
Abstract
In the clinical application of traditional porcelain-fused-to-metal crowns and bridges, porcelain chipping has appeared as the major problems encountered by dentists. Once fracture occurs, neither aesthetics nor chewing efficiency remains. It is difficult to meet clinical needs with current repairing options. Self-glazed zirconia has been developed recently and is widely used in crowns, bridges, and veneering owing to its high strength, low wear on opposite teeth, and aesthetic appeal. In this study, we explore the application prospect of the chipped porcelain-fused-to-metal restoration repaired by the novel self-glazed zirconia veneering with a digital workflow. The results demonstrated that self-glazed zirconia can meet both the aesthetical and functional requirements of anterior and molar teeth in a timely and efficient manner.
Introduction
Crowns and bridges have gained considerable popularity because of their strength, comfort and aesthetics in oral clinical practice. Traditionally, metal-based reconstructions for fixed dental prostheses were considered as the gold standard [1]. In clinical practice, PFM crowns and bridges are the most frequently used traditional type of restoration for fixing tooth defects and dentition defects. Despite being a mature technology (i.e. developed more than 50 years ago), porcelain fused to metal still suffers from clinical failures, mostly due to chipping or fracturing of the veneering ceramic [2-4]. The chipping or fracture of the PFM restorations involves the following factors: (1) incorrect design of the framework, which results in concentrated areas of stress; (2) a wide variation in porcelain thicknesses; (3) the large thermal expansion of porcelain and metal; (4) improper operation during production; (5) being struck in the seating process; (6) occlusal disorders; and (7) accidental impact or occlusion [5–10].
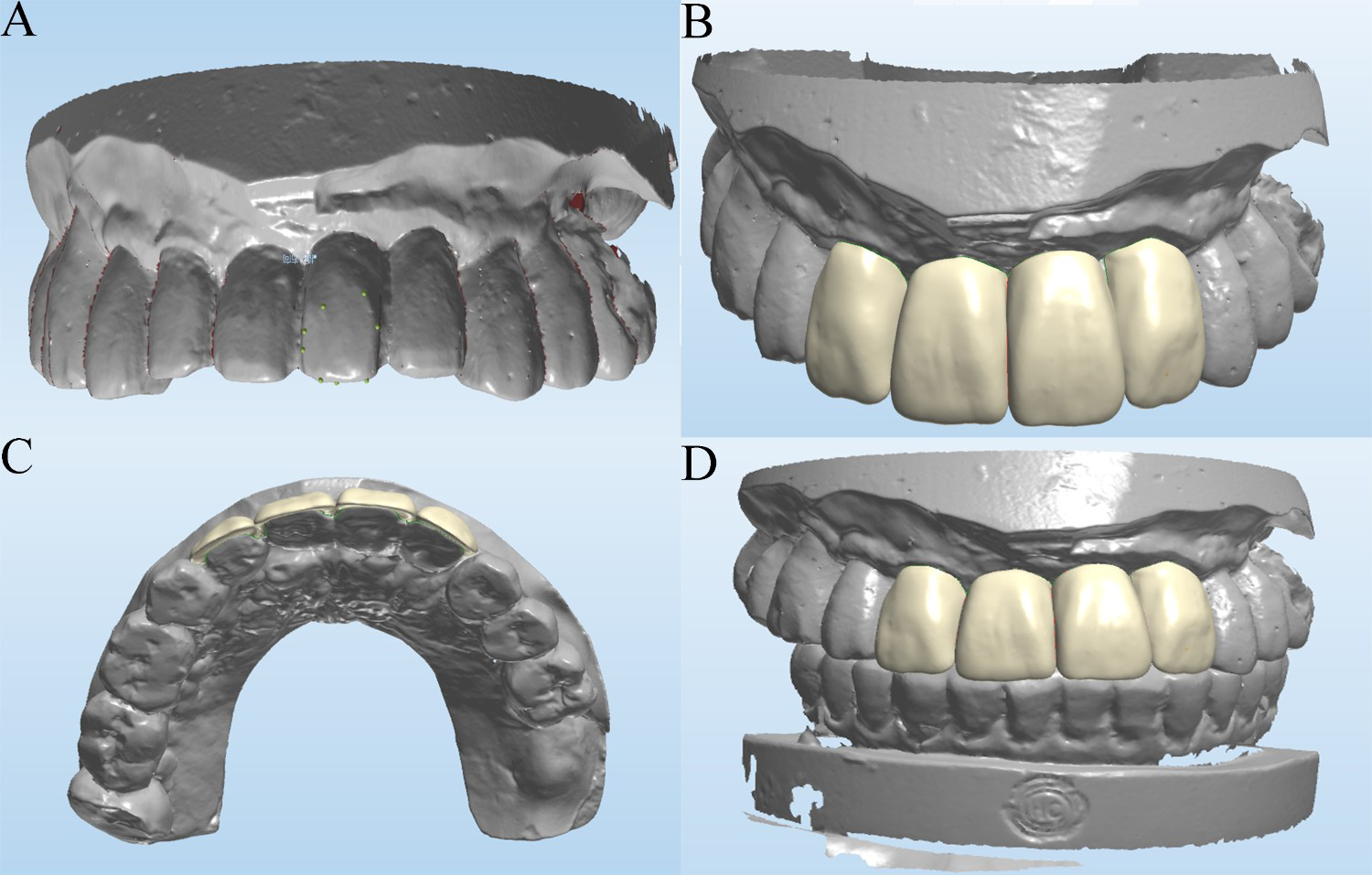
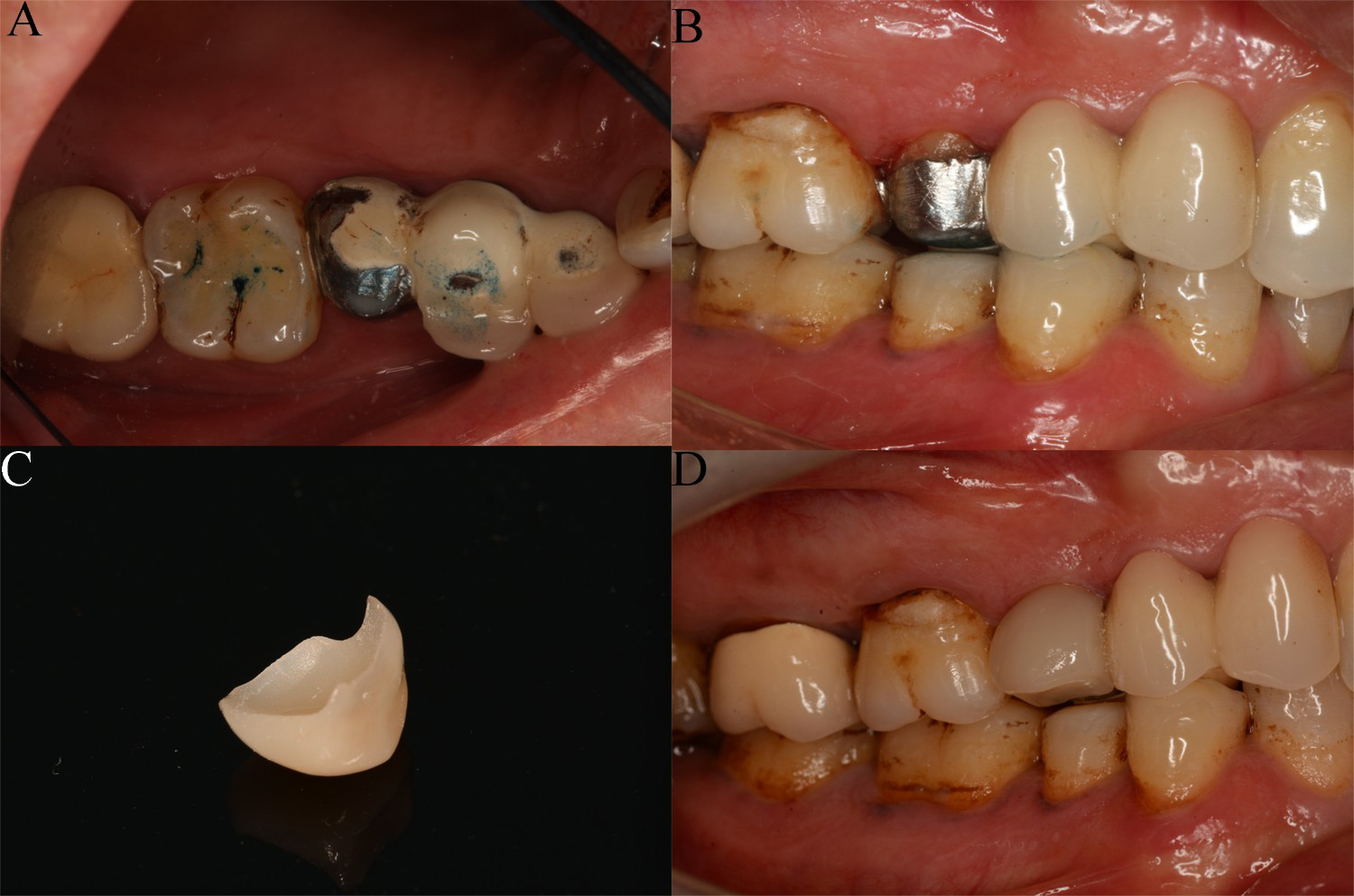
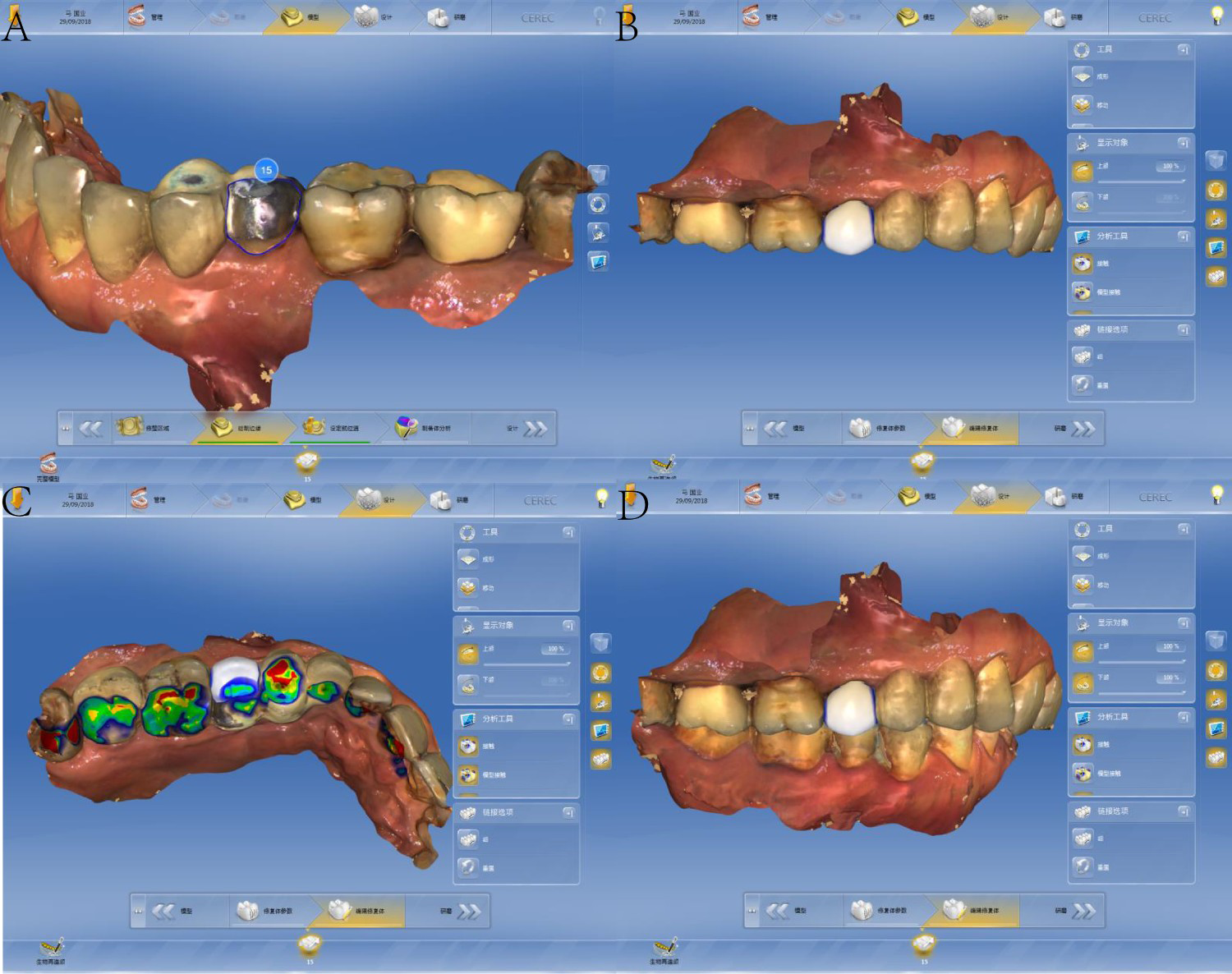
Case study 1. Intraoral photos demonstrating the process of repairing chipped porcelain for traditional bridges on the anterior. (A) Initial condition; (B) 3D printing of novel self-glazed zirconia veneering prostheses; (C) labial view; (D) intaglio view. (A) Digital model based on scanned data; (B) and (C) CAD morphology of veneering; (D) CAD of the occlusion. Case study 2. (A) Labial chipping in buccal and occlusal of 15; (B) preparing 15 PFM crown by polishing part of the occlusal porcelain and all of the buccal porcelain; (C) 3D printing novel self-glazed zirconia veneering; (D) 3D printing novel self-glazed zirconia veneering prostheses repair. (A) Digital model based on scanned data; (B) and (C) CAD morphology of veneering; (D) CAD of the occlusion.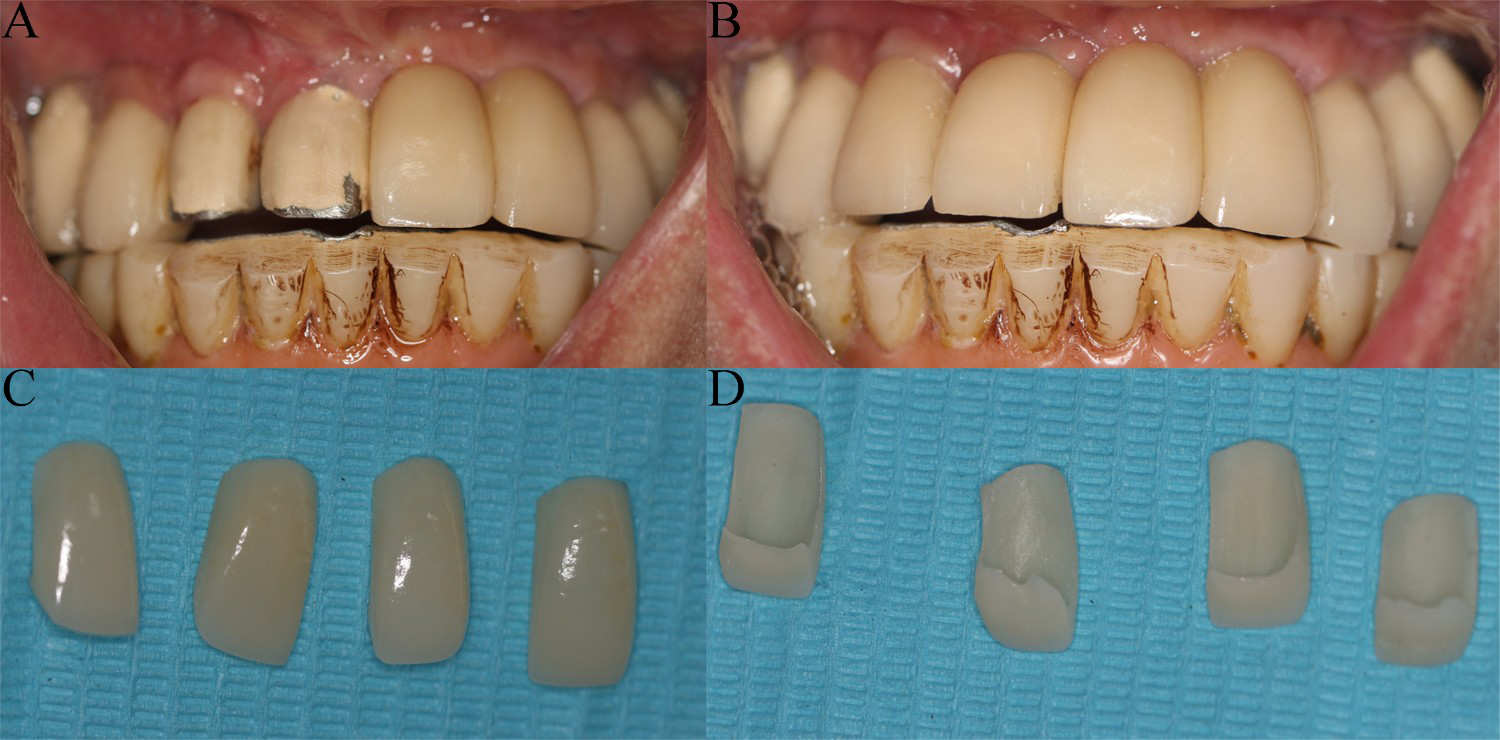
The 3D printing of novel self-glazed zirconia is an advantageous candidate for repairing the chipped porcelain of traditional restorations; this approach represents a new type of full-contour zirconia monolithic prostheses produced by 3D gel deposition technology [11]. The results have good optical transparency and colour masking effect, with a thickness of 0.6 mm, which is sufficient for obtaining ideal colour masking. Owing to high strength and low wear to the opposite teeth, the 3D printing of novel self-glazed zirconia is suitable for repairing the chipped porcelain of traditional restorations [12]. The application of digital design and manufacturing avoids issues of incorrect design due to lack of experience [13].
Methods
In this study, we selected 30 patients who were treated with novel self-glazed zirconia veneering to repair chipped Porcelain-Fused-to-Metal restoration at the Affiliated Stomatological Hospital of Guangzhou Medical University from September 2017 to March 2018. The inclusion criteria were as follows:
Chipped porcelain-fused-to-metal restoration needed repair No obvious mental illness No obvious temporomandibular joint disease No occlusion dysfunction No serious systemic disease.
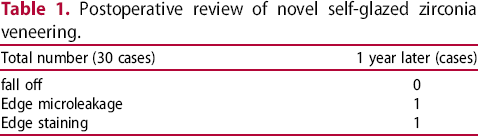
The repair effect was reviewed and evaluated at 12 months after the repair treatment. Evaluated by two restoration specialists, according to restoration retention., edge microleakage, and edge staining, etc.when there is any one of the prosthesis fracture, the prosthesis fall off, etc., and need clinical intervention, the evaluation is a failure of the restoration. When the opinions are not uniform, the party with the low standard shall prevail.
Two clinical cases
Case 1
A patient suffered chipping of a 12–22 PFM bridge, with labial chipping in 12 and 11 and incisal chipping in 21 and 22. After clinical and radiological assessments, two treatment plans were presented: (1) producing a new restoration after removing the bridge and teeth preparation by computer-aided design/computer-aided manufacture (CAD/CAM); (2) polishing the labial and incisal porcelain layer and producing a 3D printing novel self-glazed zirconia veneer.
The patient was unwilling to remove the prosthesis and had a high requirement for aesthetic effect, and so the second option was chosen. We prepared the 12–22 PFM bridge by polishing part of the palatal porcelain and all of labial and incisal porcelain. Then, using optical digital scanning, we obtained digital data. And we that allowed the chair-side design and production of a 3D printing novel self-glazed zirconia veneer with the help of computer aided design and manufacturing. Finally, the 3D printing novel self-glazed zirconia veneer was bonded by super bond with only minimal clinic adjustment (Figures 1 and 2).
Case 2
A patient suffered chipping of a 13–15 PFM bridge, with labial chipping in the buccal and occlusal of 15. After clinical and radiological assessments, two treatment plans are were presented: (1) producing a new restoration after removing the bridge and performing teeth preparation by CAD/CAM; and (2) polishing part of the occlusal porcelain and all of the buccal porcelain and producing a 3D printing novel self-glazed zirconia veneer.
The patient was unwilling to remove the prosthesis, and so the second option was chosen. We prepared a 15 PFM crown by polishing part of the occlusal porcelain and all of the buccal porcelain. Then, using optical digital scanning, we obtained digital data that allowed the chair-side design and production of a 3D printing novel self-glazed zirconia veneer with the help of computer aided design and manufacturing. Finally, the 3D printing novel self-glazed zirconia veneer was bonded by super bond with only minimal clinic adjustment (Figures 3 and 4).
Results
Postoperative review of novel self-glazed zirconia veneering.
Discussion
To solve various tooth defect problems, traditional fixed restorations are considered a good choice from both aesthetical and functional points of view. However, with increasingly popularity of fixed restorations, porcelain chipping has become a problem in the past few years. Some studies have shown that the rate of porcelain chipping is as high as 3%–25% in 3–5 years [14-16]. Once fracture and chipping occur in PFM restorations, neither aesthetics nor chewing efficiency remain [17].
Clinical repair options include removing the entire restoration and replacing it with a new restoration, reapplying the broken piece of porcelain with resin cement, replacing the missing piece of porcelain with composite-based resin and preparing the restoration for a new veneer and adhesively bonding the ceramic veneer onto the existing restoration [5,18]. However, these approaches suffer from a number of issues. First, incorrect design of the framework would result in stress concentration areas. Second, for patients with improper habits, the approach is both difficult and can cause pain and irreversible damage to the tooth and periodontal when removing the entire restoration; it is also costly and time consuming. Reapplying the broken piece of porcelain with resin cement can match the shape and colour well, but is restricted to broken pieces of porcelain that are intact and of sufficient size. Simultaneously, dentists should not polish all of the porcelain layer in case they impact on the bonding effect. Finally, it is difficult to meet aesthetic requirements [19]. To saving time and money, some dentists prefer composite-based resin to repair[20]. However, the composite-based resin has the risk of aging, discoloration and secondary caries. Lastly, for chipping defects in anterior teeth, preparing a new veneer that is adhesively bonded onto the existing restoration is a possible approach; however, this option requires high precision and sufficient space for the repair work. Furthermore, the process is very complex.
Novel self-glazed zirconia produced by 3D printing has high strength and good aesthetical appeal. This approach avoids the risk of porcelain chipping by using gel deposition technology to produce a full-contour zirconia monolithic prostheses without veneering porcelain [21]. At the same time, owing to the material surface structure, 3D printed novel self-glazed zirconia is as smooth as natural enamel, and low wear to the opposite teeth after repeated chewing [22]. It can effectively avoid the errors caused by model preparation and unreasonable shape design caused by technicians’ inexperience by using digital optical scanning and computer-aided design. The thickness of 3D printing novel self-glazed zirconia veneering can reach an astonishing 0.2 mm; although, a minimum thickness of 0.6 mm is need to obtaining the ideal colour masking effect. A study has shown that 60% of the failures were observed at the labial, 27% at the buccal, 5% at the incisal, and 8% at the occlusal regions [23]. So the 3D printing novel self-glazed zirconia veneering described here used the wrapping type, which looks like L or V and gives the veneer a retention cap structure similar to a full crown. It has advantages in appropriateness of placement, strength, and aesthetic appearance [19]. Wrapping provides a larger specific surface area, which means that the 3D printing novel self-glazed zirconia veneering bonds more closely with the base crown. The high strength and aesthetic characteristic are obtained through piled up colloid zirconia with different colours and sizes, which allow for nano-gradient structures during 3D printing [11,24,25]. The 3D printing of novel self-glazed zirconia not only masks the discoloration of teeth, but also significantly improves the bonding force of the restoration because of a unique porous light scattering layer on its surface. The micro-nano technology endows an irregular porous structure on the tissue surface. Given its 4-META content, Super-Bond C&B forms strong bonds with dental alloys and a wide range of porcelains [5,26,27]. Consequently, the 3D printed novel self-glazed zirconia veneer bonds more closely with the base crown by increasing the specific surface area, which can effectively reduce veneer shedding. Finally, 3D printing of novel self-glazed zirconia veneering can mask colour effectively and achieve high light transmittance, much like natural enamel [28], which removed the need for extensive polishing.
Conclusions
The 3D printing of novel self-glazed zirconia veneering not only saves time and money, but also improves the aesthetics and accuracy of repairs to the chipped porcelain of traditional crowns and bridges. It reduces the requirements of repair space and effectively avoids the problem of further damage (e.g. the repair failing off). This approach provides a new and effective way to repair the chipped porcelain of traditional crowns and bridges.
Footnotes
Disclosure statement
No potential conflict of interest was reported by the authors.