction surveys, indicating good reliability of the instrument. The staff survey was anonymous and the patient interviews were conducted by the same two staff members, neither of whom provided direct care to the patients. Thus, the data collected were likely to reflect staff and patients’ true views about services.
CONCLUSION
To summarize, the findings provide patient and staff opinions of major changes within a single mental health service and we anticipate results will not only be of interest locally, but to other health service providers as well. The information gained from this study may help in planning, reduce difficulties experienced by patients and staff when relocating between treatment settings, and optimize continuity of care. 33 These results of the first 100 patients admitted to the new facility indicate that, despite initial trepidation, the move did not have any measurable negative impact on overall service provision and patient satisfaction. Constantly assessing areas of strength and weakness, from patient and staff point of view, will ultimately increase patient satisfaction and improve staff morale, while also improving the way services are delivered.
Footnotes
Acknowledgements
We thank Damien McCaul (CNC) for assisting with the data collection.