
Abstract
The locus of care for the mentally ill has alternated over the centuries from institutional-to community-focused care. In Western countries prior to the 1950s, an emphasis was placed on institutional care, beginning with Parish workhouses and ‘madhouses’ to larger, state-run asylums. During the 1950s, the process of deinstitutionalization commenced in the context of broader social change of the post-war period, public outrage over the standards of institutional care, the advent of effective pharmacotherapy and legislative changes, including the development of community health-care facilities and subsidized private health care. Approximately 75–85% of institutional beds were then closed over a 20 year period across Britain, North America and Australia, and the burden of care was transferred to community settings. The closure of long-term and rehabilitation beds has necessitated the development of alternative models of care for the severely mentally ill in the community. The most established of these was pioneered in Madison, Wisconsin in the late 1970s and is termed ‘assertive community treatment’ (ACT).[1]
The aim of ACT is the ongoing care and rehabilitation of severely mentally ill patients in community settings by a mobile, multidisciplinary team of mental health workers. The essential characteristics of ACT have been defined as:(i) low caseloads of 8–12 patients per worker; (ii) an integrated multidisciplinary team; (iii) no greater than 20% part-time staff; (iv) 24 h availability;(v) team autonomy; and (vi) part-time psychiatrist in-put.[2] In the original study, Stein and Test reported readmission rates of only 6% in the first year compared with 58% in a control group not receiving ACT.[1] Other significant benefits included reduced unemployment, increased social contact, increased patient satisfaction and improved self-esteem. In rraddition, a cost–benefit analysis showed a cost saving of nearly $US400 per patient per year for the ACT group.[3] Subsequent controlled trials of ACT have reported inconsistent findings. Marks et al. reported reductions in duration but not the number of readmissions in an inner London sample randomized to either home-based care or standard care following presentation for emergency hospital admission.[4] In the same year, Muijen et al. reported no differences in readmission rate, hospital stay or symptomatic ratings of illness in patients referred on discharge from a mental hos-pital.[5] The PriSM Psychosis study in the UK reported a reduction of inpatient care and costs in an intensive care community setting with added advantages of improved quality of life and improvements in social networks.[6] In contrast, Burns et al. in the UK700 study found no clear benefits on the measures of cost, clinical outcome or cost-effectiveness in 708 patients randomized to either intensive or standard case management over a 2year pe-riod.[7] However, a review of both the PRiSM and UK700 studies found that the intensive case management arms failed to meet fidelity criteria for ACT.[8]
The first Australian study of ACT conducted by Hambridge and Rosen followed the Madison model closely.[9] Case management was provided by a multidisciplinary team with low staff turnover, small caseloads, 24 h access and individual case management of patients. Significant decreases in the number of patients readmitted, number of readmissions and duration of readmissions were reported. In addition, there were improvements in psychosocial functioning, and psychotic symptoms remained stable despite mean reductions in antipsychotic medication dosages. In the only randomized trial comparing ACT to standard case management performed in Australia, Issakidis et al. found no reductions in readmissions, mean bed-days or the number of patients readmitted.[10] That study was conducted only over a 12 month period so delayed positive effects of ACT cannot be disregarded.
With the notable exception of Hambridge and Rosen, the studies of ACT in Australia published to date generally have included experimental or newly formed teams.[9] One problem with such research designs is the possibility of model programs contributing to a ‘Hawthorne effect’ through enthusiasm, special status etc.[11] The assessment of ACT in a well-established team under non-experimental conditions could in part counter such bias. For this reason, we decided to use a clinical audit process to investigate the effectiveness of an ACT model in reducing readmission in a severely mentally ill population.
SERVICE DESCRIPTION
The North East Mobile Support and Treatment Service (NEMSTS) operates within the Austin Health Mental Health Clinical Services Unit. It is a community-based psychiatric rehabilitation service providing home-based treatment and rehabilitation to residents in the northeast area of Melbourne and serves a population of approximately 180 000 people.
The NEMSTS consists of a multidisciplinary team of nine clinicians, including six community psychiatric nurse/case managers, one occupational therapist/case manager, a half-time psychiatric registrar and two sessions of consultant psychiatrist time. The service provides intensive case management in a home-based, outreach format to adult patients aged 18–64 years and has a working caseload of 50 patients. Case manager: patient ratios are approximately 1:7 and case management occurs almost exclusively in the patient's place of residence. The hours of operation are 08.30–21.00 Monday to Friday and 08.30–17.00 on weekends. Emergency care outside these times is provided by the Crisis Assessment and Treatment Team (CATT).
The patient cohort is characterized by severe psychiatric disability and associated psychosocial impairments. The aim of the NEMSTS is to maximize each patient's function, minimize disabilities and prevent relapse. Patients receivea thorough clinical and psychosocialassessment that forms the basis for an individual service plan (ISP). The ISP attempts to address three key target areas for rehabilitation:(i) core symptoms of mental illness; (ii) basic living skills; and (iii) psychosocial impairments of function.
Core symptoms of mental illness. Persistent negative or positive symptoms are addressed following a thorough review of diagnosis and medication compliance, sideeffects and efficacy. An emphasis is placed on minimization of side-effects to enhance compliance, and daily medication supervision of atypical antipsychotic medication with reduced side-effects is offered when required. Inadequate symptomatic control is usually managed with the trials of alternative medication or augmentation of existing medication.
Basic living skills. Fundamental living skills such as personal hygiene, cooking, budgeting and the use of transport are often found to be lacking and contribute signi?cantly to handicap, perceived stigma and social isolation. Clinicians work closely and in a practical manner with patients with the aim of addressing de?ciencies while encouraging independence. For example, case managers may assist a patient with budgeting in a range of ways from clarifying their income and entitlements and establishing banking access to formulating an achievable budget.
Psychosocial impairments. Interventions target the patient's needs in areas such as accommodation, work, relationships, leisure and financial and legal issues. The case managers may provide direct assistance or establish links with relevant agencies such as vocational rehabilitation services, the Ministry of Housing or non-Government organizations (NGOs).
Unique aspects of the NEMSTS function are: (i) the mobility of clinicians; (ii) the provision of a home-based service; and (iii) high staff: patient ratios. In addition, there are extended hours of staff availability. This approach is modelled on the initial report of ACT by Stein and Test and provides the potential for intensive clinician input tailored to each patient's varied and individual needs.
METHODS
A retrospective case audit was performed for all patients registered with the NEMSTS on 11 September 2001. Demographic data were collected from individual case managers who had intimate knowledge of individual patients' functioning. Diagnoses were made according to Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV)[12] on the basis of case reviews by the consultant psychiatrist and psychiatry registrar. The records of previous inpatient admissions to the adult psychiatry services were obtained from a running admissions and discharges summary placed at the beginning of each patient's unit record. Statutory orders were obtained from legal documents in the unit record. Medication status was derived from the medication chart of the Unit Record. Global Assessment of Functioning (GAF) scores, using the GAF scale published in the DSM-IV,[11] were determined by consensus opinion between case mangers and psychiatry staff of the NEMSTS.
In order to assess the effectiveness of the NEMSTS in preventing psychiatric readmission, documented admission dates were determined for two study periods. The baseline was a period of 12 months prior to registration with the NEMSTS following which continuous case management by the NEMSTS was maintained. The second was the 12 month period ending on 11 September 2001 (i.e. the previous 12 months). Admission data for patients who were with the NEMSTS for a period of less than 1 year were not included in the analysis because our clinical experience suggests that at least this amount of time is required for rapport building, medication adjustment, alternative medication trials and the establishment of community linkages. Bed-day costs and annual costs of the NEMSTS and standard Continuing Care Team (outpatient service) were obtained from the Finance Manager of Austin Health's Mental Health Clinical Service Unit and the Manager of the Community Care Service. An assumption was made that, in the absence of the NEMSTS, clinical care of the patients would be undertaken by the Continuing Care case management service and adult inpatient service when admission was required.
The results of this study were processed using SPSS 10.0 processing software. Data were screened for normality using the skewness and kurtosis measures. The results indicate that both number of admissions before and after treatment and length of stay data violated the assumption for normality. To overcome this limitation, all data were analysed using non-parametric statistical methods (Wilcoxon signed ranks test).
RESULTS
Forty-three patients were registered with the NEMSTS on 11 September 2001, including 24 male (56%) and 19 female patients (44%). The mean age was 38 years (range: 23–62 years) and mean illness duration was 15 years (range: 2–36 years). Diagnostic categories consisted of schizophrenia 79% (n = 34), schizoaffective disorder 19% (n = 8) and bipolar affective disorder 2% (n = 1). Six further patients fulfilled a second diagnostic category: one patient had an anxiety disorder and five had an axis II disorder (personality disorder). Three-quarters (n = 33, 77%) of patients had one or more nonpsychiatric comorbidity. Of these, 60% were smokers, 30% abused other substances including alcohol, 37% had a major medical disorder and 6% other comorbidities. Psychosocial functioning was low with a mean GAF score of 46 (range: 25–82). This represents marked disability with patients likely to experience severe ongoing symptoms of mental illness such as frequent suicidal ideation, persistent delusions and hallucinations, and poor social adjustment (e.g. reflected by few or no friends, inability to maintain employment).
The majority of patients were single (n = 29, 68%) while equal numbers of patients were married as were divorced (n = 5, 12%). Of the remaining four patients, two (4.6%) were in a de facto relationship and two were widowed. Nearly half of the patients lived with their family of origin (n = 21, 49%), eight were in supported accommodation (19%), six in government-subsidized housing (14%), six in their own home and two in private-rented accommodation (5%).
Thirteen patients (30%) were under an Administration Order through the State Trustee. No patients were under a Guardianship Order. Nineteen patients (44%) were under a Community Treatment Order of the Victorian Mental Health Act (1986). The majority (n = 38, 88%) of patients were receiving a disability support pension while only four (9%) were employed and one patient was receiving unemployment bene?ts while looking for work. Sixty per cent of patients (n = 26) used public transport, 30% private transport (n = 13) and 9% (n = 4) relied signi?cantly on our team to provide transport. Almost 70% (n = 30) of patients received some form of linkages service. Twenty-two were linked into an NGO, eight were in a vocational rehabilitation programme, six received home help, three patients employed meals-on-wheels and two used other forms of support services.
Time registered with our service varied (Table 1). The majority (n = 18, 41%) had been case managed with the service over a period of 2–4 years while 12 (27%) were case managed for less than 1 year and 10 (23%) for 1–2 years. Only three (7%) were long-term patients of more than 4 years.
Duration of case management with North East Mobile Support & Treatment Service (NEMSTS)
All 43 patients were on one or more psychopharmacological agent. Fourteen patients (33%) were on a depot antipsychotic, three (6.9%) an oral typical antipsychotic, 35 (81%) an oral atypical antipsychotic, 11 (26%) a mood-stabilising agent, six (14%) an antidepressant, 20 (47%) a benzodiazepine, seven (16%) an anticholinergic and nine (21%) other classes of medications (Table 2).
Psychopharmacological treatments in North East Mobile Support & Treatment Service (NEMSTS)
Number and duration of readmissions
The number of admission episodes in the index period for the sample prior to NEMSTS ACT was 24 (mean number of admissions per patient = 0.80, SE = 0.17). This was reduced to 14 (mean number of admissions per patient = 0.47, SE = 0.15) during the second study period. Figure 1 demonstrates the mean number of admissions per patient before and after the implementation of the NEMST. The results indicate that there was a 41.7% decrease in the mean number of admissions after the introduction of the NEMST (W −R(29) = −1.945, p = 0.052).
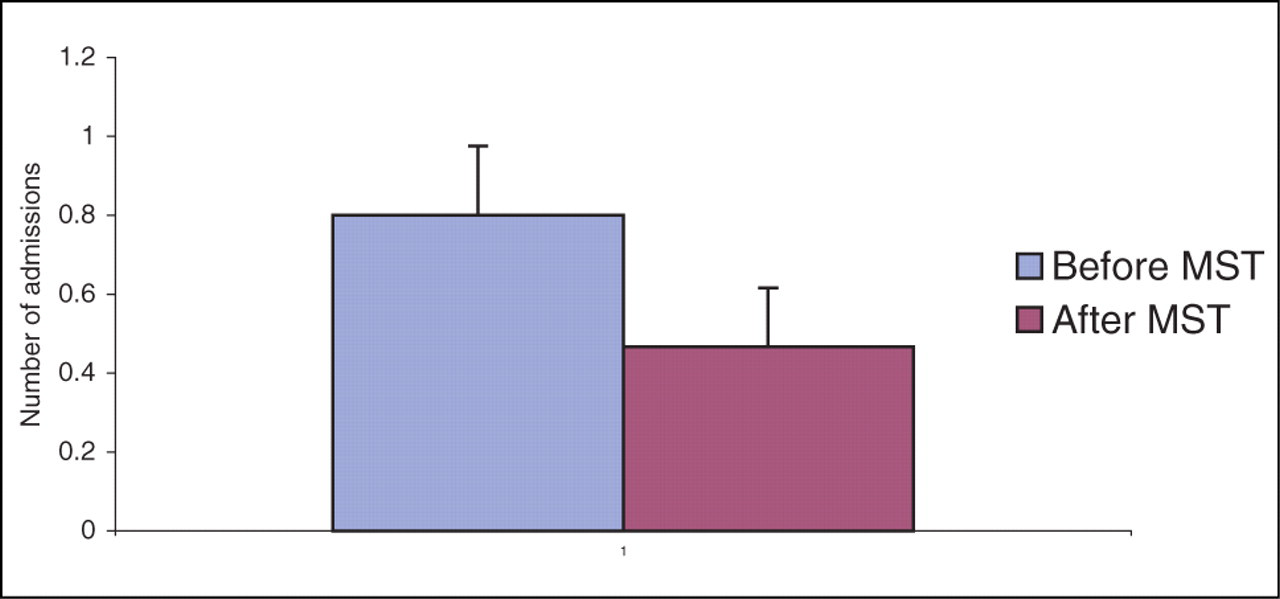
Number of hospital admissions per patient before and after the introduction of North East Mobile Support and Treatment Service (NEMSTS) (mean ± SEM) (p = 0.052).
The duration of readmissions in days reduced from 2128 (mean = 70.9, SE = 20.9) in the first study period to 305 (mean = 10.2, SE = 3.5) during the second study period. Figure 2 shows the mean number of days spent in hospital before and after the implementation of the NEMST. These results indicate that there was an 85% decrease in the mean number of days spent in hospital, taking the average hospital stay from 71 to 10 days after the introduction of the NEMST (W −R(29) = −2.469, p = 0.014).
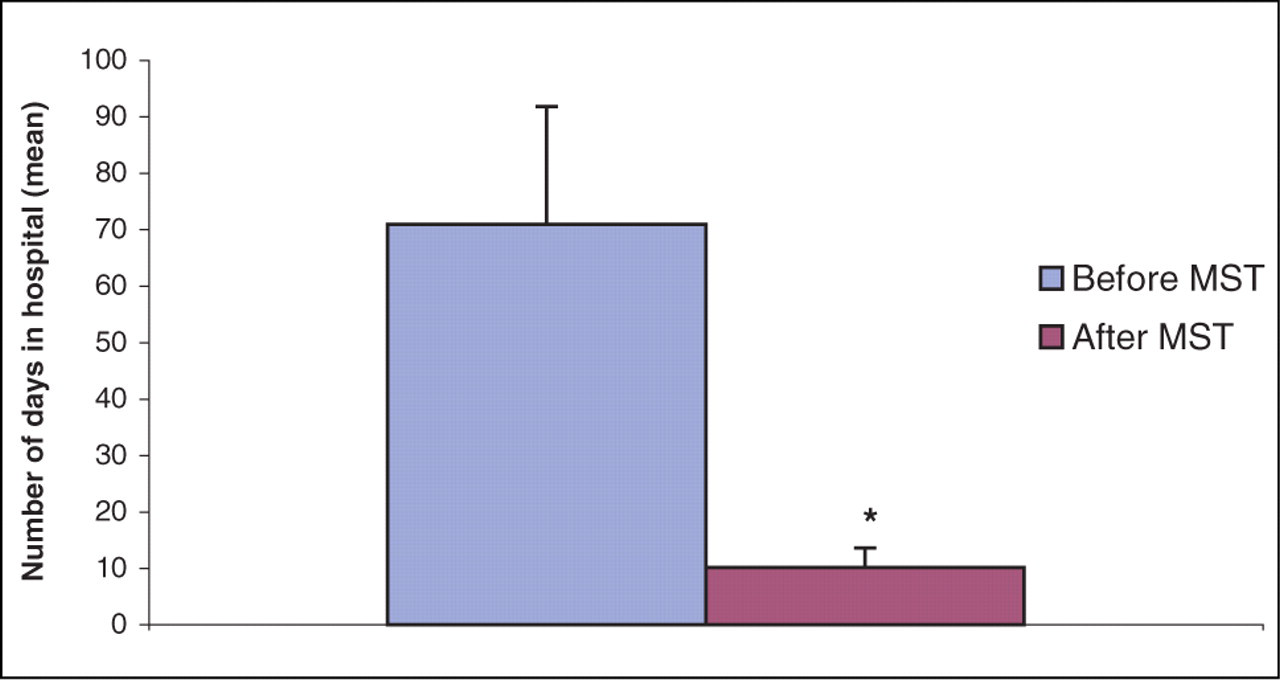
Average number of days spent in hospital before and after the introduction of North East Mobile Support and Treatment Service (NEMSTS) (mean ± SEM) (p = 0.014).
Mental Health Service delivery costs analysis
Thirty-one patients were included in the effectiveness data on the basis of more than 12 months of treatment by NEMSTS. In the 12 months prior to patients' registration with NEMSTS, the total number of admission days was 2128 days. During the 12 month study period, there were only 305 admission days. This represents a reduction of 1823 inpatient bed-days. The cost of a psychiatric bed-day at Austin Health is $452.00. The total cost of outpatient care by the standard outpatient treatment service (CCT) at Austin Health is $218 000 per annum for 50 patients ($1 090 000 for the care of 250 patients, including wages and infrastructure costs). The cost of the NEMSTS per annum (including wages and infrastructurecosts) is $613 000. For the purposes of a limited cost analysis, the total cost of patient care per annum is assumed to consist of the cost of the community treatment service (CCT or NEMSTS) plus the cost of inpatient care. In the 12 months immediately prior to registration with NEMSTS, the cost of standard outpatient care per annum was $218 000 (CCT) plus $961 856 in inpatient psychiatric care ($452.00 2128 bed-days), making a total of $1 179 856. In the 12 month study period, the cost of outpatient care (NEMSTS) per annum was $613 000 plus $137 860 cost of inpatient psychiatric care ($452.00 305 bed-days), making a total of $750 860. The potential cost savings achieved for this patient population treated by the NEMSTS calculated from reduced readmission days in hospital is $428 996 per annum or $13 838 per patient.
DISCUSSION
The Cochrane Database defines effectiveness as ‘the extent to which a specific intervention, when used under ordinary clinical circumstances, does what it is intended to do’. Previous studies of ACT have generally compared a model ACT team, set up for the purposes of conducting a study into ACT, with a standard control. This approach has potential biases, particularly related to the approach a model team makes to ACT. Specifically, model teams are likely to be constructed from those interested in testing the model, team members may possess increased enthusiasm for a novel team role and there may be some investment in producing a positive outcome. These factors may contribute to a Hawthorne-type effect with positively biased results.[11] For this reason, we chose a clinical audit methodology in a well-established team in an attempt to investigate potential stable long-term gains of ACT. At the time of the study, the team had been working together for a period of 5 years and had a relatively stable constitution with five of the seven case managers being members of the original team. The limitations of this method include selection bias and inability to demonstrate a causal link between reduced bed-day readmissions and ACT.
The study describes the ACT of a severely disabled group of patients in a community setting. The predominance of male gender, schizophrenia as the major diagnostic category (79%) and long mean illness duration (15 years) is similar to ?ndings in previous studies and suggests this study targeted a similar sample.[6], [10], [13] The mean GAF score of 45.9 is lower than that reported in some other studies and represents a severely disabled group of patients.[]4,15] The study methodology does not allow for an analysis of the effectiveness of the ACT to make significant improvements in global functioning or symptomatology. Other indices suggesting significant disability include high rates of reliance on disability support pension (88%), low rates of unsupported accommodation (5%), high rates of comorbidity and high reliance on other community linkage services (70%). In particular, the high percentage of our patients living with their family of origin (21%) coupled with a mean age of 38 years raises issues of carer burden and future supports as the patients age.
The main finding of this study is the reduction in psychiatric bed usage associated with the institution of ACT. The mean number of psychiatric readmissions was reduced by 42%. Although this was not statistically significant (p = 0.052), there is a trend towards a significant reduction in readmission. Of greater importance is the statistically significant 85% reduction in bed-day usage following ACT (p = 0.014). This reduction in bed-day usage represents potential cost savings of $428 996 per annum or $13 838 per patient per annum. The study design and the data available are insufficient to perform a detailed cost-effectiveness analysis. It is also not possible to conclude whether these savings were available to be passed on to the service. A lack of significant change in readmission rates has been reported in the majority of previous studies of ACT.[4], [6], [7], [10] However, reductions in total bed-day usage is a more robust finding.[4], [5], [9] It seems that the main effect of ACT is to reduce bed-day usage rather than readmission rates. This may reflect global reductions in chronic psychopathology, early detection of relapse by ACT and/or effective early discharge planning by ACT. The findings of this study are in contrast to those reported by Issakidis et al. who did not find reductions of bed usage following ACT.[10] Our findings are, however, consistent with those of Hambridge and Rosen who demonstrated a 62% reduction in bed-day usage.[9] The study by Issakidis et al. was funded for only 1 year and from our experience it is likely that this period is insufficient to establish the benefits of ACT, including establishment of rapport, community linkages, adequate trials of alternative pharmacological interventions and the stability of accommodation.[10]
It is unclear from this or previous studies as to which aspects of ACT are most associated with reducing bed-day usage. Our clinical experience suggests that the intensive and mobile nature of the service is critical and provides the opportunity to engage patients in their own home (in contrast to the formality and artificiality of a community mental health clinic), the facility to assertively follow up non-attendance and the long-term engagement of a dedicated case manager. We believe the capacity to supervise oral medication, sometimes on a daily basis, has enhanced the capacity to transfer patients to modern atypical antipsychotics available only in oral form, improving compliance and reducing the incidence of extrapyramidal side-effects associated with older typical antipsychotics.
Despite the chronicity of the patient's illness and the potential for dependency of patients on an intensive ACT, we found that only a small percentage (7%) of patients required ACT for prolonged periods of greater than 4 years. This is in contrast to the 50% of patients who had utilized the service for less than 2 years, of whom 27% had utilized the service for less than 1 year. Only very small numbers of patients are re-referred to the NEMSTS. This suggests that improvements made during ACT are sustainable following the institution of less intensive case management. However, few studies have examined functioning following discharge from ACT.
CONCLUSION
Assertivecase management (ACT) has arisen in the context of deinstitutionalization of treatment of the severely mentally ill in Australia and elsewhere. This study examines the effectiveness of ACT in reducing readmissions in a sustainable clinical environment. Assertive community treatment as applied by our service is effective in significantly reducing readmission days. There was a nonsignificant trend in reduction of readmission rates. No conclusions are made about the most effective aspects of the model of ACT presented.
ACKNOWLEDGEMENTS
The authors are grateful to Mr Boyce Felstead and Mr John Brown at Austin Health for their assistance in providing financial data for this study.