
Abstract
The term ‘policy’ seems to engender a particularly negative connotation in the minds of many clinicians. This is, in part, understandable. The term is used to describe things such as government action, government programmes and/or the political process and this does not help with clarity. Most clinicians have also been in receipt of policy decisions that have made their work harder, not easier. A reasonable working definition, at least for the purposes of this paper, is: ‘public policy is deciding at any time and place what objectives and substantive measures should be chosen in order to deal with a particular problem, issue or innovation’.[1] Essentially, this means what action governments take to respond to an identified problem and, in this article, I am limitingmy discussion to government policy.
A review of the public policy and health policy literature identifies the contextual issues within which policy development takes place, the factors that shape the content and impede or facilitate implementation.2–8 These can be drawn together into a five-part policy cycle (Figure 1),[9] which can be applied to mental health policy. Like all models, this cycle is not always followed to the letter. However, all the components can be found in the policy process and understanding the cycle will assist psychiatrists and other mental health professionals to participate in, and exert greater influence on, the policy process.
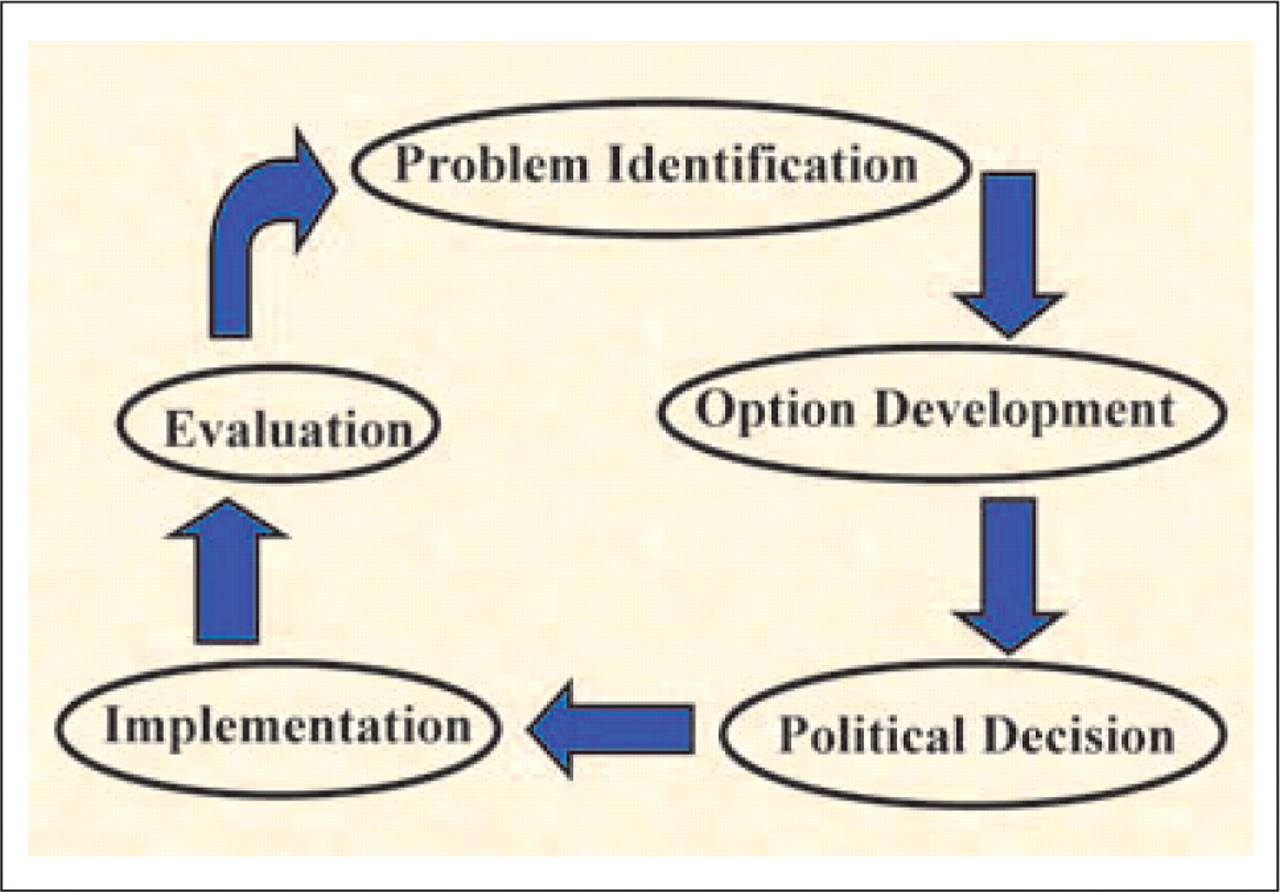
Policy cycle.
PROBLEM IDENTIFICATION
For there to be a policy, there must first be a real or perceived problem for the policy to address. The identification of this problem occurs within a larger social, cultural, historical and political environment. The problems that clinicians think are the ones that need addressing in mental health are not necessarily those that government think are big. The fact that 60% of people who have a mental disorder do not receive treatment[10] might not be a big problem for a busy psychiatrist in clinical practice. However, governments take a different view about people who do not, or cannot, access health care.
Among themany issues impacting onmental health and the treatment of people with mental illness, how does one or more of these issues become identified as needing government attention? Roberts et al. highlight two mechanisms that determine what issue receives selective attention.[9] First, cultural norms and social attitudes provide a set of filters that selectively focus on or divert public attention from issues. If a particular matter is devalued or stigmatized, it can have attention diverted away. This was the case with the quality of care, and abuses inflicted on patients, in psychiatric hospitals during much of the last century. The extension of human rights to encompass mentally ill individuals legitimized action to address the problems in these hospitals. The resultant deinstitutionalization is now facing a backlash as the societal focus has shifted from patient abuse and neglect in institutions to community safety and the ‘right’ to treatment for mental illness. A parallel changing of norms and attitudes underpins the fluctuations in the threshold for involuntary detention in our Mental Health Acts.
The second mechanism relates to the role of ‘issue entrepreneurs’. Roberts et al. describe these individuals or groups as activists who take up particular issues, as they emerge from the filters, to highlight and promote them as a problem needing attention. The entrepreneurs may be politicians or interest groups within the community and their motives vary. Some act on the basis of a conviction about the need to improve a particular area and these individuals or groups often have a stake in that area. A coalition with such convictions, including the Australian National Association for Mental Health and the Royal Australian and New Zealand College of Psychiatrists (RANZCP), acted as issue entrepreneurs between 1984 and 1989 to build the momentum for the National Mental Health Strategy.[11]
The motives of politicians are usually a mixture of genuine interest and party and/or electoral politics. The balance between these motives is often not clear to others who are involved and this can create misunderstanding and disappointment. The willingness of politicians to become involved in particular issues can be influenced by the electoral cycle, with a need to placate activists and minimize adverse publicity in an election year. The different roles of politicians, their staff and public servants are important to understand. Although it is expected that the public service implements the policies of the elected government, most governments are not elected with a detailed mental health policy. Even when mental health is part of a political party's health policy statement, there is usually little detail and much room for interpretation. The bureaucracy does most of this interpretation, has the corporate history about government programmes, can facilitate or impede implementation and generally holds the keys to making the machinery of government work.
Additional complexity arises with our federated system of government. Agreement on a national mental health policy requires, at a minimum, its endorsement by the Commonwealth and all State and Territory governments. All jurisdictions need to accept that mental health is important enough for national policy attention, even before the debate about policy content starts. Issues such as this can become caught up in competition between the Commonwealth and State/Territory governments, which may have nothing to do with mental health but may reflect political rivalry, especially when different political parties hold government in different jurisdictions. Alternatively, it can reflect the longstanding Commonwealth/State power struggle for influence in the health system. Data can be important in forging political allegiances across governments, across government departments and making the case for action. Prior to the adoption of the National Mental Health Policy, the Commonwealth considered mental health to be the responsibility of State and Territory governments and was not supportive of a national policy. A critical piece of research helped change this. A report prepared in 1988 for the Commonwealth by Peter Eisen and Kevin Wolfenden demonstrated that Commonwealth expenditure for people with mental illness was far more than the total cost of all State mental health expenditure. This was confirmed by the National Health Strategy, which showed that the extent of the Commonwealth expenditure on people with mental illness was $2.58bn in 1991/92 (e.g. on sickness benefits, pensions, Medicare benefits and Pharmaceutical benefits).[12] The combined expenditure of the public mental health services run by States and Territories was only $871m in that year; mental health was not only a State and Territory responsibility.
The data went further and highlighted the inconsistencies in the existing policy frameworks. The Commonwealth spent $1.45bn in 1991/92 on income security for people with mental illness and psychiatric disability, but had historically excluded them from the programmes designed to decrease dependence on welfare payments and help disabled people back into the workforce (e.g. in the Commonwealth Rehabilitation Service). Studies such as this became tools for the issue entrepreneurs and helped establish the need for a national approach to mental health in which the Commonwealth became a key player in terms of funding and national leadership.
The interaction between the social filters and the efforts of issue entrepreneurs produces fluctuating patterns in the process of problem definition and in this the incentives and behaviour of the media play an important role. The reporting of issues by the media can highlight important problems needing attention or create the perception of a problem where none really exists. The media focus can be captured by scandal and/or personalities, which at its worst is called tabloid journalism. Information is presented, in part, for its entertainment value and there is a herd pattern found among themedia. Competitivemedia outlets feel compelled to cover a story simply because other outlets are doing so, but the interest in the issue can quickly fade. Issue entrepreneurs have to be patient as their issue cycles in and out of public attention and different perspectives on the issue are presented as problems at different times. An example is the media reporting about mentally ill people in the community. In recent years, there has been media coverage about the neglect of, and alternatively the dangerousness of, these individuals.
DEVELOPMENT OF A POLICY OPTION
Once it has been agreed that a problem exists and needs to be addressed, policy makers have to find a way of doing this. Sometimes the option for fixing the problem is predetermined. This occurs when the elected political party has made a commitment to take certain action. However, this is rare and, once elected as the government, solutions to various problems need to be found. How a solution is chosen among a range of options is policy development.
Governments often start by looking at what other jurisdictions or countries have chosen to do in response to similar problems. Alternatively, they may consider the problem in a very generic way. For example, solutions can be sought by considering health as an industry with inputs, process, outputs and outcomes and applying industry solutions to problems of quality, equity and efficiency. Mental health has either been advantaged, or disadvantaged depending on your view, by the lack of outcome measures. In industry, routine outcome measures are considered essential in order to measure efficiency and allow customer feedback and benchmarking. The first National Mental Health Plan identified the need for consumer outcome measures for these purposes and the Second and Third National Mental Health Plans have driven their development and implementation, with an extensivemental health classification and outcomes network now operational (http://www.mhnocc.org). Whether a policy option is being imported from another jurisdiction or from another industry or is developed generically, it is necessary to arrive at a consensus on the option to be chosen. Achieving this consensus requires the relevant stakeholders to consider the possible options and choose from among them. Choosing the stakeholders to consult is important, because any major group excluded from the process will create ill will and potential opposition. It is nearly always better to have all stakeholders involved in the process, even if it is considered that this will result in time-consuming debate and even enmity. Subsequent political support may depend, in large part, on the extent of stakeholder consultation and support for any particular option.
Stakeholder analysis is a recognized methodology used to determine the position of relevant groups and individuals both inside and outside government who are likely to influence the policy choice and the success of its implementation.[13] Stakeholder analysis includes interest group analysis and bureaucratic analysis and has been refined to the extent that software exists to do the analysis.[14]
The opinions of stakeholders and views of the general population (often considered to be expressed through the media) sometimes agree. Where they do not, timely objective data can be particularly useful. Following the 1997 Port Arthur shootings, there were inaccurate media reports concerning Martin Bryant's mental state. The question for the media was whether the problem that caused the tragedy, and therefore needing a policy response, was dangerous mentally ill individuals in the community or the availability of guns. Data have been made publicly available at a Melbourne conference by a New Zealand gun control researcher, Philip Alpers, showing that the majority of mass civil homicides are not committed by persons with known mental illness discharged from hospital and that most perpetrators held a licence for their firearm.[15] Media coverage and government consideration of this data helped successfully turn the debate toward gun control.
The aforementioned example also demonstrates that, overriding stakeholder analysis, is the question of whether an option presented as a policy position is politically feasible. The position of experts in the stakeholder community and politics can clash when the two come to irreconcilable conclusions. The debate about needle exchange programmes is an example.[16] The scientific data supported the use of such programmes but the political view was that they would be unpopular with the electorate. This leads us to consider how the decision is made to adopt a policy, and this decision is political.
POLITICAL DECISION
The environment of political decision-making is complex. Factors such as the relative power of each player in the political landscape, the positions taken by them and the intensity of commitment for or against the policy all come into play. Within the political sphere, these players include not only the Health Minister, but also his or her staff, other key Ministers (especially the Minister for Finance and/or the Treasurer) and their staff and the Premier or Prime Minister and his or her social policy or health policy adviser.[7] Senior government bureaucrats and advisory bodies in each of these departments are often exceptionally influential through the advice they give to the Minister's office. Successfully negotiating a coalition of support from among these players usually involves bargaining and trade-offs. Throughout the process of negotiation, the content of a policy will be modified, because compromise is usually necessary to achieve consensus.
In trying to arrive at a decision about adopting a policy, the politicians and their advisors scan the stakeholder and community landscape to assess the degree of support the policy will have. Determining this is made difficult in health andmental health by levels of complexity. It is necessary to consider the impact of a policy change on other parts of the system because it may be necessary to make multiple changes at the same time in order to achieve the right policy outcome. Failure to do this can undermine the success of good policy decisions in another area. For example, the policy of closing longstay hospital beds during the 1990s was accompanied by another policy to expand community-based mental health services. However, the lack of community-based accommodation for patients discharged from the hospitals, often the responsibility of the Housing Department, seriously undermined the mental health policies.[17]
Another component of this complexity is the concentrated costs, and power, of select groups such as the medical and nursing professions. The potential beneficiaries of a policy, for example consumers, are generally less powerful and less well-organized. The closure of a ward in a psychiatric hospital with the savings going to community-based services is likely to bring amuchmore vigorous response from the staff who are to be affected in the hospital than the potential beneficiaries of the community services. This imbalance can create significant obstacles to having a policy adopted, and national and state consumer advisory groups were promoted under the National Mental Health Strategy in part to help address this imbalance.[18]
To create the necessary support for a policy to be adopted, it can be useful to align it with symbols that are seen as ideologically unchallengeable and which would have widespread community support. Community mental health care was aligned with ‘least restrictive care’. Concepts such as the ‘right’ to treatment and ‘equity’ in access to care were introduced to generate support for the relevant policies.
Sometimes it is also a matter of reframing the explanation around the policy to ensure political adoption. The policy position of allowing patients to be involuntarily detained in private hospitals was initially seen as unsupportable because of the perception that the private sector would profit from patients being treated in hospital against their will. The policy explanation was reframed to state that a person with mental illness, who had chosen and paid for their private health insurance, should be allowed to remain with the psychiatrist (and hospital) of their choice even when (or especially when) their illness was at its worst. With this reframing of the context, the policy became politically acceptable and was adopted. Perceptions of policy reform are matters of values as well as facts. Political decision-making is about emotion as well as data.
POLICY IMPLEMENTATION
Many policies are developed and adopted but not implemented. Government options are actually quite limited and in reality they have only five main levers available.[4], [9], [19] These are: information collection and publication; the financing system that determines what resources are available, where these resources come from and who has access to them; the payment system that determines on what terms these resources are made available to individuals and organizations; the organization of the health system in both the distribution of services and how they respond to consumer demands; and the regulatory system, which imposes a set of constraints on services, for example how providers are trained and recognized, how the medical and pharmaceutical benefit schemes operate and the regulations that cover the private health insurance and private hospital systems.
In Australia, the National Mental Health Policy was adopted in 1992 and has been implemented through three National Mental Health Plans. Successful implementation requires not only an implementation plan but also the support of those professional and community organizations that came together to ensure that the policy was adopted in the first place. In addition, forging new alliances consolidates support and enhances implementation. Such an alignment occurred between governments and the Strategic Planning Group for Private Psychiatric Services, which had been established by the Australian Medical Association and the RANZCP. The private sector had not been involved in the development of the Policy nor the early implementation of the National Mental Health Plan. Likewise the creation of the Mental Health Council of Australia resulted, in part, from the need to have a broad-based nongovernment body working with governments on the implementation of the Second National Mental Health Plan.
Both the Commonwealth and the States and Territories used the financing and payment levers to help drive the implementation of the National Mental Health Policy. For example, the first National Mental Health Plan detailed how the Policy would be implemented and came with $135m over 5 years of specific Commonwealth funding. The provision of this funding through Schedule F of the 1993–1998 Commonwealth/State Medicare Agreements was made on the basis that States and Territories not only implement the Policy but maintain their own financial effort in mental health. This successfully prevented substitution of new Commonwealth funding for State and Territory funding.
The information lever also proved useful. The Commonwealth, States and Territories all agreed under the Medicare Agreements to provide data on their progress in implementing the Policy. The data were drawn from a set of 49 national policy indicators, first collected for the 1992/93 year and published annually or biennially since.[20] These National Mental Health Reports became public benchmarks used by community groups and the media as a form of public accountability (http://www. health.gov.au/internet/wcms/publishing.nsf/Content/ health-pg-mental-pubs.htm).
Policy implementation also requires staying power. During the life of the first National Mental Health Plan, the political party in power in all governments (with the exception of the Northern Territory) changed. However, the policy implementation agenda continued essentially unchanged. In part, this was because substantial public expectation for change had been created and progress toward meeting this was being reported annually. Governments, with some short-lived exceptions, felt obliged to maintain the pace. The other reason for sustained implementation was because the Commonwealth funding for policy implementation was locked into the 5 year Medicare funding agreement. Over time, this led to the perception that the National Mental Health Policy had bipartisan political support; this consolidated the reforms being promoted by the Policy.
The implementation of policy virtually never goes as planned. Flexibility in responding and adapting to emerging issues, which can create barriers and opportunities, are essential. The implementation of the National Mental Health Plan provided a classic example of how an unplanned enhancing of the process can occur. The negotiations on, and drafting of, the National Mental Health Policy commenced in 1989 and concluded with the adoption of the Policy by all Health Ministers in April 1992. The 1992 Federal Budget, with Brian Howe as Health Minister, contained $135m for the implementation of the National Mental Health Plan. Starting in 1991, the Human Rights and Equal Opportunities Commission held an Inquiry into the Rights of Persons with Mental Illness. Commissioner Brian Burdekin released the report in 1993 when there was a new Federal Health Minister, Graeme Richardson.[21] The report identified the same service deficiencies as the National Mental Health Policy and Plan. In the face of extensive adverse media coverage, Senator Richardson announced additional Commonwealth funding, which amounted to a further $134m over the 4 remaining years of the National Plan, effectively doubling the budget for the National Mental Health Strategy.
EVALUATION
If many polices are not implemented, even fewer are evaluated. By the time an evaluation is due to be conducted, most of the government officials originally involved in its development will have departed. During the implementation, organizations that support the policy may have wilted (or grown), and those who oppose it may be stronger. The environment will be different. For an evaluation to have credibility, it must be as transparent and independent as possible. This means finding people to undertake the evaluation who can demonstrate objectivity. It was difficult to find individuals within Australia who had not been part of, or impacted upon by, the National Mental Health Strategy, so individuals from outside the country were recruited to help with the early evaluations.[22], [23] This also provided an international perspective on the strengths and weaknesses of the policy and its implementation. With the availability of higher quality independent data, it has become possible to have the evaluation done by representatives of the key stakeholders.[24]
The results of the evaluation should be used to revise the policy (Figure 1). In Australian mental heath reform, the policy has not been revised. Rather, successive 5 year plans have been implemented, each attempting to build on the successes and deficiencies of the early plan. For example, the evaluation of the first Plan identified that areas such as prevention, early intervention and primary health care were neglected. These were then incorporated into the Second Plan.
In revising policy or developing successive implementation plans, it is important to resist the temptation to neglect those areas that have been successful and focus primarily on areas that have been less well addressed. In Australia, there has been criticism that we did this with the Second Plan, neglecting the unfinished agenda of the first Plan.23–25 Creating the perception that structural service reform and enhancement was not a priority compared to mental health promotion and illness prevention allowed the momentum to fall away and resultant provider and community backlash has occurred. In broadening the scope of policy implementation, it is important to ensure that scarce resources remain focused on key areas where the best outcomes can be achieved. If we spread our effort and resources too widely, effectiveness will be diluted, with a loss of credibility for the Policy.
CONCLUSION
Policy development, adoption, implementation and evaluation are often seen as political and bureaucratic exercises out of the reach and interest of clinicians. However, all clinicians are stakeholders and those in leadership positions must actively engage in the policy process. It is important that the perspectives of clinical leaders be brought to the process so decisions are made more on the basis of relevance and less on the basis of political expediency and ideology. In doing this, it is necessary for clinical information to be communicated in a way that can be assimilated by individuals unfamiliar with the technical detail. It is often necessary to reframe the information or reduce it to what may seem overly simplistic or inexact.
Mental health professionals have an advantage in the policy arena because they are trained in systems thinking. They can understand the context within which policy is framed, as well as the resources needed, the interrelated components of provision and the outcomes that need to be achieved.[26] However, they must be prepared to enter an arena where they are not automatically given a status, which some professionals see as their birthright and others see as not only unfamiliar but disturbingly irrational.