
Abstract
Borderline personality disorder (BPD) is well recognized as one of the most distressing mental health disorders for patients and as one of the most challenging for mental health clinicians. As such, the first publication in 1991 of a randomized controlled trial (RCT) of the effectiveness of psychosocial treatment was greeted by clinicians with considerable enthusiasm. 1 Being the first RCT published, this 1991 publication represents a landmark in the treatment of people with BPD. Since 1991, there have been 11 RCTs or controlled trials published of effective psychosocial treatment for people with BPD; dialectical behaviour therapy (DBT) has dominated the publications with six RCTs and two other controlled trials published to date. In addition, several uncontrolled pre–post studies of DBT for BPD have also now been published. 2 Dialectical behaviour therapy has been shown to be effective for people with severe forms of BPD including comorbid depressive disorder and substance use. 3 – 5 Further, DBT has been recommended as a specific treatment for BPD by the American Psychiatric Association guidelines. 6 A review of the economic impact of the treatment gave a calculation of DBT saving approximately $US10 000 per patient per year, particularly through the decreased rate of hospitalization. 7
Dialectical behaviour therapy or DBT-orientated treatment is becoming widely used with DBT being implemented now in areas that include substance use disorders, bulimia, forensic settings, attention deficit–hyperactivity disorder (ADHD), depression, family violence, and with suicidal adolescents. 2 , 8 Dialectical behaviour therapy is also being used in inpatient, day patient and crisis settings. 2 It has a strong international infrastructure, 9 including core manuals 3 , 10 and a robust training framework. It can be readily taught and learnt within a reasonable time frame. Research has demonstrated that public service clinicians from diverse backgrounds (nursing, social work, psychiatry, psychology, ‘case workers’) are able to acquire a solid understanding of DBT theory and practice. 11 Dialectical behaviour therapy has been shown to be effective in the USA 1 , 4 and in Europe. 5 , 12 These factors combined to make DBT (or DBT-orientated practice) highly relevant for service providers to consider introducing into routine Australasian public mental health systems. There is one non-peer-reviewed report of DBT implementation in New Zealand that briefly reports on decreased health resource usage but not clinical outcomes. 13 What has been required is research exploring whether DBT could be effectively implemented in Australasia, and more specifically in routine Australasian public mental health services.
Dialectical behaviour therapy is a cognitive–behavioural therapy enhanced by the addition of mindfulness practice and acceptance-based philosophy and practice. Dialectics refers to the synthesis of different perspectives, with the most important synthesis in DBT being that of patient and therapist expectations of patient change alongside patient and therapist acceptance of the patient as they are in the present. Standard DBT comprises individual therapy (60–90 minutes per week), group skills training (120–150 minutes per week; two trainers, 6–9 patients), crisis telephone coaching and a consultation meeting for therapists (60–90 minutes per week). Individual therapy with an individual DBT therapist focuses on motivation, commitment and functional behavioural analyses (problem and solution analysis) of target behaviours that the patient records using a daily diary card. Common targets for behaviour analysis are selfharm and substance use behaviours and urges to suicide, self-harm or use substances. Group skills training teaches patients mindfulness, distress tolerance, emotion regulation and interpersonal effectiveness skills; this is education-focused, assisting patients’ strengthening and generalization of existing skills and the learning of new skills. Patients are encouraged to make use of telephone skills coaching to support their maximal use of skills at times of crisis.
METHOD
Sample
Patients were recruited from those already being treated within the service in a treatment as usual manner. Patients completed the International Personality Disorder Examination (IPDE), 14 a semistructured diagnostic interview conducted by one of the authors (JB). Eleven patients with an IPDE diagnosis of BPD entered the DBT trial. One patient's DBT therapist left the service 1 month after treatment commenced, leaving 10 patients who are the subject of this report. All 10 patients were female, whose age ranged from 21 to 53 years (mean, 34.3; median, 34). Nine patients identified themselves as New Zealand Euro-pean/Pakeha and one as Maori/European. Six patients had previously disclosed histories of childhood sexual abuse.
Treatment
The 10 patients were treated in 2001 in two groups of five, in two separate geographical areas, one urban and one rural. In each geographical area, treatment was standard DBT comprising individual therapy (60–90 minutes per week), group skills training (2 hours per week delivered by two trainers), telephone calls and therapist consultation meeting (90 minutes per week). Treatment reviews and supervision took place in the weekly therapist consultation meeting. Rating therapists’ adherence to the model was beyond the scope of the study. Treatment was provided by 10 clinicians comprising three psychologists, two social workers, two drug and alcohol counsellors, one nurse, one psychiatrist and one psychology intern. Medication use continued in a treatment as usual manner and was not recorded for data analysis.
Design
Cultural (Maori) and consumer advisors were involved in the development of the project proposal and approval was obtained from the Waikato Ethics Committee before implementation of the research project. There was no placebo, non-treatment or control group. Patients were referred and assessed for BPD using the IPDE. Patients entering the trial completed the outcome measures pre treatment and post treatment. Using patients as their own controls, pretreatment scores were compared with post-treatment scores by the use of two-tailed independent t-tests. The IPDE, outcome data and post-treatment qualitative interviews were independently administered and collected by one of the authors (JB) who had no role in the delivery of treatment. The qualitative interviews involved the development of themes from patient answers to a standardized set of questions on the different components of DBT treatment (individual therapy, group skills training, telephone consultation) and crisis services.
Data
Demographic data on gender, age and history of childhood sexual abuse were collected at the outset. The Millon Clinical Multiaxial Inventory, 3rd edition (MCMI-III), a self-report rating scale that is well correlated with the DSM-IV, 15 was completed pre treatment and post treatment by all 10 subjects. Patient-rated symptoms were also measured by the Symptom Checklist 90-Revised (SCL-90-R), which was completed pre treatment and post treatment. Because of initial assessment time constraints and the response style of five participants being significantly slower in completing psychometrics, SCL-90-R data could only be obtained at pretreatment for five of the 10 participants. Acute hospital bed usage data were collected for the 1 year period before treatment in the trial and for the 6 month period of the trial. Qualitative interviews were conducted with all 10 participants immediately following the completion of the 6 month treatment.
RESULTS
Rate of retention in treatment
All 10 patients were retained in treatment at the end of the 6 month trial.
MCMI-III
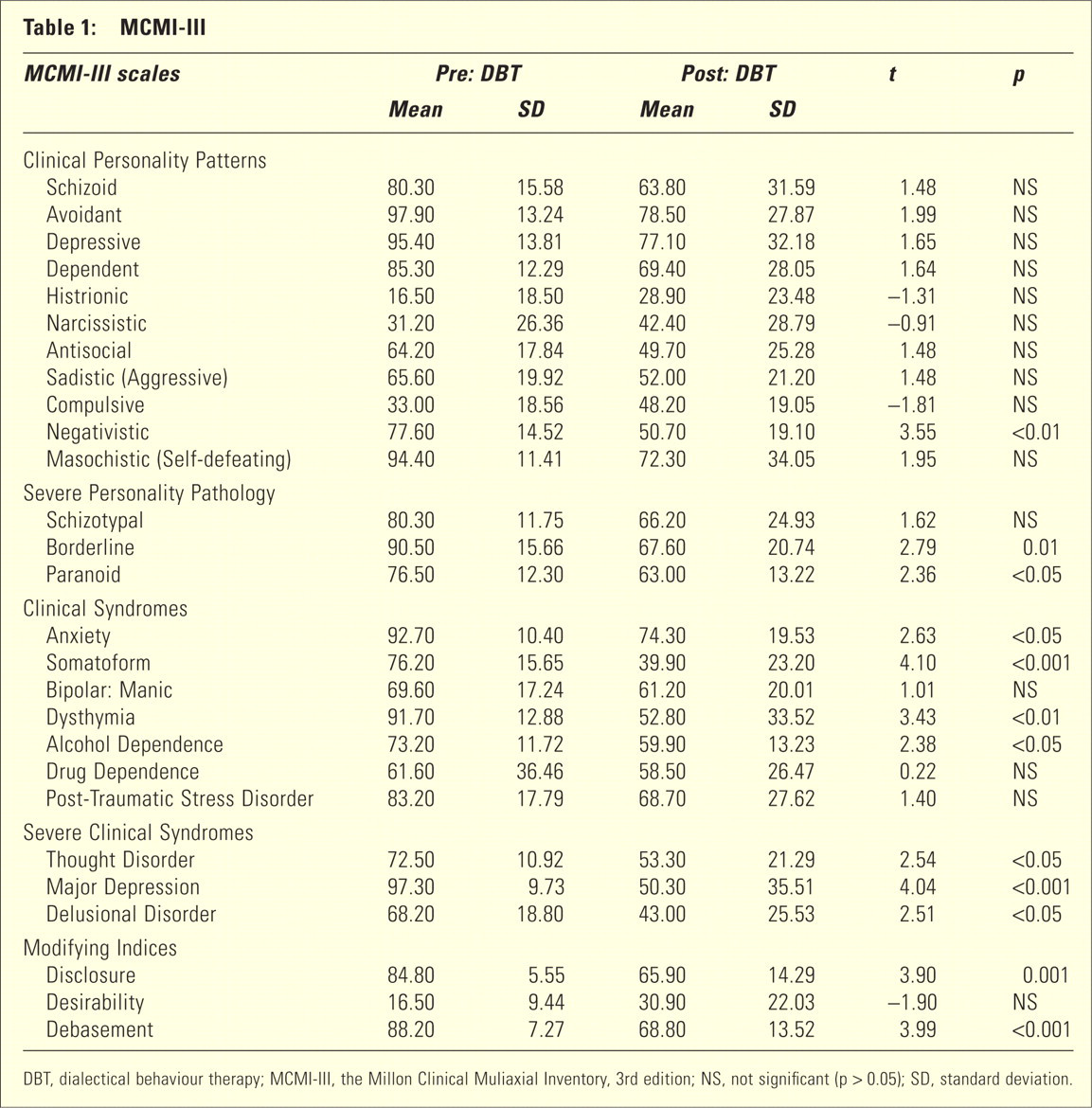
Table 1 outlines the results of the group analysis for the responses of the 10 participants on the MCMI-III before and after their participation in the 6 month DBT programme trial. Statistically significant improvements in functioning were evident on 10 of the 24 scales (p < 0.05 to p < 0.001) including the Negativistic, Borderline, Paranoid, Anxiety, Somatoform Dysthymia and Major Depression scales. The statistically significant group differences evident on the Disclosure and Debasement scales of the Modifying Index are indicative of improved skills in communication distress. 16
MCMI-III
DBT, dialectical behaviour therapy; MCMI-III, the Millon Clinical Muliaxial Inventory, 3rd edition; NS, not significant (p > 0.05); SD, standard deviation.
The MCMI-III categorizes Base Rate (BR) scores according to severity as follows: 16
BR < 85 –indicating the prominence of a syndrome or disorder –‘Severe’ range
BR = 75–85 –indicating the presence of traits or a syndrome –‘Moderate’ range
BR < 75 –not clinically significant –‘Mild’ range
Before their involvement in the DBT programme trial, the group mean scored in the ‘severe’ range on eight (Avoidant, Depressive, Dependent, Masochistic, Borderline, Anxiety, Dysthymia, Major Depression) and in the ‘moderate’ range on a further four (Negativistic, Paranoid, Somatoform, Post-Traumatic Stress Disorder) of the MCMI-III scales. Following the DBT treatment trial, none of the group means for the MCMI-III scales were within the ‘severe’ range and only two of the group mean scales were within the ‘moderate’ range (Avoidant, Depressive), both of which, before the treatment trial, were within the ‘severe’ range.
The pretreatment mean BR score on the MCMI-III Borderline scale was 90.5 (‘severe’ range), improving post-treatment to 67.6 (not clinically significant range). 16 Single-subject analysis of the MCMI-III data revealed improvement in psychological functioning in eight of the 10 participants, while the remaining two participants essentially maintained their status quo.
SCL-90-R 17
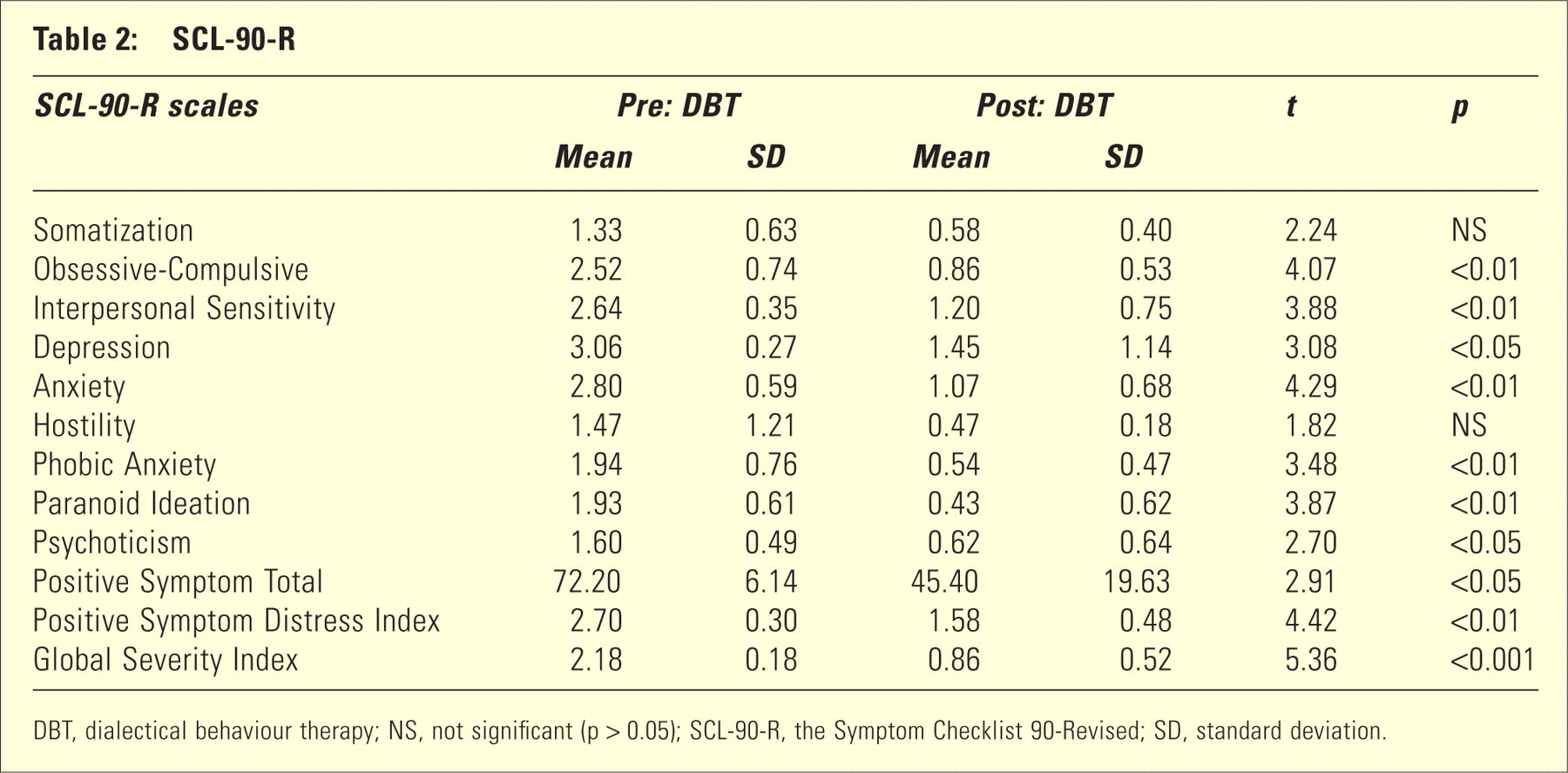
Table 2 displays the pretreatment, post-treatment group analysis for the five patients who completed the pretreatment SCL-90-R. Statistically significant reductions in SCL-90-R t-scores were obtained on the Global Severity Index (GSI; p < 0.001) and 10 of the 12 subscales (p < 0.05 to p < 0.001), representing significantly less psychological distress following the 6 month trial. Individual analysis demonstrated all five patients recording statistically significant reductions on at least 10 of the 12 SCL-90-R scales.
SCL-90-R
DBT, dialectical behaviour therapy; NS, not significant (p > 0.05); SCL-90-R, the Symptom Checklist 90-Revised; SD, standard deviation.
Acute psychiatric inpatient bed days
Acute psychiatric inpatient bed day usage decreased from a mean of 0.57 days per patient per month in the year before DBT treatment to 0.2 days per patient per month during the 6 months of DBT treatment.
Qualitative data
All 10 patients reported significant consumer satisfaction with their experience of the programme. Common themes to emerge during follow-up interviews with participants included comments on the practical utility of the treatment (n = 8), alternative skilful responses learned to deal with target problems (n = 8), achievement of long-term goals (n = 5), development of a sense of responsibility for one's own recovery (n = 3) and hope and happiness (n = 3). When asked about the most effective parts of the programme, some participants mentioned a particular favourite skill (n = 7), while others mentioned the treatment package as a whole (n = 4), the group dimension (n = 3) or the use of diary cards (n = 3).
While no external measure of self-harm behaviour was undertaken for the purpose of this evaluation, four of the seven patients with histories of self-harm and their clinicians reported clinically significant reductions in self-harm episodes.
Four of the 10 participants had pretreatment histories of frequent contact with the mental health crisis service. Of these four participants, three reported reductions in the frequency with which they used the crisis service, which they attributed to their participation in the DBT programme. One participant reported increased use of the crisis service, which was attributed to the evoking of emotional material in the course of DBT treatment. This qualitative assessment of reduction of crisis service usage occurred despite patients being encouraged to use the crisis service for telephone contact at times of crisis to get coaching on skills that would help them manage their crisis and keep themselves safe.
DISCUSSION
The main findings were a 100% treatment retention rate, large improvements in MCMI-III and SCL-90-R ratings and a decrease in acute hospital bed days used. While large changes were made in the 6 months of treatment, it was not expected that treatment would finish at the end of the 6 month trial. It would be reasonable to hypothesize that further gains were made in treatment beyond the 6 month period of the study. The retention rate is pleasing for a disorder recognized for its high attrition rate and compares favourably with the 83% retention rate of the seminal 1991 DBT research.
Further strengths of the study include being prospective, use of a standardized diagnostic measure (IPDE), use of two objective standardized outcome rating scales, diagnostic assessment and data collected by an independent project evaluator and large changes that occurred as indicated by effect sizes. The effect size is calculated by subtracting the post-treatment mean from the pretreatment mean and dividing by the pretreatment standard deviation. Effect size of 0.2 is considered small, 0.5 moderate and 0.8 large. The effect sizes for the MCMI-III Borderline and Paranoid personality subscales were 1.46 and 1.10, respectively. The effect sizes for MCMI-III Major Depression, Dysthymia, Somatoform, Anxiety and Alcohol Dependence clinical syndromes were 4.80, 3.02, 2.32, 1.77 and 1.13, respectively. In assessing the size of clinical change using the GSI of the SCL-90, Mehlum states that ‘A GSI value below 1.0 is conventionally regarded as indicating non-caseness’. 18 Six months after treatment began, the mean GSI score changed from 2.18 to 0.86. This change is indicative of movement from very high chronic symptomatology to ‘non-caseness’ 6 months later.
Methodological shortcomings include small numbers, rating scales being filled out at only one time interval pretreatment and one time interval posttreatment, the absence of a control group, SCL-90-R data collected for five participants only and the absence of quantitative data on self-harm and crisis service resource usage. The absence of a control group means that non-specific factors, such as patient and therapist interest, enthusiasm and positive expectations associated with a newly adopted treatment, could not be excluded as confounding variables. These limitations occurred in the context of the goals of the study, which was to be a pilot study of the effectiveness, utility and feasibility of implementing DBT into a routine existing Australasian public mental health service. Stevenson and Meares in discussing the dilemma of control groups state that ‘Since personality disorder is relatively enduring, comparisons between different periods of patients’ lives offer a suitable means of obtaining a control’. 19 Patients in this study were all being treated for chronic conditions which had been present for many years. Goals of treatment were for chronic symptoms or problems. This makes it unlikely that gains made were due to spontaneous remission or regression to the mean (the resolution of short-term symptoms in a chronic disorder).
Utility and feasibility
The outcome evaluation was intended as a pilot study assessing the feasibility and effectiveness of implementing a DBT programme within an existing public mental health service. Public facilities in Australasia have experienced progressively shorter average length of inpatient stays because of inpatient resource limitations following deinstitutionalization. Any treatment that both is clinically effective and decreases hospital usage is of substantial interest and importance.
Research questions included whether clinician training and clinical skills would be sufficient to successfully implement DBT in a system where DBT was carried out by a relatively large number of clinicians (compared with patients) and partly in a rural area. Also, New Zealand public service clinician expectations were that out-of-hours calls would be taken by a generalist mental health crisis service but not the individual DBT therapist.
Before the start of the study, seven of the 10 treating clinicians attended DBT intensive training provided by Behavioural Technology Transfer Group, comprising the 1 week full-time training followed by 6 months of study and clinical work, followed by another 1 week full-time training. A further three clinicians familiarized themselves with DBT theory and practice. Treating clinicians for the pilot study were recruited from interested clinicians within the service and from a range of professional backgrounds. Congruent with previous research, 11 our local experience was that DBT could be effectively practiced by a wide range of clinicians from different training and professional backgrounds, provided practitioners were supported with skilled supervision and/or consultation by those well grounded in the DBT model and principles. This underscores DBT's practical and clinical utility in public mental health services. 11
The work was spread among 10 clinicians with six clinicians having one patient each in individual treatment and two clinicians having two patients each. This spreading of the workload recognized the challenging nature of the work and the unfamiliarity of clinicians at the time with DBT, and was congruent with clinicians’ workload desires. While encouraging individual clinician limit-setting, DBT appears to encourage the individual therapist being reasonably available for crisis calls outside usual working hours, a dimension of DBT that differs from expectations of New Zealand public service clinicians. Despite out-of-hours crisis calls not being taken by individual therapists but by a general mental health crisis team, outcomes were positive.
The approximate amount of patient contact time was 90 minutes per week with the individual DBT therapist (individual DBT + crisis telephone contact), and 2 hours per week with the two group skills trainers. In addition, there was a 90 minute consultation meeting for therapists. Our impressions of the minimal resourcing required to establish and maintain a viable treatment team is four clinicians treating six patients utilizing a total of 22 hours of clinician time/ week. Where clinicians treat more than one patient, an economy of scale of therapist time/patient would exist, particularly regarding the consultation meeting time which the therapist would already be attending. Having eight patients attend the group skills training would result in another economy of scale.
This pilot study comprised two DBT treatment teams, one urban and one rural. While there are reports of successful implementation of DBT in urban areas, this is the first study, to the best of our knowledge, of successful implementation of DBT in a rural area.
It was intended that the study's outcome would influence future service delivery decisions. The results of this pilot study were instrumental in obtaining funding for the ongoing provision of DBT. Waikato District Health Board now has a dedicated financially ring-fenced DBT service as part of its routine service, staffed part-time by clinicians who are imbedded within existing community mental health services. Having DBT clinicians imbedded in existing teams maximizes integration, knowledge dissemination and inclusivity, avoiding some of the dangers of standalone specialist services. Waikato District Health Board provides public mental health services to a population of 350 000, has been providing a DBT service now for 5 years and is currently providing DBT treatment for 20 patients with the diagnosis of BPD.
While the primary goal of the study was to assess DBT effectiveness, utility and feasibility in Australasia, the results also provide a basis for a future Australasian RCT. To address the potential confounding variable of patient and therapist interest, enthusiasm and positive expectations, DBT could be compared to another treatment associated with such attributes.
CONCLUSIONS
This DBT pilot outcome study demonstrated efficacy of the treatment provided and is the first peerreviewed publication of DBT treatment conducted in Australasia of which we are aware. Dialectical behaviour therapy has practical and clinical utility of relevance to Australasian public mental health services. It is feasible to implement a DBT service within existing Australasian public mental health services.
Footnotes
Acknowledgements
Thanks to the patients who agreed to take part in this study, Waikato District Health Board DBT clinicians who generously made themselves available, Waikato District Health Board for fully supporting the project, Wendy Tuck for her perseverance in getting the project off the ground, Susan Yates for her work as research assistant, John Fitzgerald for his support and consultation, Nigel Marsh for his data analysis input and Mike Batchelor and Graham Mellsop for their reviews of an earlier version of this paper. <ref<