
Abstract
While benzodiazepine medications are an effective part of a clinician's armamentarium, there exist wide variations in physician prescribing habits, with inappropriate prescribing occurring in some instances. 1
Benzodiazepines were launched in the 1960s with distinct therapeutic advantages over their predecessor, the barbiturates. However, within a decade there was emerging awareness of the potential for tolerance and dependence, which could occur within weeks for short-acting forms. 2 More recently, non-reversible deleterious effects on cognition have been identified following chronic benzodiazepine usage. 3
Alprazolam is a benzodiazepine with a relatively short half life (12–15 hours). 4 In Australia, alprazolam is approved for subsidized prescription (authority only) under the Pharmaceutical Benefits Scheme (PBS) for the treatment of panic disorder where other treatments have failed or are inappropriate. 5
The diagnosis of panic disorder by primary care physicians can be compromised by a range of factors including the high rates of psychiatric comorbidity and prominence of somatic symptomatology associated with panic disorder. 6 , 7 The sequelae of panic disorder can be highly adverse, and may involve suicide attempts, alcohol abuse and relationship disruption. 8
Effective treatment options for panic disorder include psychotherapeutic measures (such as cognitive behaviour therapy) and pharmacotherapy. The latter includes both tricyclic antidepressants and selective serotonin reuptake inhibitors, with benzodiazepines as an adjunctive option. 9 , 10 Although it has been suggested that high potency benzodiazepines such as alprazolam have superior efficacy over lower potency benzodiazepines, a number of studies have demonstrated comparable efficacies between various benzodiazepines at equipotent dosages. 11 , 12
An important public health issue concerns opiate-consuming intravenous drug users (IDU) who also use benzodiazepines, with a substantial literature associating this practice with increased risk of overdose as well as with reduced health and social functioning. 13 , 14 Injection of benzodiazepines by this population has been associated with an exacerbation of these harms in addition to increased risk of blood-borne virus transmission and injection-related harms such as local infection, vascular damage, and gangrene. 15 This population who inject both opiates and benzodiazepines also have a greater likelihood of mood and anxiety disorders as well as polydrug abuse and dependence, presenting greater challenges to treatment services. 16
A variety of benzodiazepines have been favoured for injection by opiate users. In Australia during the early part of the decade, gel capsules of temazepam were preferred and were associated with serious adverse physical sequelae. 17 , 18 Public health measures involving policies that restrict access to benzodiazepines which are favoured for injection by opiate users had positive outcomes in Britain. 19 In Australian settings, in 2002 attempts were made to change physician behaviour through the introduction of an authority prescription requirement for temazepam capsules. 20 However, it was found that the policy change had little effect on the frequency of injection of temazepam capsules among IDU, as the drug was able to be accessed from private scripts (not involving the PBS) and diverted sources, resulting in a view that additional strategies were required.
Temazepam gel capsules were removed from the market in 2004, and subsequently a marked reduction in benzodiazepine injection was noted among IDU, 21 particularly among those in heavily populated capital cities. 22 However, in relatively isolated regions, such as Tasmania and the Northern Territory, benzodiazepine injection continued unabated. 20 In Tasmania, alprazolam largely replaced temazepam gel capsules as the benzodiazepine of choice for injection, with diazepam injection less common and remaining at rates similar to those before the temazepam capsule's market removal. 23 Tasmania traditionally has a low availability of heroin, with diverted pharmaceutical opioids typically used by IDU; the practice of injecting alprazolam with opioids has been reported as producing a heroin-like ‘high’. 22
In Tasmania, the per-capita prescription rate for alprazolam was more than double the rate nationally. In recent months, repeated cases of morbidity and mortality in relation to alprazolam and opiate co-administration were detected. 24 In response, a Working Party, comprising representatives of the Royal Australian and New Zealand College of Psychiatrists and Royal Australian College of General Practitioners, as well as state government agencies comprising Pharmaceutical Services and Alcohol and Drug Services, was convened in December 2006 with the aim of improving the quality of health care by addressing the potential over-prescribing of alprazolam in Tasmania.
As physician prescribing is subject to multiple influences, including education, patient preferences and patient pressure, 25 – 27 the intervention comprised two components: educational sessions for general practitioners, and regulatory changes to the prescription of alprazolam.
In June 2007, an education session was delivered to general practitioners in each of the three major regions of Tasmania. These were delivered by psychiatrists, pharmacists and addiction medicine specialists, and encompassed the diagnosis and potential sequelae of panic disorder, the evidence base for benzodiazepine prescription for panic, the issue of benzodiazepine abuse among opiate users, and the forthcoming prescription regulation changes. Further detail on the content of these sessions can be provided on request.
Regulatory changes for alprazolam were introduced on 1 September 2007. These did not change the scheduling of the drug (S4D under the Tasmanian Poisons Declared Restricted Substance Order 1990) but placed additional requirements on its prescription and dispensing, including: pharmacies being required to provide monthly reporting of all alprazolam prescriptions dispensed (along with Schedule 8 drug reporting); application for authority to prescribe being required where alprazolam is prescribed in excess of 4 weeks to patients who are also prescribed opioid medication; patients enrolled in methadone or buprenorphine maintenance programs being required to have explicit approval from the clinical director overseeing this program to receive prescriptions of alprazolam; and a requirement that medical practitioners are notified not to prescribe alprazolam to patients currently receiving benzodiazepines and/or opioids from another medical practitioner.
The current study aimed to assess the impact of this combined intervention through an analysis of prescription data in the period before and 12 months following the intervention.
METHODS
Prescription data were derived from two sources. First, all alprazolam prescriptions (0.25, 0.5, 1.0, 2.0 mg) subsidized through the PBS and Repatriation Pharmaceutical Benefits Scheme (RPBS) for the period 1 January 2000 to 31 August 2008 were collated for Tasmania and the rest of Australia, and adjusted for population using Australian Bureau of Statistics annual population data. Second, Tasmanian data for the numbers of individual patients receiving alprazolam prescriptions via private or subsidized prescriptions were accessed from the Tasmanian Pharmaceutical Services Branch. These were examined for the period 1 September 2007 to 30 September 2008. It should be noted that information in both datasets relates to prescription of alprazolam for any purpose (i.e. both on- and off- label applications), and no inferences can be made as to the clinical context of any of these prescriptions. Polynomial regression models and descriptive statistics were conducted using SPSS 16.0. Linear trends are akin to saying that the relationship between time and prescription can be described as following a simple straight line (as one increases, so does the other), while quadratic trends suggest that there is a change in the direction of this relationship (as time increases, prescriptions increase to a point after which they begin to fall). Whether such trends provide a good description of the observed relationship between time and prescriptions is described by the coefficient of determination, R2, which can take values between 0 and 1, where a value of 1 indicates that the regression line perfectly fits the data. In addition, t-tests for linear and quadratic coefficients provide an assessment that these differ significantly from zero (failure to attain statistical significance for a linear coefficient, the ‘slope’ of the line describing the relationship between time and prescriptions, would suggest that prescriptions remained stable over time).
RESULTS
At the time of the study intervention, Tasmania had 551 practising general practitioners. Invitations for one of the three educational sessions were sent by the divisions of general practice. Total attendance was estimated at 142 across the sessions (approximately 26% of GPs).
Population-adjusted rates of PBS/RPBS subsidized prescriptions (Figure 1) demonstrate that between 2001 and 2007, prescription rates in Tasmania were, on average, more than twice that of the rest of Australia. Following the interventions, there appears to be a decline in the prescription rate in Tasmania, which is not apparent in the national trend. This apparent decline in subsidized prescriptions could not be accounted for by an increase in non-subsidized (private) alprazolam prescriptions. Such an inference can be made as during the September 2007 to September 2008 period the rate of private alprazolam prescriptions in Tasmania was, on average, 30% of the total prescriptions, and this rate was quite variable; there was no suggestion of any increasing linear trend: t(11) = 1.3, p=0.19. Because there was no suggestion of any systematic change in the rate of private prescriptions of alprazolam in Tasmania after the interventions, this means that any changes in subsidized prescriptions in the months following the interventions can not be simply attributed to patients shifting from subsidized to private prescriptions. As such, it is appropriate to interpret the PBS/RPBS data to examine the influence of the interventions.

Population-adjusted PBS and RPBS prescription rates for Tasmania and Australia, 2000–2008.
An annual trend is apparent in the prescription rate data, which likely reflects the influence of the PBS prescription ‘safety net’ program allowing more individuals to access subsidized alprazolam prescriptions once they have expended a given amount on prescription medications during the calendar year. To overcome this within-year variability, a 12 month period (1 September–31 August) was analysed for trends (Figure 1). National prescription rates (excluding Tasmania) follow a steadily increasing (linear) trend over the 6 years prior to the intervention (prescription rate = 0.05 (year) + 1.5, R2 = 0.92, t(5) = 7.3, p<0.01) which remains linear when the year following the intervention is included (prescription rate = 0.04(Year) + 1.5, R2 = 0.91, t(6) = 7.6, p<0.01). For Tasmania, there was a steady linear increase in alprazolam prescriptions in the 6 years prior to the intervention (prescription rate = 0.16 (year) + 3.0, R2 = 0.88, t(5) = 6.0, p<0.01), but when the year following the intervention is included, a linear trend is no longer an adequate fit to these data (prescription rate = 0.08 (year) + 3.2, R2 = 0.32, t(6) = 1.7, p = 0.14), and instead a quadratic trend (a curved line) is required to fit the reduced rate of prescription following the intervention (prescription rate = 0.56 (year) −0.05 (year)2+2.4; R2 = 0.89, linear: t(5) = 5.9, p < 0.01; quadratic: t(5) = 5.1, p<0.01).
In terms of total numbers of subsidized prescriptions, in Tasmania, alprazolam prescriptions fell from 19 228 in the 12 months between September 2006 and August 2007 to 16 261 in the same period for 2007–08, a 15.4% decline. By contrast, in the rest of Australia, subsidized prescriptions increased 1.3% in this same period (363 472 for September 2006–August 2007, 368 355 in the same period in 2007–08). Corresponding figures for all other subsidized benzodiazepine prescriptions showed slight declines in this period both in Tasmania (6.9% decline from 219 701 in the 2006–07 period to 204 471 in the subsequent year) and in the rest of Australia (5.3% decline from 5 442 934 to 5 153 262 in these respective periods). Subsidized prescription rates for all other benzodiazepines have followed strongly linear annual declines in the past 5 years (R2 = 0.79 and 0.90 for Tasmania and the rest of Australia respectively).
The number of individual patients receiving any alprazolam prescriptions in Tasmania (including both subsidized and non-subsidized) was only available for analysis for the 13 months following the intervention (Figure 2). The number of individuals receiving co-incident alprazolam and opioid prescriptions declined linearly in this period (patients = − 6.3 (month) + 246.1, R2 = 0.59, t(11) = 4.0, p<0.01). The number of individuals receiving coincident alprazolam and opioid prescriptions for longer than 1 month remained low, with such patients comprising less than 2% of the total number of individuals receiving alprazolam prescriptions during this period. For individuals receiving alprazolam prescriptions but not also prescribed opioids, a linear trend did not fit the data (R2 = 0.28, t(11) = 2.0, p = 0.07) and instead a quadratic pattern was apparent, suggesting an initial increase in patients in the first few months following the interventions and possible indications of a slight decline in latter months (patients = 1192.7 + 50.4 (month) − 2.9 (month)2, R2 = 0.52, t(10) = 2.7, p = 0.02 (linear); t(10) = 2.2, p = 0.05 (quadratic)).
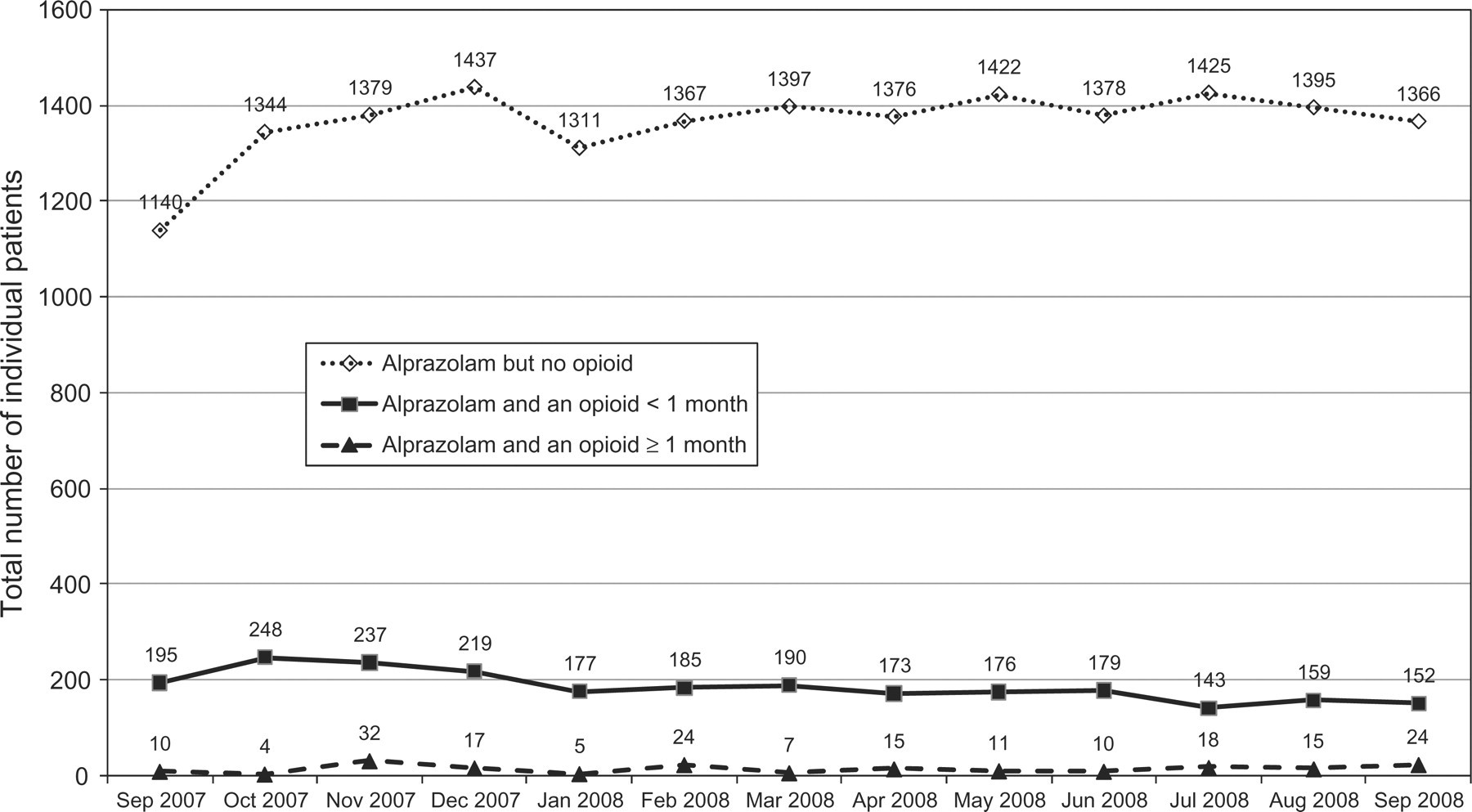
Monthly numbers of individual patients receiving alprazolam in Tasmania in the 13 months following the intervention.
DISCUSSION
This intervention was associated with a reduction in the number of subsidized prescriptions for alprazolam in Tasmania in the 12-month period following the intervention. This contrasted with trends for prescription rates on the Australian mainland which showed no change in this period. There was no evidence for compensatory increases in private prescriptions for alprazolam, nor of switches to other benzodiazepines. Importantly, the number of individuals being co-prescribed alprazolam with opioids, the primary target group for the intervention, declined in the months following the intervention.
Studies regarding physician education have generally found greater efficacy where interventions utilize opinion leaders to disseminate information. 28 Other proven educational strategies include the use of written reminders and outreach programs where the intervention occurs in the physician's office. 29 In contrast, formal CME conferences have shown inconsistent effects upon physician behaviour. 29
The current study adopted an opinion leader approach to the three GP education sessions, deploying the Clinical Director of Tasmanian Alcohol and Drug Services, a senior psychiatrist in private practice, a senior pharmacist from the Department of Health and Human Services and a psychiatrist with an addiction psychiatry subspecialty who was chairman elect of the Tasmanian branch of the RANZCP.
Regardless of the type of educational intervention employed, inconsistencies in results occur across physicians by virtue of differences in their motivation levels and readiness to change and the degree to which they consider their current practices to be problematic. 29
While the success of educational approaches is reliant upon a physician's motivation for increasing their clinical competence, regulatory changes utilize an external pressure to change prescribing habits so have sometimes been classified as a coercive technique. 30 Studies suggest that strategies designed to bring about changes in clinical practices such as physician prescribing may be more effective when they involve a series of interventions in which education is one arm of a multi-faceted approach. 30 , 31
Limitations
This study had a number of limitations. Ideally, a monthly assessment of the number of individuals receiving both subsidized and non-subsidized alprazolam prescriptions in the period prior to the intervention would have allowed clearer identification of the impact of the intervention.
The intervention comprised two complementary components, with the education sessions focused on the rational prescription of alprazolam generally, and the regulatory changes targeting patients receiving co-prescriptions of alprazolam and opioids. However, the available data did not enable quantification of the relative contributions of these components to the reduction in alprazolam prescription. Similarly, it was not possible to compare prescribing patterns between medical practitioners who attended the education sessions and those that did not, nor to control for other external influences on physician prescribing. However, the naturalistic design employed here provides an appropriate global assessment of the impacts of the overall intervention program.
The proportion of alprazolam prescriptions that were written from physicians other than general practitioners was not measured. These physicians were not subject to the education intervention yet were potentially affected by the regulatory changes.
Finally, given the important health implications, more data are needed in regard to the proportion of alprazolam prescriptions being made to opiate-consuming IDU and whether this demographic is instead more commonly receiving alprazolam from diverted sources.
CONCLUSION
Interventions in the form of educational meetings based on current evidence-based practice are an important and effective method to improve the quality of health care. In this case, the potential benefits of physician education were supplemented by the introduction of appropriate pharmaceutical regulatory measures, highlighting the value of collaboration between colleges and health services to achieve changes in prescription habits. Future actions could include designing regulations which address rational alprazolam prescribing in non-opiate-using populations.