
Abstract

The National Mental Health Policy [1],[2], released in 1992, has been something of a guiding framework for mental health reform in Australia over the past 8 years. Its implementation was guided, between 1993 and 1998, by the (First) National Mental Health Plan [3]. This Plan was refined and the Policy implementation continues under the Second National Mental Health Plan [4]. There was no specific indication in the Policy that Australia needed, or would in fact undertake, studies to generate national information on the mental health status of the population.
In 1993 I became Chair of the Australian Health Minister's National Mental Health Working Group (NMHWG) which was to oversee the implementation of the National Mental Health Policy and Plan. In that year, I developed a template to describe the elements of the reform process (Figure 1) which has only been published once, in the 1995 National Mental Health Report [5]. The focus of mental health reform at that time was largely on structural changes in public mental health service delivery [6]. Although the template recognised the importance of estimating the population need for services, as well as the population outcomes of any changes arising from the reforms, I considered that national-level, overseas studies, supplemented by local studies which had been carried out within Australia, would suffice in making these estimations
National mental health reform template.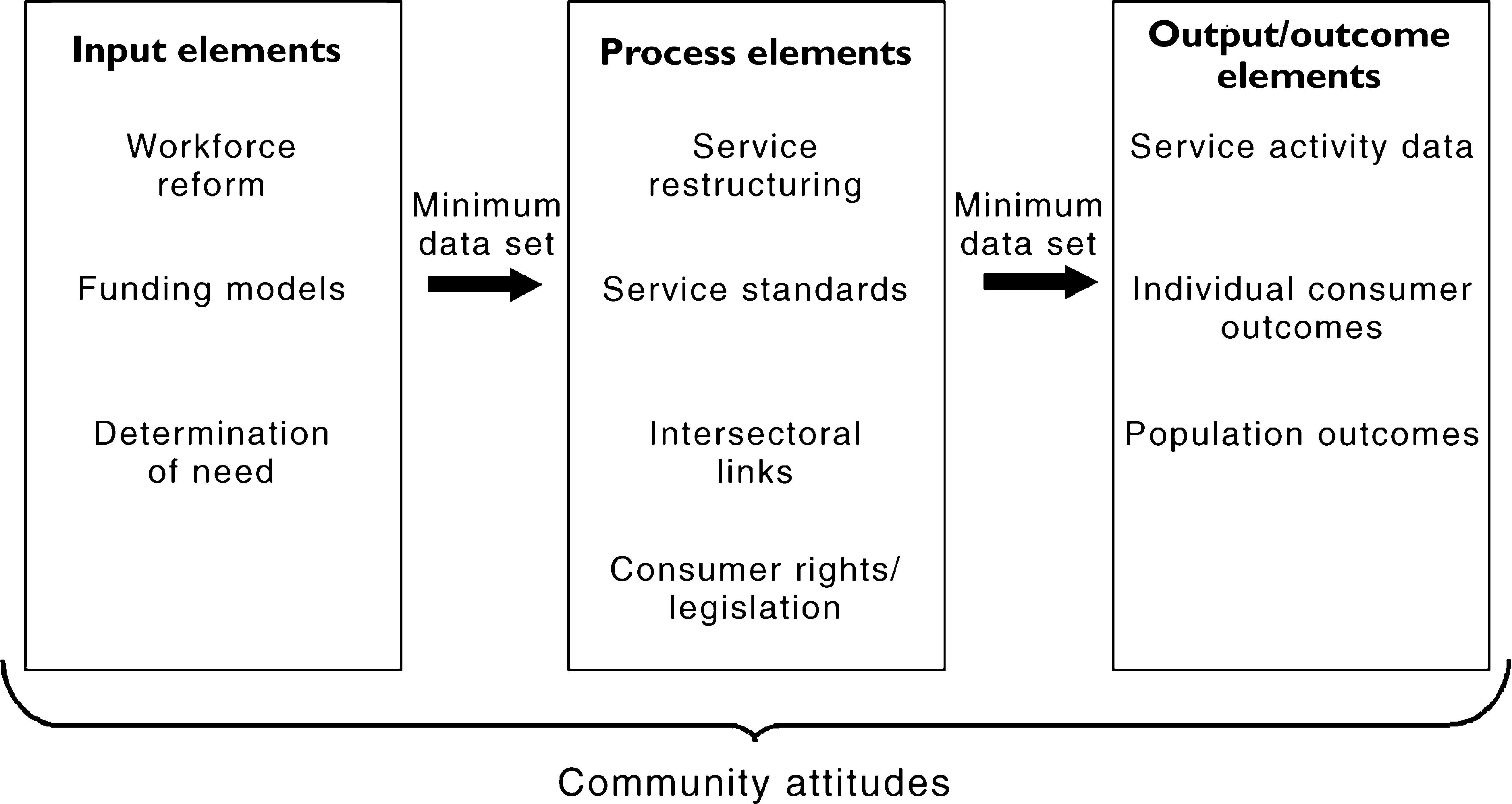
During 1994 I was persuaded by three individuals, Gavin Andrews, Scott Henderson and Wayne Hall, to reconsider this position. Data from other countries cannot be easily extrapolated to Australia and local studies are not able to be reliably generalised to the national level. I also came to the view that Australian national-level data would be more influential at a political level. In December 1994 a meeting of experts was organised by the Commonwealth Mental Health Branch and held at the Australian National University in Canberra to explore the feasibility of such a study. This meeting agreed that three pieces of information were needed: to estimate the prevalence of mental disorders, to determine the disability associated with these disorders and to determine the service utilisation of people with mental disorders.
A three-component survey was designed by an expert team, recommended by the NHMWG and approved by the Commonwealth Minister for Health and Family Services. The several million dollars required to carry it out were provided from the allocation to the Commonwealth Mental Health Branch under the National Mental Health Strategy. Overall management was undertaken by a Survey Management Group, which I chaired and which established a Technical Advisory Committee, chaired by Scott Henderson. Results from each of the components are reported in this issue of the Journal.
The first component of the survey, the National Survey of Mental Health and Wellbeing was carried out by the Australian Bureau of Statistics between May and August 1997 and is comprehensive by any international standard. Its size, 10 600 adults surveyed, is greater than the National Comorbidity Surveys (NCS) [7]. The work of the WHO Training and Reference Centre for the Composite International Diagnostic Interview (CIDI) at the University of New South Wales in developing the computerised survey instrument was groundbreaking. For the first time, Australia has data from a nationally representative sample on the 1-year prevalence of mental disorders, the disability associated with these disorders and what services, if any, people with mental disorders use.
The high rates of comorbidity, especially with alcohol and illicit drugs, confirms clinicians' experience. In light of this, I am even more certain that the administrative separation of mental health and substance-abuse services which exists in our health systems makes little sense, especially to the consumer and their carers. Also, the role of general practitioners as the primary service provider has been confirmed. The Second National Mental Health Plan has as a priority the need to enhance the capacity of primary health care workers in mental health, and this is overdue.
The second component of the survey focused on people with psychotic disorders. This is of particular importance, not least because of their use of psychiatric resources, especially hospital beds. However, because of the relatively low prevalence of this group, they would not have been adequately represented in the adult household survey. It was therefore decided that a separate ‘low-prevalence survey’ would be undertaken to access this population. The report by Jablensky et al. presents the findings of a census of 3800 Australians aged 18–64 years with psychotic disorders attending mental health services in the Australian Capital Territory, Queensland, Victoria and Western Australia [8]. Despite all the effort that has gone into the development of comprehensive area-based services, the report showed that many of these people are still marginalised and experiencing considerable disability. A substantial number do not get the care they need from a range of health and social services, and my high hopes for the inter-sectoral links element of the National Strategy [9] have not yet been realised. This area must continue to be addressed in the Second Plan.
Determining the prevalence of mental disorders in children and adolescents requires a different methodology and a third study was commissioned through the University of Adelaide. Sawyer et al., using a household sample, studied 4500 children aged 4–17 years and the findings presented in their report are crucial for this relatively neglected population [10]. As the Second National Mental Health Plan has a much greater focus on children and youth, and emphasises prevention and early intervention, planning based on this data will be essential for the Plan's success.
Designing and carrying out all three components had problems. Difficulties with instrument design and use, inclusion and exclusion criteria and sampling frames were just a few of the challenges. In both the general adult and the child and adolescent surveys, problems were encountered between those who designed the surveys and those who carried them out. Ensuring confidentiality of respondents in the general adult component meant some cells containing information were collapsed with resultant loss of specific information. The members of the Technical Advisory Group deserve considerable credit for steering a path through what, at times, seemed like an impassable minefield.
The studies are not just academic exercises. Estimating prevalence, disability and service utilisation is important. Both prevalence (or incidence) and disability are crucial for estimating disease burden. Using a common construct for burden which quantifies the disease and injury burden caused by both mortality and non-fatal health outcome, such as the disability adjusted life-year (DALY) [11], we can compare the impact of mental disorders with those of other health conditions. This is essential in the battle for health resource allocation. The DALY cannot be calculated without information on disease occurrence and disability weights. Work in Australia [12] and internationally [13] has demonstrated the considerable importance of mental disorders when this approach is taken over mortality data alone.
However, knowing that the burden is high is only going half-way. We need to know the most cost-effective ways to reduce this burden. There is substantial evidence that most of the commonly used mental health interventions are efficacious, that is, they work better than placebo in randomised, controlled trials [14]. A recent review by Shah and Jenkins [15] analysed 114 cost-effectiveness studies and 14 cost-benefit studies of specific mental health interventions and modes of service delivery. Despite the difficulties with design and analysis, these type of studies have helped refine the interventions which can produce the best outcomes at lowest cost. However, the vast majority compared one psychiatric intervention or mode of service delivery with another, and provided limited information on the cost and health gain of interventions for mental disorders compared with other health conditions. Very little work has been done comparing cost and outcome in a common dimension, such as QALYs or DALYs, for interventions with mental disorders and other common health conditions. The limited work which has been done, however, suggests that interventions for mental disorders, such as schizophrenia and bipolar disorder, can result in equivalent or more savings in terms of DALYs averted than can interventions for conditions such as diabetes, cancer and coronary heart disease [16]. More such studies must be done.
The findings of the surveys in the area of service utilisation will assist the Commonwealth, state and territory governments and the private sector in the planning, delivery and funding of services. Knowing more about demographic variables, comorbidity, the perception of health status and attitudes which determine health-seeking behaviour will allow unmet needs to be more clearly defined and addressed. However, the prevalence rates for disorders found in the household surveys are so high that no government or health insurance fund could possibly consider allocating resources to the level necessary to treat all people meeting the survey criteria for a disorder. We need disaggregation and refinement of the data and further research to know when criteria becomes disease, when need becomes demand, who recovers spontaneously, who should be provided with services and whether these services should be primary health care or specialist services.
Despite their comprehensive scope, the national surveys have gaps. Indigenous people were not specifically catered for and we still know too little about their mental health needs and how to address them. People from non-English-speaking backgrounds were not well represented in the surveys. There has also been concern also that older people were under-represented in the adult survey. Ways of addressing these short-comings must be found. Nevertheless, I believe the Australian mental health surveys are one of the outstanding achievements of our National Mental Health Strategy. They are a credit to those with the wisdom to see the need for them and the perseverance to carry them out. They have provided an evidence-based platform for improvements in the mental health of the Australian people.