
Abstract
Comorbidity of mental disorders is increasingly recognized as a major public health problem, with community studies from Australia, the US and UK finding high levels of comorbid mental disorders in adults[1], [2] and adolescents.[3] Comorbidity is associated with poor treatment and severe illness course.[1], [4] In young people aged between 15 and 24 years, comorbidity is strongly related to disability,[5] reduced academic performance, increased suicidal behaviour, impaired social contact and overall psychological distress.5–7
Comorbidity is also related to help-seeking.[4] Furthermore, the number of concurrent psychiatric disorders, rather than a specific pair of comorbid disorders, is thought to determine the likelihood of an adolescent seeking treatment.[7] This raises the question of whether there are adequate services available to deal with the complexity of comorbidity in a population of young help-seekers.
These factors make comorbidity an important area to consider in terms of identification and development of management strategies. However, although clinicians may be aware of the prevalence of, and issues surrounding, comorbidity in a clinical setting, formal evidence-based guidelines regarding comorbidity in Australia have not been fully developed. The Australianand New Zealand Clinical Practice Guidelines for Specialist Mental Health is based on participants with a single disorder.[8] This paints an unrealistic picture about possible clinical presentations in young people, and reduces the usefulness of the guidelines in their application to cases of comorbidity.
Given the prevalence and negative impact of comorbid psychiatric disorders in adolescents, information is needed about patterns of comorbidity in young people seeking help from mental health services. This will allow evidence-based service planning and treatment guidelines based on a real world picture.
To this end, the present study aimed to identify the pattern of comorbidity present in an Australian adolescent population seeking help for a range of non-psychotic mental health problems at a specialist mental health service.
METHOD
Setting
ORYGEN Youth Health (OYH) is a public mental health service that serves patients aged between 15 and 24years living in the western and north-western regions of Melbourne, Australia. The catchment area covers approximately 1000 000 people and includes some of the most socioeconomically deprived areas of Melbourne. OYH has several specialist intervention programmes, including the Personal Assessment and Crisis Evaluation (PACE) Clinic, the Early Psychosis Prevention and Intervention Centre (EPPIC) and Youthscope. The PACE Clinic manages those at risk of developing psychosis, while EPPIC manages young people with a first episode of psychosis. Youthscope manages young people with non-psychotic mental problems for upto 6months. The present study was set in the Youthscope service. Eligibility for treatment at Youthscope is determined by clinicians and is based largely on the presence of a Diagnostic and Statistical Manual of Mental Disorder, Fourth Edition (DSM-IV) diagnosis of a non-psychotic mental disorder such as depression, anxiety disorders and personality disorders. However, those with uncomplicated primary diagnoses of attention-deficit hyperactivity disorder, conduct disorder (CD) and oppositional defiant disorder (ODD) are not generally accepted for treatment. Referrals to Youthscope come from a variety of services, including general practitioners, schools, and drug and alcohol services. Young people and their families can also self refer. Those not accepted can access limited secondary consultation and are offered suggestions ofalternative services, including Child and Adolescent Mental Health Services.
Sample
Consecutive referrals to Youthscope in the 6month period from April to September 2003 were invited to participate in the research. This included individuals who were referred and accepted into the clinical service and those who were referred and not accepted into the clinical service. Acceptance into the service was decided by clinicians who were independent of the study and was not affected by the young people's decisions about participation in research. Exclusion criteria included: known general medical causefor presentation to OYH, known intellectual disability and an inability to speak English.
Materials and procedure
Psychiatric diagnoses were assessed by using the Structured Clinical Interview for DSM-IV (SCID I/P)[9] and the ODD and CD sections of the Schedule for Affective Disorders and Schizophrenia for School-Aged Children – Present and Lifetime Version (K-SADS-PL).[10] All participants gave signed consent to participate. No informant interviews took place. The interviews were conducted by trained research interviewers.
Data analysis
To examine the pattern of comorbidity within an adolescent help-seeking population, frequency and descriptive analyses were computed.
RESULTS
Two hundred and seven young people consecutively referred to the service were invited to participate in the study, with 151 young people consenting to participate. Of these 151 participants, two people did not complete the diagnostic interview and, therefore, were excluded from further analysis. The final sample comprised 149 young people (58.4% female) with a mean age of 17.7 years (SD = 2.6, range 15–24). This sample included 87 young people who were referred and accepted for treatment and 62 people who were referred and not accepted for treatment. The mean age of refusers (18.7 years, SD 3.0) was significantly higher than for participants (F(1,205) 5.5, p< 0.05). There were no significant gender differences between participants and refusers.
Table 1 shows the prevalence of DSM-IV disorders present in the whole sample at the baseline assessment. The prevalence estimates represent psychopathology in the month before the baseline assessment. Approximately 40% of adolescents seeking help for mental health problems at OYH met criteria for major depressive disorder in the preceding month. Over onequarter of the sample presented with a substance use disorder, while a large proportion of adolescents rated for post-traumatic stress disorder, and social and specific phobia (Table 1).
Prevalence of all DSM-IV axis I disorders in the past mont
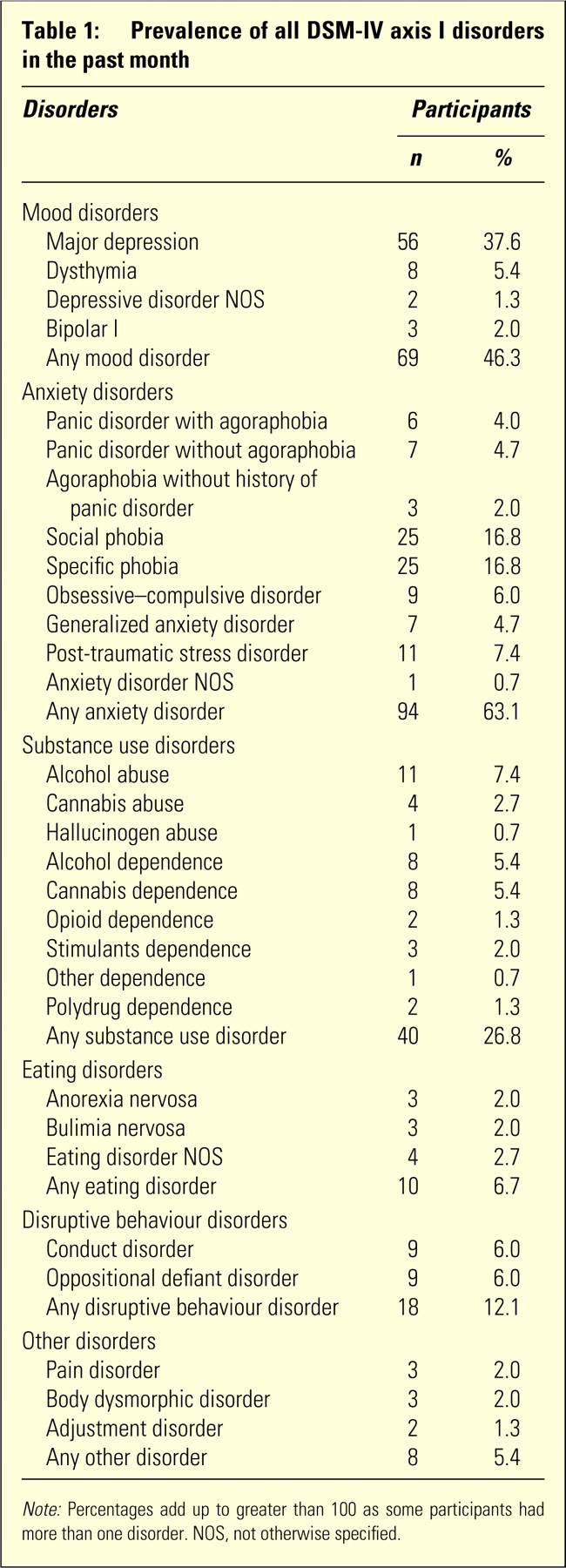
Note: Percentages add up to greater than 100 as some participants had more than one disorder. NOS, not otherwise specified.
Prevalence of all DSM-IV axis I disorders in the past month
Seventy-eight per cent ofthe sample rated for at least one current diagnosis with almost half the sample presenting with two or more disorders. Table 2 shows the number of current diagnoses the sample rated for at the baseline assessment.
Frequency of participants with 0–6 current diagnose
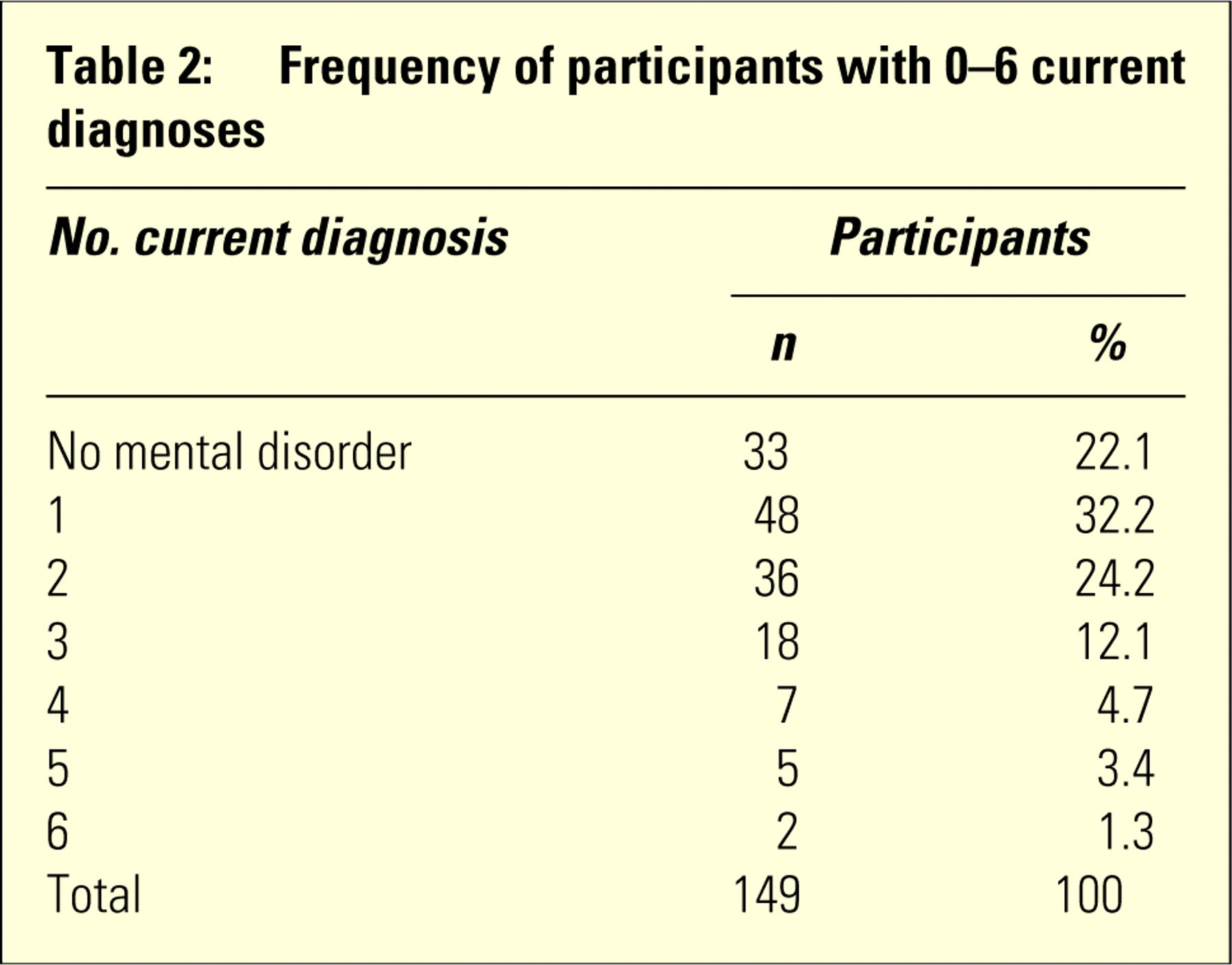
Frequency of participants with 0–6 current diagnoses
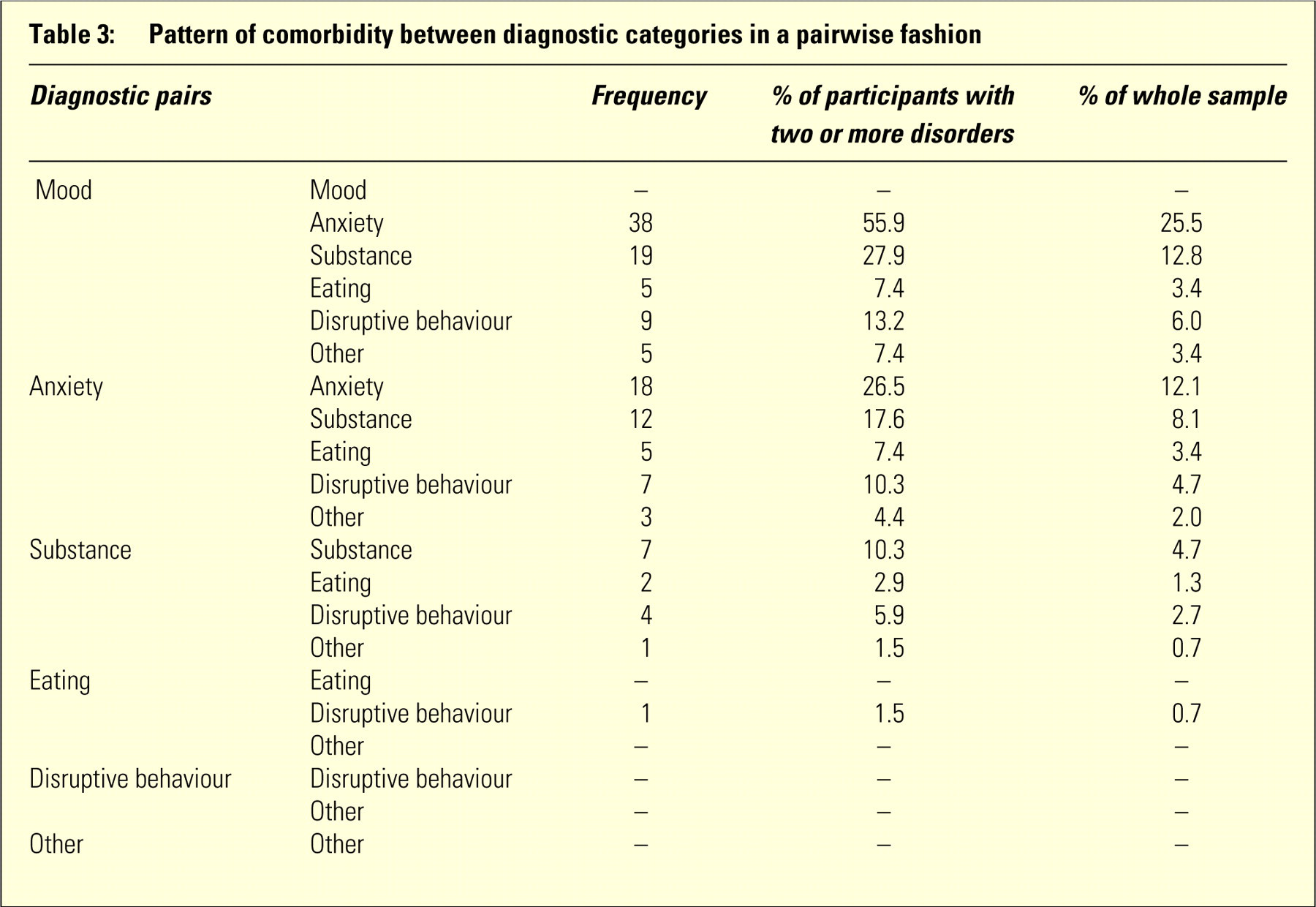
Of those participants with two or more disorders, there were 58 distinct combinations of diagnoses. Given the diversity of diagnoses within the sample, individual disorders were collapsed into diagnostic categories according to DSM-IV and the pattern of comorbidity between categories was examined in a pairwise fashion. The number and percentage of participants presenting with each diagnostic pair are detailed in Table 3.
Pattern of comorbidity between diagnostic categories in a pairwise fashion
Pattern of comorbidity between diagnostic categories in a pairwise fashion
Comorbidity between mood and anxiety disorders was prominent in the sample, as was presentation with more than one anxiety disorder. There was a high rate of comorbidity between substance use disorders and other mental disorders, particularly mood and anxiety disorders. Disruptive behaviour disorders were also found to be comorbid with mood and anxiety disorders.
DISCUSSION
The aim of this study was to identify the pattern of comorbidity present in an Australian help-seeking population. Mood disorders and anxiety disorders were both common in this sample, with major depression the most frequently recorded disorder. Substance use was also prevalent in this group, with alcohol and cannabis use the most common substances used. Our results are consistent with other studies, which found that mood, anxiety and substance use disorders are the most frequent forms of mental disorder in 15–25 year olds.[1],3–5,[7]
Pattern of comorbidity
Substantial comorbidity was found within this sample as almost half of the participants met criteria for two or more diagnoses in the month preceding the assessment. The rate of comorbidity found in the present study is higher than the rate reported in other studies.[3], [4], [11] This may be explained by the fact that other studies have based their findings on community samples or samples of participants receiving clinical care, whereas the present findings are based on young people referred to a mental health service. This high rate of comorbidity is consistent with previous findings where people with comorbid disorders are more likely to seek treatment than people with one disorder.[4]
Comorbidity between mood disorders and anxiety disorders was found to be the most prominent combination of diagnostic categories. This is consistent with other research.[1], [3], [12] A high rate ofcomorbidity was also found between substance use disorders and other mental health disorders, with the most common combination found to be substance use disorders with at least one mood and anxiety disorder.
Implications for clinical services
Patients with comorbid depression and anxiety are commonin clinical practice and present special treatment challenges compared to those with depression or anxiety alone. For example, comorbid depression and anxiety has been found to be associated with more severe symptoms, a more chronic course and increased suicide risk.[12] These challenges are acknowledged in clinical practice and the most recent Australian clinical guidelines state that the most effective method of treating comorbid depression and anxiety is by treating the disorders simultaneously. An integrated treatment approach to any set of comorbid disorders is thought to be preferable than treating each disorder separately (either sequentially or in parallel bydifferent services).[13] Unfortunately, to date the same philosophy is not applied to comorbidity between substance use and other mental disorders.
Comorbidity between substance use disorders and other mental disorders has been well documented by previous studies and is highlighted by the present findings. However, in Australia, unlike the UK or New Zealand, two separate systems of care are in place to manage these disorders.[14] In Australian clinical practice, the treatment of substance use disorders is often the responsibility of drug and alcohol services, while all other mental disorders are managed by specialist mental health services, with little integration between the two systems. Indeed, the current Australian and New Zealand clinical guidelines state that substance use should be treated first, before treating depression.[15] It should be noted that successful treatment of a substance use disorder may be hindered if, for example, the substances are used to relieve the symptoms of depression. Alternatively, substance use may contribute to the onset of, or maintenance of, depression. Therefore, if the depression is treated without treating the substance use, one of the potential contributors to the depression continues. It thus makes sense to treat the disorders simultaneously. This issue has been discussed recently at the government level,[13] but integration between these services has not been implemented at a general service level.[14]
Some limitations of the study must be acknowledged. The sample size is small. Although it did capture the majority of those referred to Youthscope in the 6month data collection phase, no diagnostic data are available for those who did not consent to the study. Therefore, a selection bias may be operating. Also, because the study was set in a specialized service, generalizations to the whole community cannot be made. Despite these shortcomings, valuable information can be gained. In particular, the results suggest that integration between treatment for substance use disorders and treatment for other mental disorders is well overdue, and needs to be addressed at all levels, from government policy to the clinical frontline, to offer adequate care to young people experiencing these problems.