
Abstract
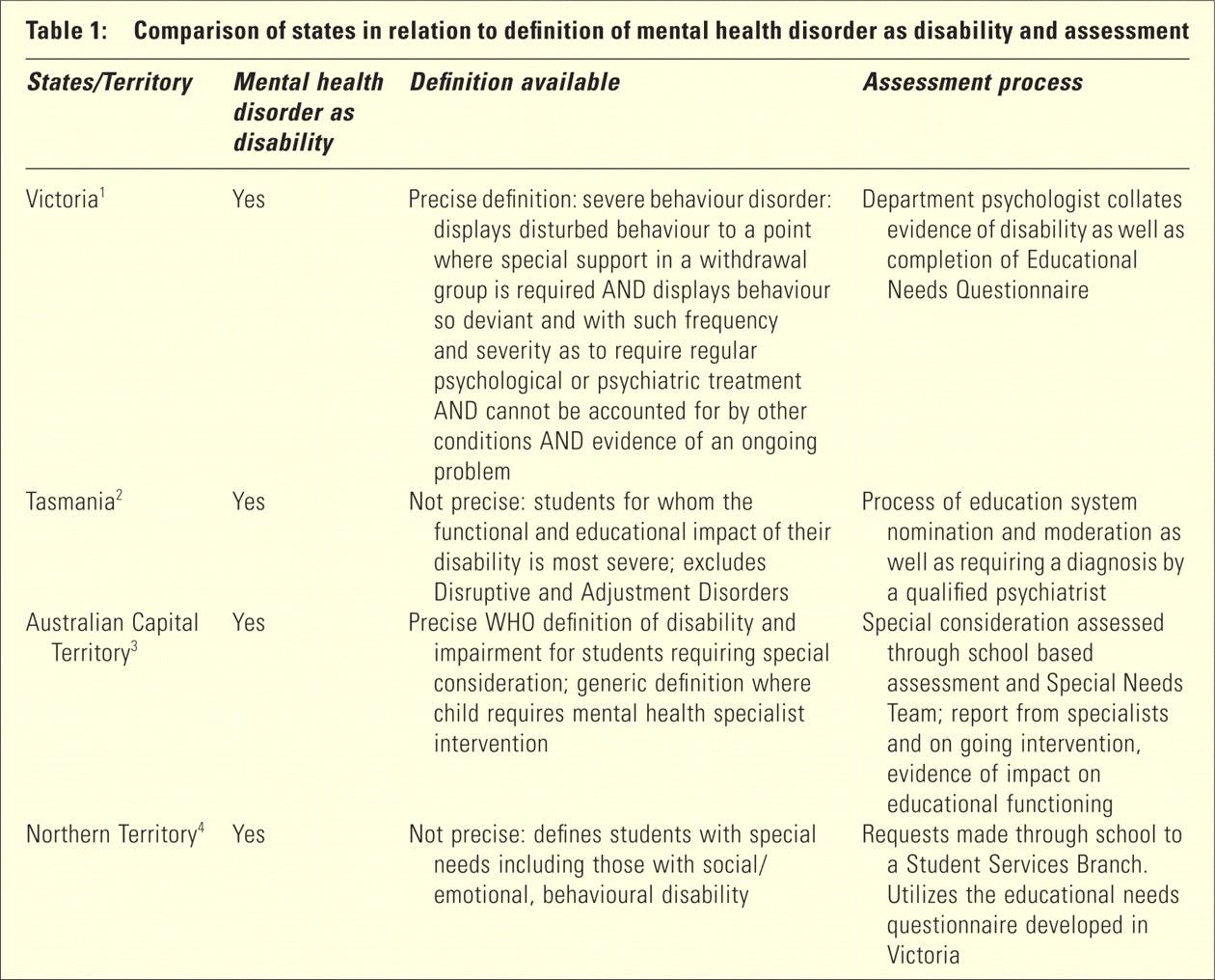
Children and adolescents with mental disorders face confusion and discrimination within Australia's various state education systems in relation to their disability status. The issue is important as the nomination of a disability status to mental disorders can attract extra support and funding for the affected child. There are three problems embedded within this issue. First, there is conceptual confusion over whether mental disorders are disabilities. Only a few education administrations, for example, Victoria, Tasmania, the Australian Capital Territory (ACT) and the Northern Territory consider mental disorders to be disabilities (Table 1). 1 – 5 Second, even in those selected jurisdictions that are supportive of the inclusion of mental disorders within a disability framework, significant variation and inconsistencies exist in how mental disorders are defined. Other inconsistencies are present whereby some selected mental disorders are classified as disabilities to the exclusion of others. Finally, even when mental disorders are recognized as disabilities, complex information gathering processes are used to quantify the amount of assistance offered. Such multifaceted processes can disadvantage and burden some children and families. Each of these problem areas will be considered in turn.
Comparison of states in relation to definition of mental health disorder as disability and assessment
THE DISABILITY ISSUE
The first problem domain involves confusion over whether childhood mental disorders are recognized as disabilities. This is an important and fundamental issue because conceptual failures in this realm have implications for the child's trajectory through the education system. All education systems have policies for children with accepted disabilities such as physical, language, hearing, intellectual and vision problems. It is obvious that children with these problems are disadvantaged, deserve a disability status and need to access extra school supports which aid in the completion of their education. Completion of secondary school education is now recognized as critical in terms of future employment. 6 However, not all States recognize mental disorders as disabilities.
The failure by certain states to recognize childhood mental health disorders as genuine disabilities conflicts with contemporary understanding of childhood mental disorders and their outcomes. The Australian Bureau of Statistics survey of childhood mental health problems 7 found considerable extra difficulties were faced by affected children. Severe mental health problems were common (7%); many of the disorders were co-morbid with other disorders, and affected children have poor self-esteem, increased limitations in peer activities and reside in less cohesive families. The Western Australian Child Health Survey 8 found that students with mental health problems were performing at below age academic competence and were more likely to be absent from, and less attached to, the school. Furthermore, there is evidence that children who do not reach diagnostic criteria are impaired. 9
THE INCONSISTENCY ISSUE
A number of inconsistencies occur both across and within education systems. First, a number of states (e.g. Queensland) recognize Autistic Spectrum Disorder (ASD) as a separate disability. Such recognition is a major inconsistency, as ASD is widely accepted as an umbrella term covering a number of autism related mental disorders described in the Diagnostic Statistical Manual Edition IV. 10 Why one mental disorder is acceptable as a disability and not others is unclear.
A further inconsistency occurs within education systems as to which mental disorders are judged disabilities and those that are not. One state system, Tasmania, 2 accepts some mental disorders as disabilities and not others (e.g. Disruptive Disorders are excluded). This distinction is bizarre as many children who experience chronic antisocial and oppositional behaviour have multiple levels of functional impairments to their psychological capacities. Richters and Cicchetti 11 have detailed the nature and extent of disabilities in children with disruptive disorders. In brief, children experience a host of behavioural difficulties from an early age, which results in significant conflict with family and peers. As well, such children suffer from increased rates of anxiety and depression. Many endure neuropsychological and social cognitive deficits. Excluding such children from the disability status becomes illogical in light of their numerous impairments.
In the four education systems that accept mental disorder as deserving of disability status, significant variation exits in how the problem is conceptualized (Table 1). For example, Victoria has an inclusive generic definition, which focuses on severity of disability. 1 Tasmania has a less precise definition that also emphasizes severity but excludes some disorders. 2 The ACT has the most comprehensive definition adopting the World Health Organization definition of disability. 3 The Northern Territory has a general definition utilizing a disability framework. 4
THE PROBLEM OF ASSESSMENT BURDEN
The third problem involves the variations in the assessment processes required by the different education systems (Table 1). For example, in Tasmania, 2 a complex process of information gathering and diagnosis by a psychiatrist is required. However, it is likely that some of the social and behavioural characteristics of the clients themselves could make such procedures problematic. Children with mental disorders are likely to reside in multi-problem families with a range of financial, motivational and psycho-social troubles. Families may feel burdened by attendance at appointments, the costs of travel and the demands of a specialist assessment. Further complicating the situation, the identified patient may be poorly motivated, have reduced communication skills and resist being interviewed by a specialist. Some of the most disadvantaged adolescent students may wish to attend school but be openly reluctant to participate in an assessment process. In addition, there are problems such as a lack of appropriate specialists in the public or private systems, the need to collate extensive information, and the time demands needed to provide evidence of disability status. All these problems conspire to make for an information gathering process poorly matched to client needs.
In summary, three problems are present. Some education systems do not accept the disability status of mental disorders at all or exclude a few disorders and accept others. Across educational systems, there is definitional disarray with respect to a common understanding of mental disorders. Finally, significant obstacles exist for children with complex disorders in being able to access an adequate assessment. Each of these problems in turn reinforces a discriminatory approach to children with mental disorders.
DISCRIMINATION AGAINST CHILDREN WITH MENTAL DISORDERS
The authors recognize that many education systems offer help (e.g. behaviour management services) to children with mental problems or disorders. However, the provision of such services does not solve the problem. The failure of various education systems to recognize some or all mental disorders as disabilities means the affected children will often be deprived of appropriate assistance equivalent to other disabled groups. This state of affairs amounts to a case of discrimination.
The nature of the above discrimination is defined by the Disability Discrimination Act 1992 12 under Section 6, Indirect Disability Discrimination: ‘The discriminator requires the aggrieved person to comply with a requirement or condition: (i) with which a substantially higher proportion of persons without the disability comply or are able to comply; and (ii) which is not reasonable having regard to the circumstances of the case; and (iii) with which the aggrieved person does not or is not able to comply’. The complex assortment of emotional, behavioural, cognitive and social deficits present in mental disorders makes compliance with ordinary educational processes problematic if not impossible. The authors would argue that the case for discrimination is clear.
The picture is further compounded by the fact that 70% of Australian children between 0–14 years of age live in States where mental disorders are not recognized as disabilities within education systems. 13 In addition, as an average of 350 000 people move between State and Territories each year, many families are likely to be facing the distressing scenario of negotiating conflicting education systems criteria. 14
SOLUTIONS
A consistent disability framework and advocacy
A common approach to the recognition of childhood mental disorders as disabilities could occur if there was an agreed Australia-wide conceptual foundation. One example comes from the Diagnostic Statistical Manual Edition-IV 10 definition of mental disorder. It highlights four elements: personal distress (e.g. a painful symptom); disability (e.g. impairment in one or more important areas of functioning); a significantly increased risk of suffering death, pain, disability; and the loss of freedom. A comprehensive definition of disability is also available from the recent publication of the Draft Disability Standards for Education 2004 which aims to be incorporated into the National Disability Discrimination Act 1992. 15 This definition includes criteria such as: total or partial loss of the person's bodily or mental functions; a disorder or malfunction that results in the person learning differently from a person without the disorder or malfunction; a disorder, illness or disease that affects a person's thought processes, perception of reality, emotions or judgement or that results in disturbed behaviour. Both approaches have much in common and could provide the foundation for a consensus understanding. The Commonwealth Government is seeking to amend the Disability Discrimination Act (1992) to incorporate new, clear standards, making it unlawful for an educational authority to discriminate against a person on the ground of the person's disability. 16
A coalition of clients, careers and professionals needs to lobby state, territory and Commonwealth governments to agree on a consistent approach to the classification of mental disorders as disabilities. An example of one such organization is the Australian Infant, Child, Adolescent and Family Mental Health Association. However, the formal adoption of the Disability Discrimination Act amendments may bring this matter to a head even without such advocacy. As well, the coalition needs to ensure that extra Commonwealth funding is allocated to the states and territory education systems so as to absorb the expected increase in demand for services. 17
Flexibility in the assessment process
The assessment process could be made less burdensome to vulnerable students. One possibility is the use of the Achenbach Child Behaviour Checklist, Teacher Report Form and Youth Self Report. 18 These questionnaires are in widespread use in Australia, both in clinical and research settings. All questionnaires provide a score which indicates whether or not the student's level of symptomatology is within the clinical range. The latest version of the Achenbach scales uses either a computerized or hand-scoring system to convert symptom scores into diagnostic categories which equate to DSM diagnostic groups. 19 For some students, this may provide an alternative method of establishing a diagnosis.
CONCLUSIONS
Significant reform is required to rectify discrimination towards the large numbers of children disadvantaged due to the failure of some education systems in recognizing mental disorders as disabilities. Concerted advocacy or amendments to the Disability Discrimination Act may force movement towards a common definitional stance inclusive of all mental disorders. Other reforms will be required to assessment processes to accommodate children and families unable to access such approaches.