
Abstract
Psychiatry in Australia is now faced with an array of challenges. Over the last 3 years, community-based reviews of the experiences of consumers, carers and families have highlighted the lack of access to basic assessment or review by a specialist psychiatrist as a major issue. 1 , 2 This issue is not new. The lack of access to private psychiatrists, particularly for those with more severe illness or ongoing disability, was recognized by the National Mental Health Strategy in 1993 as a major barrier to service development. This precipitated a series of important reviews and recommendations. 3 , 4 Unfortunately, many of the key elements relating to restrictive work practices, inequity and poor distribution of the workforce persist.
The current difficulties are often presented simply as part of a wider crisis regarding access to mental health professionals (e.g. decline in mental health nursing) or seen to reflect other generic issues facing the medical workforce (e.g. impacts of feminization and movements to less full-time services being provided by all doctors). Additionally, the community reviews have also highlighted the lack of access to psychiatrists in the public sector. The decline of public psychiatric services is clearly recognized by the profession. 5 This appears to be having an adverse impact on training experiences and, inevitably, on recruitment into postgraduate training. At the commencement of 2005, only 19 of 41 new training positions were filled in New South Wales, and that state has initiated a widespread review of postgraduate psychiatry training. 6
In this context, a brief reading of the 2004 National Mental Health Report is sobering. 7 The number of Medicare Benefits Schedule (MBS) services provided by specialist psychiatrists has been declining since 1995/96, despite a continuing increase in the total number of providers claiming benefits. In 1995/96 (2002 constant dollar values), psychiatrists received $223 million in rebates for services, but by 2001/02, this figure had fallen to $196 million. 7 In fact, if one calculates the total ‘savings’ to the Federal Government over this period alone, then they are now in excess of $100 million. 7 We have calculated from the accompanying tables that this fall in rebates is accompanied by a 7% fall in the actual number of consultations provided and an almost 50% increase in the out-of-pocket cost of a consultation (Table 1)!
Contrasting Medicare data on service provision, fees charged, MBS benefits paid and out-of-pocket expenses from 1995/96 and 2001/02
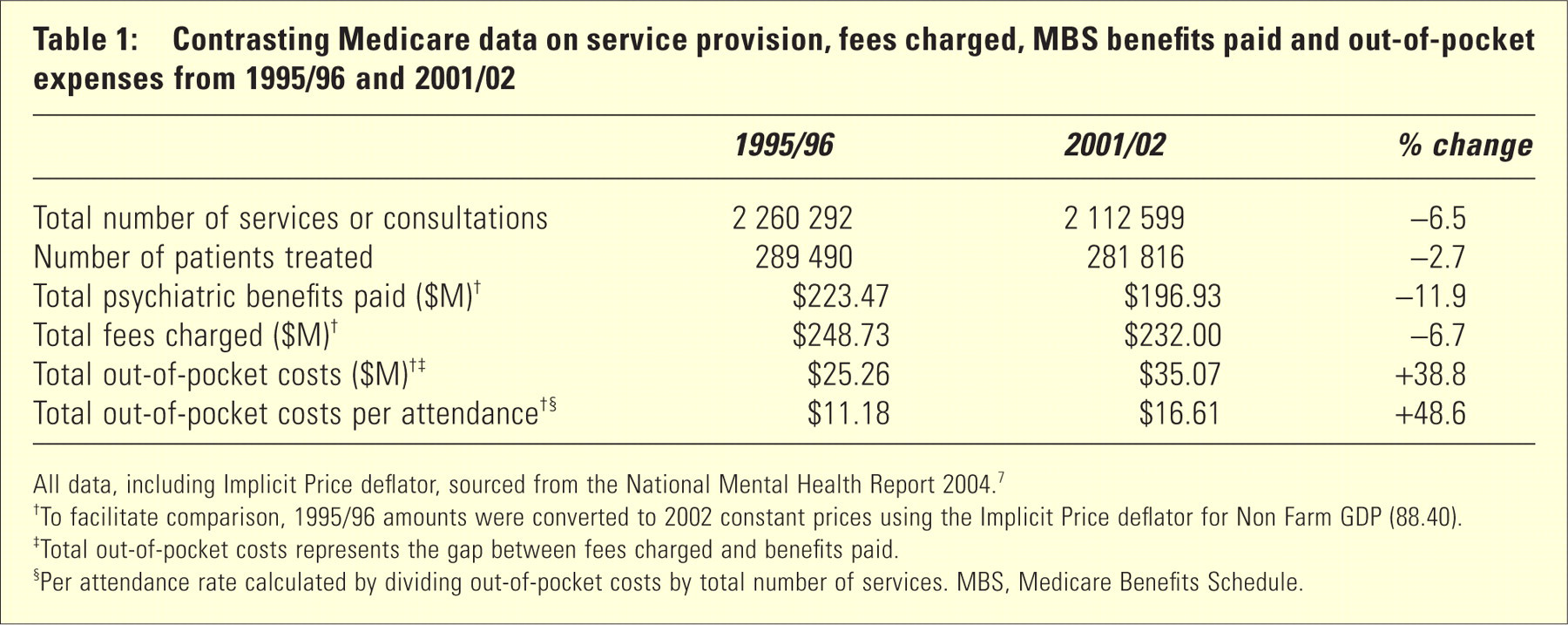
All data, including Implicit Price deflator, sourced from the National Mental Health Report 2004.
†To facilitate comparison, 1995/96 amounts were converted to 2002 constant prices using the Implicit Price deflator for Non Farm GDP (88.40).
‡Total out-of-pocket costs represents the gap between fees charged and benefits paid.
§Per attendance rate calculated by dividing out-of-pocket costs by total number of services. MBS, Medicare Benefits Schedule.
Although real growth in actual psychiatric services is limited, it is currently most evident in the private hospital sector. 7 This has occurred against the background that private psychiatry is, on a geographical basis, one of the most poorly distributed specialist services. 8 This 2002 Commonwealth review highlighted the fact that the disparity in private MBS rebates paid per capita varied from $0.31 in rural northwest Western Australia to $73.79 in inner southeast Melbourne. By contrast, public sector expenditures per capita showed only small gradients by geographical region. The 2004 National Mental Health Report also emphasizes that while Commonwealth expenditures in mental health have increased 128% in the last 9 years (with 66% being due to new pharmaceuticals), state expenditures have only increased 40% or just over 26% on a per capita basis. 7
In total, recurrent mental health spending has increased 65%, which only just outstripped general health increases of 61%. 7 The end result is that there has been no overall change in the relative expenditure on mental health, now reported as 6.4% of the total health spending. 7 It is worth remembering that 27% of all years of life lost to disability in Australia are due to mental health problems and just over 13% of total health burden similarly attributable (or over 15% if one includes death and disability due to suicide or self-inflicted injuries). 9
In essence, psychiatry is rapidly going the way of dentistry in Australia. If the Australian government no longer supports direct enhancement of state-based services and the states do not invest in new services, the public sector will continue to decline. The private sector is increasing (supported preferentially by the private healthcare rebate), but only within a narrow band of hospital-related services. Medical indemnity changes over the last 5 years have substantially increased potential private practice costs, having more marked effects on those in part-time practice, as well as increasing financial risks for those who continue private practice into later-life.
Those who are currently providing private psychiatry services are not only reducing the total number of services they provide but also increasing the cost of each service provided. Those services are now preferentially being provided to those who are most able to meet the additional costs – either directly through increased out-of-pocket expenses or indirectly through the use of private health insurance rebates. Further, much psychiatric practice takes place preferentially outside Medicare-rebated services, particularly in the medico-legal field, but also in response to other third-party insurers.
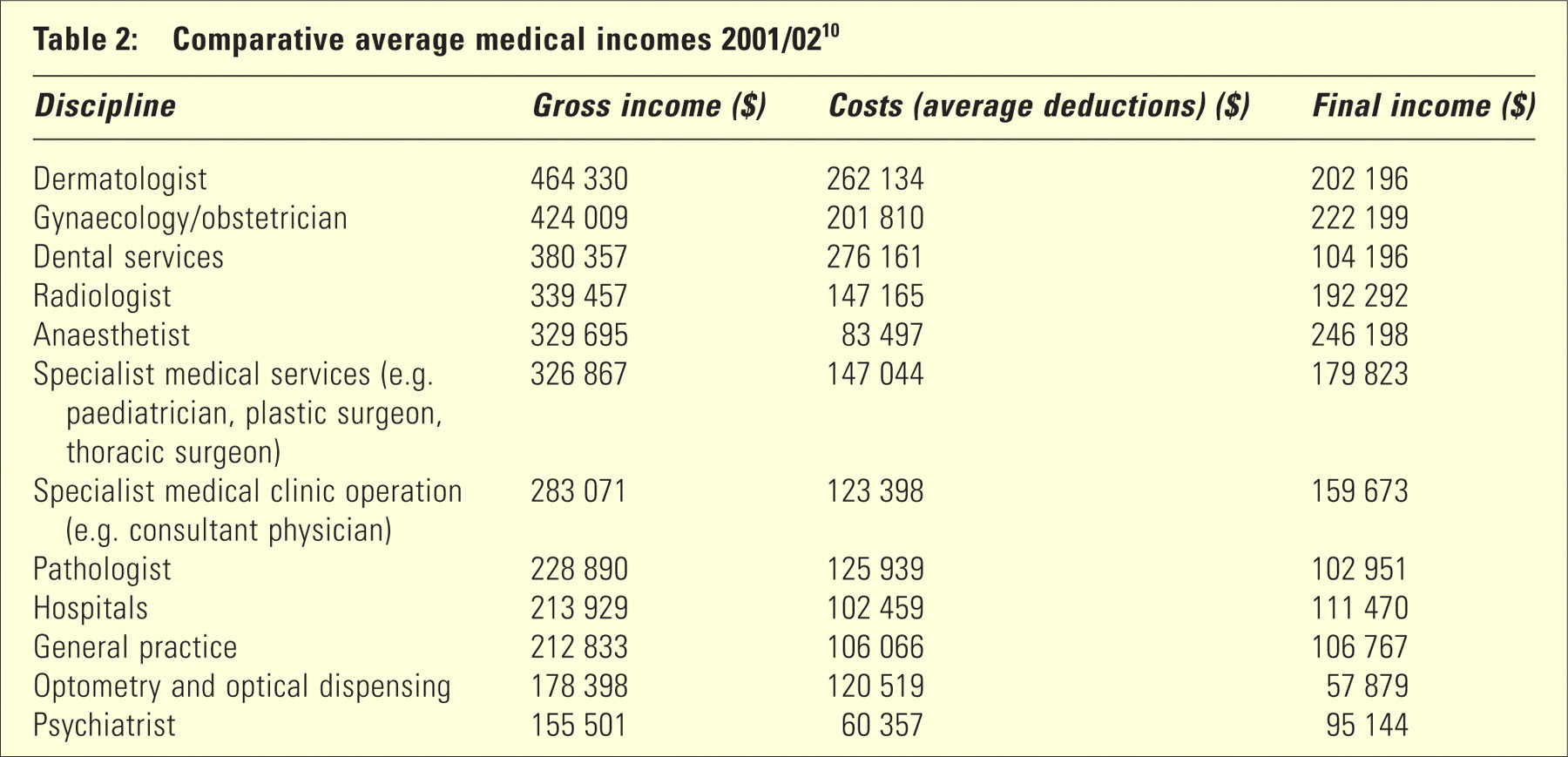
The major difference from dentistry, however, is that it is unlikely that there has been any substantial growth in psychiatrists’ personal incomes during this period. Australian Doctor led on its front page in July 2004 with ‘GPs at bottom of pay scale… with only psychiatrists and optometrists below them’. 10 The Australian Tax Office 2002 data, on which the story was based, compared 12 medical groups in terms of gross income and declared practice costs (Table 2). For declared gross incomes, general practitioners (GPs) finished the tenth ($212 833) and psychiatrists finished the last ($155 501)!
Comparative average medical incomes 2001/02 10
We are now faced with the decline in services provided, decline in the number of provider hours being worked, increasing inequity (financial and geographic) in access to services and considerable public demand for improved access to a wide range of specialist services. It is also possible that the actual number of providers in the future years may decline if current difficulties in filling registrar training posts continue. So, what's to be done? The Royal Australian and New Zealand College of Psychiatrists (RANZCP) has been well aware of the ‘workforce’ issues for some years and has emphasized the need to promote recruitment, improve the quality of training and services, increase partnerships with general practice and other service providers and evaluate new models of practice. 11
While the Australian government has supported various workforce reviews, little has really been achieved in terms of actual reform of the MBS. In fact, its most significant achievement, limitation of rebates to those who attend on more than 50 occasions in 1 year, may simply have contributed to the fall in the number of services and further transfer of costs from the Commonwealth to the consumer. It certainly has not achieved one of its stated goals, namely promoting a move to more consultant-style practice. 12
The shortfall in access to psychiatrists should be overcome by a redistribution of workload, rather than an expansion of the psychiatrist: population ratio. 3 (p. 9)
Perhaps, however, it is really time for a more fundamental shift in the debate. Issues related to psychiatrist work practices, and the extent to which they meet community needs, have been hotly debated since the early 1990s. Although various Australian government consultancies, reports and recommendations have been made, 3 , 4 few real changes have occurred. The most minor of changes, restriction of benefits paid beyond 50 sessions per year and the corresponding introduction of Medicare item 319, created great national debate. Although telepsychiatry items have recently been introduced, they are accompanied by considerable administrative constraints and have only been used sparingly. In May 2005, further small change in a desired direction was introduced with a moderate increase in the rebate (Medicare items 291 and 293) for a first consultation and development of a written management plan with the consumer and their GP.
The most basic problem for reform of rebates is that psychiatrists are largely rewarded for their time, not the actual services they provide or for meeting the needs of the wider population. A shift away from this basic premise may provide not only considerably increased financial rewards but also wider social and population-health benefits. Models for such shifts already exist within both specialist and general practice. For other specialist physicians, rebates reward diagnostic assessment and periodic review as well as specific investigations and procedures. In general practice, a whole range of specific incentives have been introduced at either the practice or individual provider level to meet population health goals (such as increased child immunisation or cervical screening rates) or to improve quality of practice (e.g. diabetes, asthma and mental health care).
The last time that a serious analysis of who was being serviced by psychiatrists was undertaken was over a decade ago. 3 However, the patterns detected then have not significantly changed and we are still working largely with the same pay structure. In that analysis, it was found that 55% of people seen by psychiatrists were seen four times or less per year, and this had remained fairly constant over the period 1985–1992. Patients seen once only comprised 24% of the patient group in 1991/92. For new versus continuing patients, the key findings were that 41% of patients seen in that year were new to the sector, with the balance having treatment histories extending back more than 1 year. Importantly, 27% of the total patient group had been attending private psychiatrists for 5 years or more. Of course, these data were drawn from the period before the introduction of the restriction on benefits to those attending more than 50 times in 1 year.
So, is it possible to design an alternative scheme that emphasizes services, not time, and builds in practicebased incentive systems? In our view, such reform could be relatively straightforward. A simple base figure per scheduled fee (e.g. $100) is assigned for any professional service over 20 minutes but with no upper limit on time (i.e. the reverse of the current system). Multiples of that basic fee are then assigned to reward socially and professionally desirable practices. In this context, the behaviour of a consultant physician rather than primary care provider is prioritized (Table 3).
Fees for psychiatric services and proposed incentives
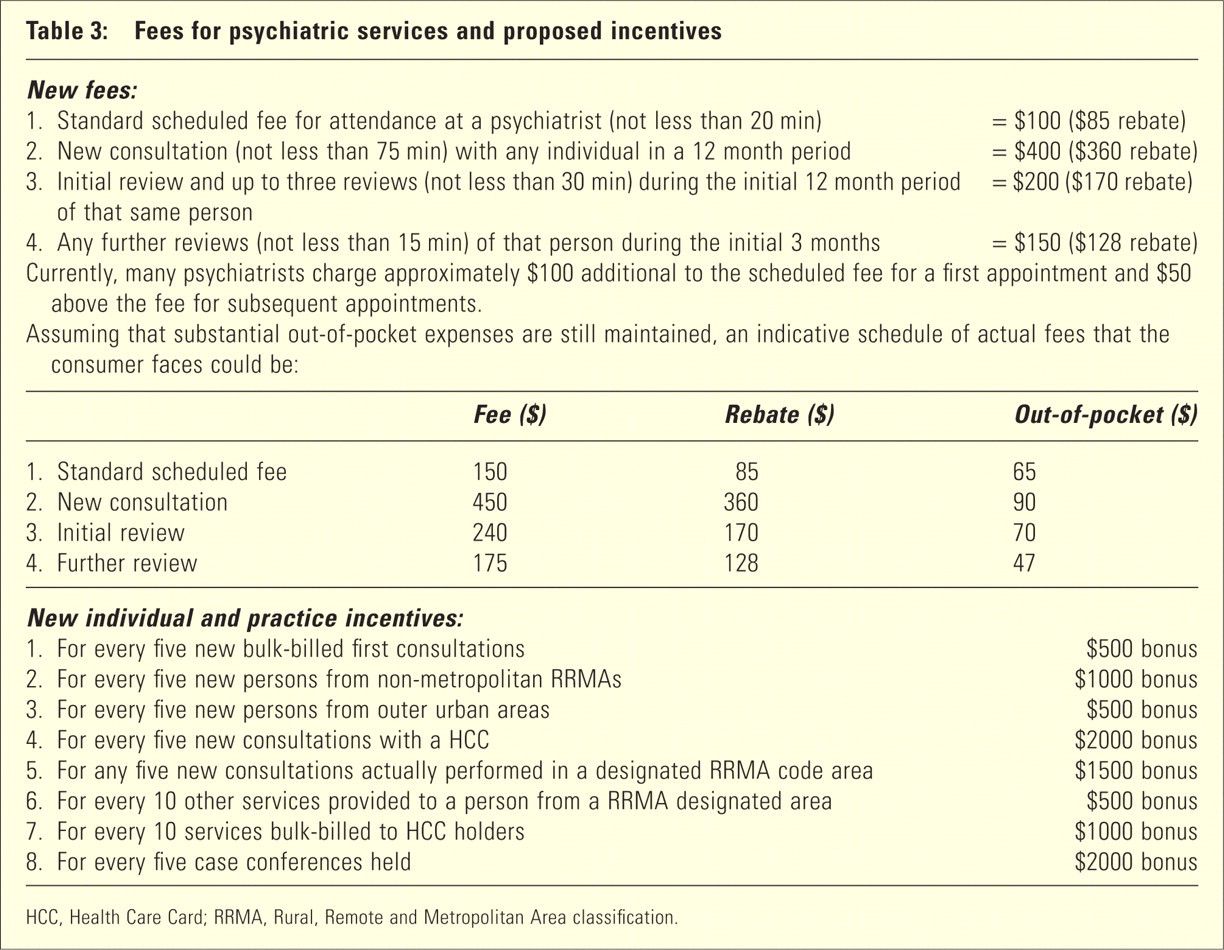
HCC, Health Care Card; RRMA, Rural, Remote and Metropolitan Area classification.
Additional incentives are then added to encourage assessment of persons from geographically disadvantaged areas (notably rural and regional Australia, though this could also include outer suburban areas) or those with limited incomes (e.g. bulk billing of younger persons or those with Health Care Card entitlements). The total fee charged is still left up to the individual practitioner. From a practitioner perspective, the number of hours worked within such a model need not be excessive. The principle is simply using the limited consultant hours available for the maximum benefit of the wider population.
Within such a model, there is a fundamental emphasis on specialized medical and psychological assessment and review rather than provision of ongoing treatment. This leaves open the question as to which health professionals, or health systems, are best placed to provide ongoing treatment. In recent years, community groups have particularly prioritized access to non-pharmacological forms of treat-ment. 1 Even though they are highly cost-effective, 13 currently we have only limited government, private or other third party insurance systems for these interventions. Correspondingly, most consumers, carers and families now rate access to specialized assessment, and non-pharmacological treatments, as highest among their priorities. 1 , 14
Private psychiatrists operate in ‘solo’ practices and so lack the professional and other mental health support needed for difficult patients…. they do not have the economies of scale to employ other mental health staff… (p. 10) 3
Development of key ‘shared care’ models with GPs and other allied health providers, particularly clinical psychologists, as well as with public sector mental health services, is critical. In Australia, the 2001 federal budget initiative, Better Outcomes in Mental Health Care, aimed to address problems for GPs in providing quality primary mental health care to their patients. In line with changing models of service delivery in psychiatry, the Better Outcomes programme has funded the ‘GP-Psych Support’ service, which provides advice to GPs from a psychiatrist within 24 hours via telephone, fax and email. Importantly, less than 2% of the more than 700 cases reviewed in the first 6 months of operation had prior involvement of a psychiatrist and the GPs who used the service reported both an increase in their knowledge about management of mental disorders as well as an increased willingness to manage more complex cases of mental health problems (data presented at the General Prac-tice–Psychiatry Liaison Workshop, RANZCP, Melbourne, January 2005). In the 2005 budget, the Australian government has committed to the ongoing funding and expansion of these shared care systems. 15
Most non-pharmacological treatments can be provided by clinical psychologists and at considerably lower cost structures than when the same services are provided by psychiatrists. Most pharmacological treatments can be provided in association with GPs or relevant state-based mental health services. The model we propose does still prioritize brief interventions by a psychiatrist (less than 3 months), but largely when those services are preferentially provided to persons with low incomes or persons from geographically disadvantaged areas. There is no doubt, however, that this model discourages frequent servicing by a psychiatrist, particularly where such services are continued for prolonged periods (greater than 12 months).
Public mental health services have shown a reluctance to become involved with ‘shared care’ arrangements with private psychiatrists or general practitioners (p. 10) 3
In our model, for 100 hours of practice, a psychiatrist could reasonably expect to bill over $40 000 (Table 4). Practice costs associated with this model may be higher than expected because of the volume of referrals, communication with other professionals and promotion of case-conferencing. However, assuming that practice costs were kept below 50%, practitioner gross revenue would be at least $20 000 or at least $200 per hour. In our view, practitioner revenue below this level will not attract new doctors to our field or encourage existing practitioners to change their current practice structures.
How 100 hours of clinical practice might look
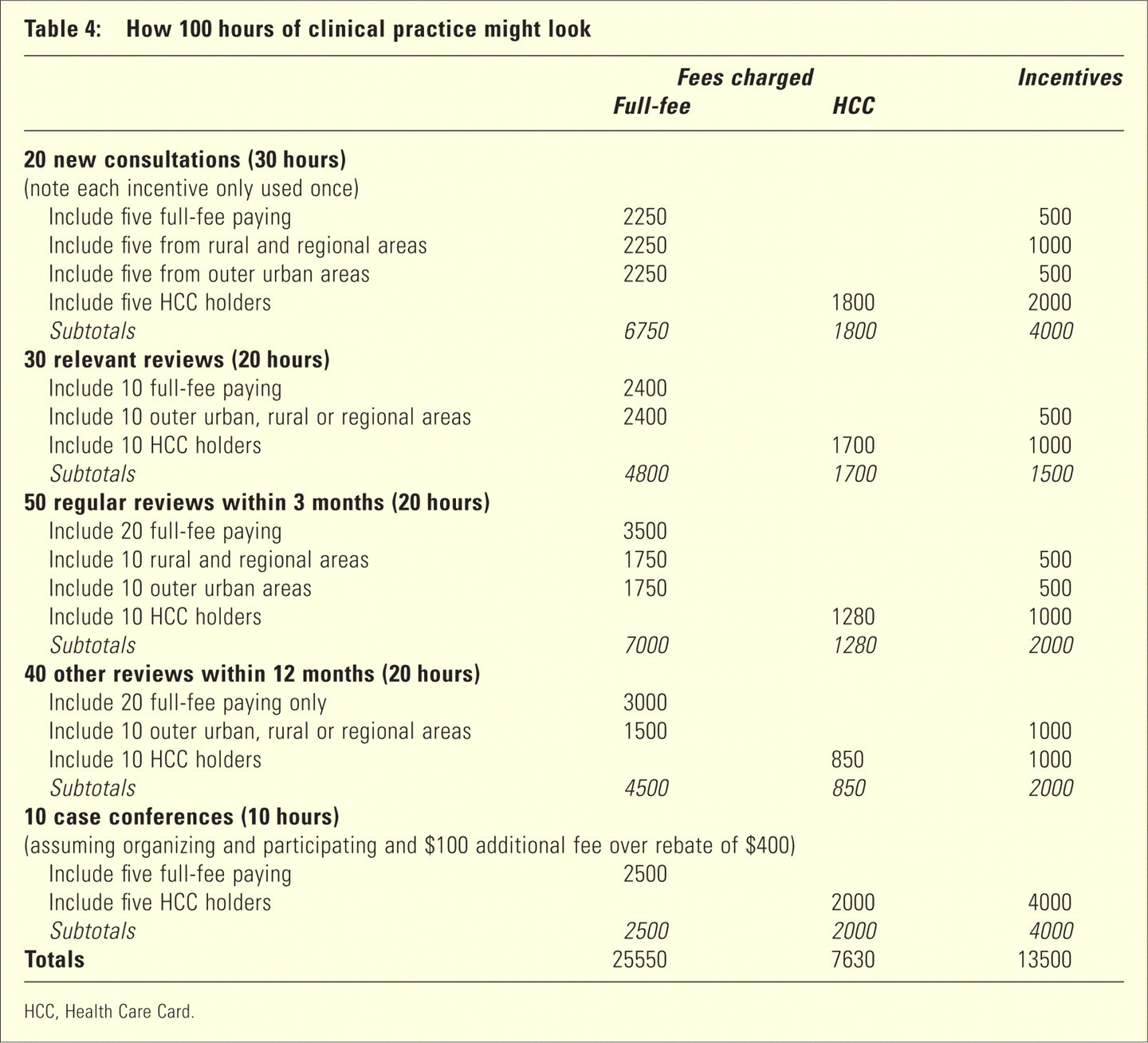
HCC, Health Care Card.
Specific incentives to join the new payment system could also be provided. This has been done successfully with GPs to promote electronic prescribing and uptake of the mental health incentives. Such incentives would assist with the necessary changes in practice structure and communication systems that would underpin these systems of care. A start-up fee of $10 000 may well be appropriate, or $20 000 for an outer urban practice, or $30 000 for a rural or regional practice.
Achieving relative parity between public sector and private sector pay rates is another vexed question. Currently, public health systems are increasingly relying on short-term contract or visiting medical officer staffing arrangements. Generally, these are more financially rewarding than traditional staff specialist arrangements. Given the additional adverse effects of changes in medical indemnity, some of the recent movement back to public sector services may have resulted from a reduction in the traditional pay differences between the sectors. If private practice was now made more attractive again, and there was no significant increase in available providers, there is the risk of exacerbating losses of specialists from the public mental health sector.
The introduction of an alternative funding model does not need to be universal. In fact, it is much more likely to come into being if only a minority of practitioners, or well-organized practices, respond. This would mean that those individual practitioners who wish to persist with their current practice models, or continue their work outside the current Medicare system, would be unaffected.
Many psychiatrists feel that the greatest impedient to the development of such an alternative model is the National Government or related health bureaucracies. Given the declining actual cost of psychiatric services to the Australian government and the increasing pressure to provide better services, government resistance may not be the major source of resistance. The real barriers remain the same as those encountered repeatedly over the last two decades. These are, first, resistance among medical specialists to move away from a simplistic fee for service model (always rewarding more professional services, investigations and minor procedures – note the positioning of dermatology, dental services and radiology in Table 2) and, second, resistance within our profession. Many of our colleagues are extremely reluctant to move from a primary mental health treatment role to a consultant physician model.
Another important alternative to the regular MBS rebate system is for the Commonwealth to contract for those specific service arrangements, as it currently does for other non-medical specialist services under the Better Outcomes in Mental Health Care Program. 15 Such professional services are currently contracted through a third party, namely, Divisions of General Practice. Other aspects, such as the telephone and on-line urgent advice, are contracted directly with suppliers of those services.
Medicare Benefits Schedule reform on its own is very unlikely to result in major changes in service provision in rural and regional Australia, or result in enhanced care to other key groups such as indigenous Australians or young people with psychotic disorders. Here, more innovative solutions need to be explored and may well require experimentation with relevant capitation or ‘managed care’ models. Although such models are commonly criticized by colleagues working within cost-constrained US entities, we do need to consider the ways in which some entities, notably in the not-for-profit sector, have operated such systems.
It is unlikely that we will ever achieve professional consensus in Australia about directions in MBS reform. However, establishment of alternate systems may provide opportunities for genuine experimentation. Additionally, the development and implementation of alternate models would clearly signal our profession's intention to respond to the challenges of increasing inequity, declining workforce participation and lack of response to the needs of the community who finance our work.