
Abstract
Keywords
Perinatal psychiatry is an emerging area of specialization within psychiatry.[1] At an organizational level, this is reflected in the recent move to form a section for Perinatal Psychiatry in the Royal Australian and New Zealand College of Psychiatrists. One can also point to a burgeoning literature,2–6 integration in clinical service delivery frameworks and expanding services as indicators of the growth in this field.[7], [8]
Perinatal psychiatry is the subspeciality of psychiatry which is devoted to the mental health needs of new parents and infants in both the pre and post natal period. As such, it is closely associated with the emergent clinical and research field of infant mental health, the latter including a range of other mental health professionals and interdisciplinary approaches.
As part of the process of further developing perinatal psychiatry as a subspeciality of psychiatry, there is a need to define the core skills and knowledge required of professionals working in this area. It is therefore timely to obtain an overview of the current clinical practice of infant mental health (IMH), including the underlying models of practice, the group of professionals providing clinical services, their specific IMH training and IMH professional development requirements. In turn, this provides a means of discussing the directions in which perinatal psychiatry might usefully develop in the future. The paper addresses these issues with respect to the role which mother–infant psychotherapy might have as a key intervention within perinatal psychiatry.
Mother–infant psychotherapy is a relatively new treatment model within perinatal psychiatry.[9] This field bridges adult psychiatry and child psychiatry as part of the ethos of treating mothers and infants as a single dyadic relationship. As in many new areas, terminology used to describe IMH interventions vary from mother–baby, parent–infant, infant–parent to infant centred modes of therapy. Part of the difficulty in this field is defining what is mother–infant psychotherapy and what disorders it can reasonably be used to treat. Whether mother–infant psychotherapy (MIPT) is primarily a treatment of the mother–infant relationship, maternal psychopathology or infant psychopathology, or all three, is still a matter for debate. Another area of inquiry is whether models that aim at prevention, early intervention or treatment are themselves best understood under the rubric of models of MIPT or reflect the fact that MIPT is but one of a range of clinical interventions to be used.
A common dilemma in psychotherapy research is the isolation of the critically effective ingredients of a therapeutic intervention.[10] As applied to MIPT, some have proposed that the critical ingredient is merely the physical presence of the mother and infant and the focus on their relationship.[11] However, if this were true one would be hard pressed to justify the need for specialized mental health interventions over and above community mother's groups, general practitioner or Maternal Child Health Nurse (MCHN). In contrast, psychodynamic concepts such as therapeutic alliance or a corrective emotional experience have been shown to account for the active ingredients in psychotherapy.[12], [13] However, as Stern reminds us, the motherhood constellation is a complex systemic interaction between mother, father, infant and potentially therapist.[4] Thus, it is possible for the infant to be physically present but not in the mind of the therapist or even the mother, in which case mother–infant psychotherapy may become a mother-only therapy.
There are a number of other important ways in which MIPT differs from the established tradition of individual psychotherapy. The significance and importance of such interventions as MIPT is growing alongside studies that point to the crucial importance of the mother–infant relationship for the subsequent emotional, psychological and social development of the child. The field of perinatal psychiatry is a rapidly growing area, which draws on disciplines ranging across the biological, psychological and social domains. Work with mothers and infants brings new challenges to psychiatry that has tended to focus on either the mother within an adult psychiatry context, or the infant within a child psychiatry setting. In this sense, both the underlying theoretical frameworks and corresponding interventions are, to some degree, in need of revision.
The aims of this survey were to explore trends in MIPT theory and practice among Melbourne-based mother–infant mental health clinicians, to examine for any differences between psychiatrists and nonpsychiatrists in their practice of MIPT, and finally to look for any differences between psychotherapy trained and other professionals surveyed in their practice of MIPT.
METHOD
Participants
The survey was conducted in 2002 in Melbourne, Victoria. The survey was limited to professionals working in perinatal psychiatry in Metropolitan Melbourne. This included those professionals working in the fields of mother–baby psychiatry, infant mental health, obstetric liaison and related areas. It encompassed all relevant professional disciplines including psychiatry, psychology, social work, general practice, psychiatric and maternal child and health nurses. Names were obtained from public lists of relevant professional associations, hospitals and clinics. An attempt was made to sample the entire population; however, the difficulties in defining and identifying this population were a major obstacle.
Measures
A purpose designed self-report questionnaire was developed which sought responses to a number of open-ended questions in addition to basic demographic data. All responses were anonymous.
Data analysis
The data were analysed using both quantitative and qualitative methods. The quantitative analysis was performed using the Statistical Package for Social Sciences (SPSS for Windows, Version 11) and included descriptive statistics and the chi-squared test. However, low numbers invalidated certain analyses. The value for significance was a p-value of 0.05 or less. In order to be able to analyse the data using quantitative methods, the data were coded using a purpose designed coding sheet. The qualitative analysis included detailed examination of all responses to individual questions in order to examine patterns for individuals and within defined professional or therapeutically orientated groups.
Indications stated by psychiatrists and non-psychiatrists for mother-infant psychotherapy
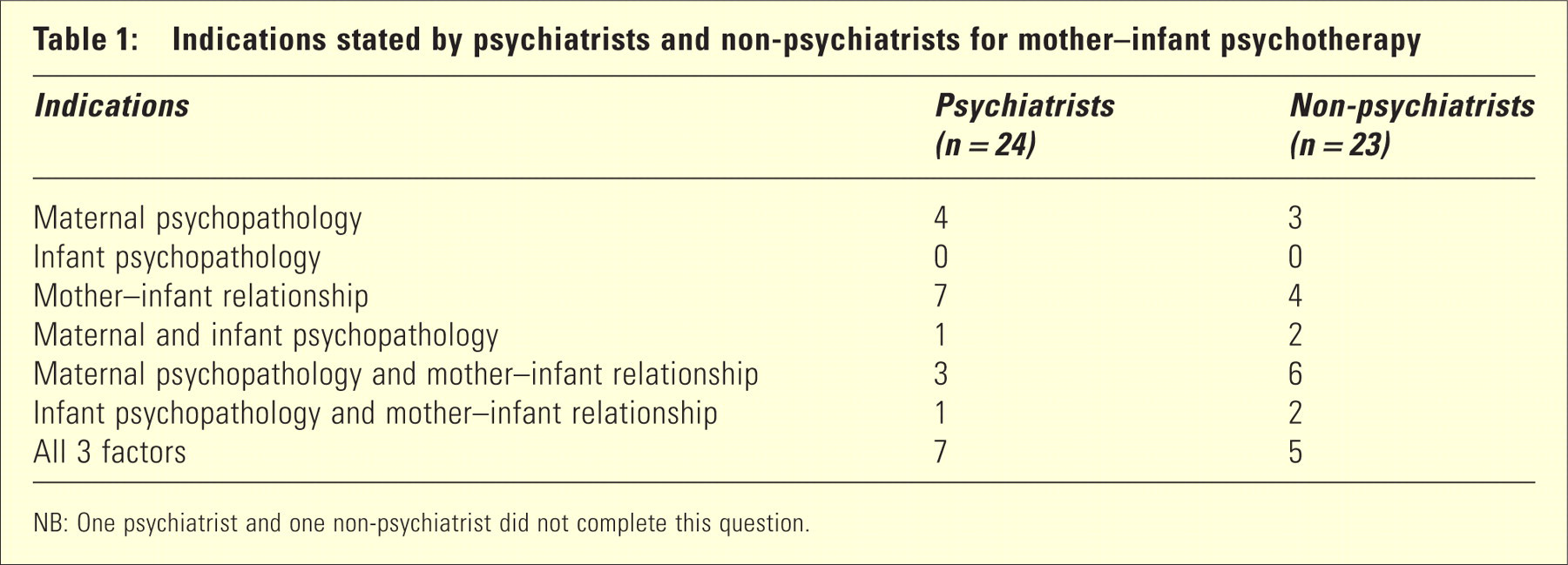
NB: One psychiatrist and one non-psychiatrist did not complete this question.
RESULTS
A total of 75 questionnaires were distributed and 47 surveys were returned, an overall response rate of 63%, of which 23 questionnaires were returned from non-psychiatrists and 24 from psychiatrists.
The survey sample was 21% male (n = 10) and 79% (n = 37) female, which reflects the marked gender discrepancy in these professional groups. This discrepancy was apparent in both the psychiatrist and nonpsychiatrist groups. The age range of participants was from 25 to over 55 years of age. The largest group was 35–44 years of age, which represented 36% of the sample; 45–54 years of age and 55 years and older each represented 26%, while the remaining 12% were in the 25–34 years group. This finding is consistent with the subspecialty group of professions that the survey targeted, suggesting that participants had completed their respective generalist clinical training and undertaken further training in the specialist clinical area of Infant Mental Health. Of the respondents, 13 (28%) had formal psychotherapy qualifications, mostly family therapy training followed by psychodynamic training. Only 2 (4%) had specific MIPT training.
Indications and reasons for referral for mother–infant psychotherapy
Twelve respondents (25%) listed all three factors of infant psychopathology, maternal psychopathology and mother–infant relationship difficulties as the most common indication for referral. This was followed by 11 responses (23%) suggesting that the mother–infant relationship was the reason for referral. Maternal psychopathology alone was the indication given by seven respondents (15%). Infant psychopathology alone was not stated by any of the respondents as a reason for referral. Only psychiatrists listed maternal psychopathology other than postnatal depression, such as ‘personality disorders’, ‘bipolar affective disorder’ and ‘schizophrenia’. When nonpsychiatrists referred to maternal psychopathology, it was exclusively postnatal depression and associated anxiety. This may suggest that psychiatrists are mostly assessing and treating severe maternal psychopathology, which would be appropriate. However, in terms of indications for treatment, this may suggest that a broader understanding of adult psychopathology is required for non-psychiatric clinicians in this field.
Theoretical models of mother–infant psychotherapy utilized by clinicians
The most common model was psychodynamic, which was used by 33 respondents (70%) followed by two or more different models used by seven respondents (15%) and then cognitive behavioural therapy and ‘no model’, which were each used by four respondents (9%). Two respondents listed specific mother–infant models while only one respondent listed family therapy models.
Why clinicians choose their specific model
Answers to this question included ‘helpful’, ‘proven to be helpful’, ‘training and belief’ and ‘makes sense’. Other respondents referred to their general psychotherapy orientation and training and to the success they have had using their particular model. Those who stated a specific general model to the previous question tended to provide more specific answers to this question. An example is the respondent who gave ‘CBT’ (cognitive behavioural therapy) as their model who then stated the reason they used this model was to ‘gather outcome data’ and because it was ‘manualized and therefore easier to learn’. Another who gave their model as ‘psychoanalytic’ stated under this was ‘most effective’.
When terms such as ‘proven’ and ‘most effective’ were used, no supporting evidence was mentioned. Those who gave more than one model and/or stated they were eclectic, wrote of factors such as ‘different models work for different people’ and [different] ‘presentations’. They also wrote of the importance of being ‘adaptable’.
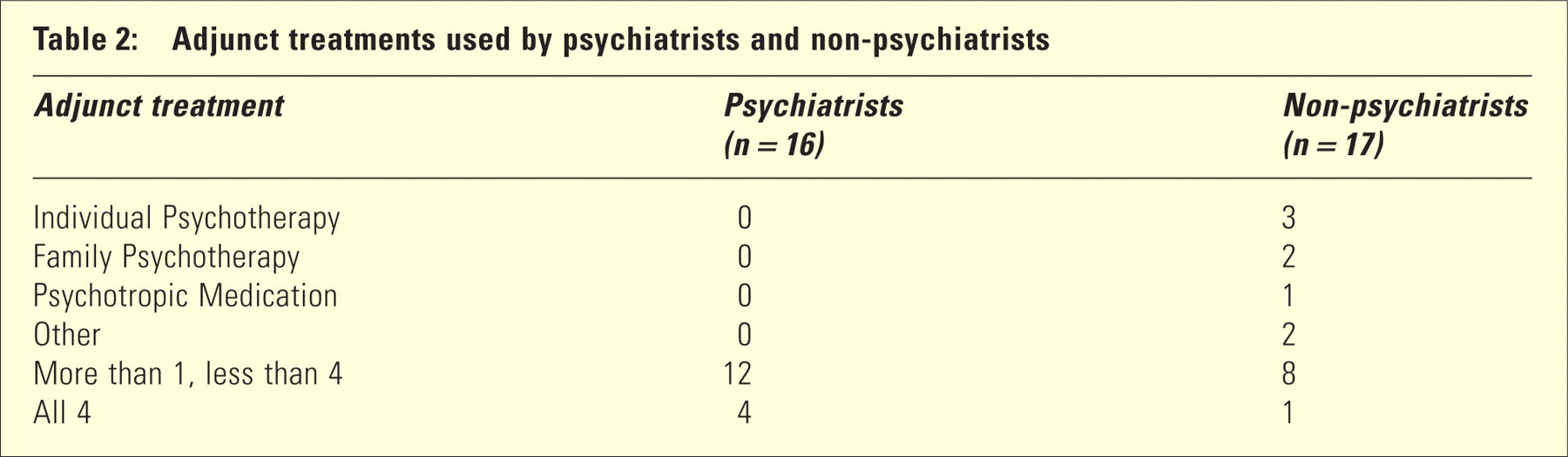
Adjunct treatments used by psychiatrists and non-psychiatrists
Authors of articles/books on mother–infant psychotherapy which have most influenced clinicians’ work in this area
The most common authors mentioned were Daniel Stern, Donald Winnicott and Selma Fraiberg. In addition, more general psychoanalytic authors such as Melanie Klein and Jacques Lacan were named. The respondent who named CBT as their sole model only listed a single author's name under this section. Of the group who gave specific models of mother–infant psychotherapy under the models question, most gave names of authors that related to their chosen model, for example, Brazelton's model and Muir's ‘Watch, Wait and Wonder’. No respondent gave names totally unrelated to the field of MIPT. Most gave names, which broadly related to their model of psychotherapy.
Is mother–infant psychotherapy a discrete intervention or to be practised in conjunction with other interventions?
In answer to this question, 41 (88%) said MIPT should be practised in conjunction with other interventions and 6 (12%) answered as a discrete intervention. This question was then partially repeated in a subsequent question, ‘Do you accept referrals for mother–infant psychotherapy as a specific or separate intervention?’ To this question, 30 (64%) answered yes. The lack of consistency of response may suggest some confusion about the role that MIPT plays as an intervention within perinatal psychiatry. Table 2 shows the adjunct treatments listed by respondents.
To what extent should the therapist be prepared to give advice on mothercraft issues (e.g. routine, sleeping, feeding, development)?
The answers ranged from ‘always’ to ‘sometimes as appropriate’ to ‘never’. The majority answered ‘as appropriate’ followed by 11 (23%) whose answers suggested that they never offer advice and four (9%) who are always prepared to give advice. Answers therefore ranged from ‘core part of practice’ to ‘should be left to MCHN’. Although others gave more subtle answers such as ‘knowledge of mothercraft areas and developmental areas is essential but not to be used in advice model’ and ‘advice (very rarely), exploration of meaning’.
The role of the father in mother–infant psychotherapy
Only one respondent felt there was no role for the father, 25 (53%) would include the father sometimes and seven (15%) always. Of those respondents who included the father always, two were male respondents and live were female, three were psychiatrists, one was a social worker, one a psychiatric nurse and two were psychologists. In terms of models this group used, all were general models not specific to MIPT; live were psychodynamic, one CBT and one eclectic.
Would specific training in mother–infant psychotherapy be helpful?
All participants gave a positive response to this question. As one respondent stated, ‘it's a specialist intervention –why wouldn't you want to be trained’. Another stated ‘because everyone in the area talks about it, but where do you actually learn how to do it’. One respondent brought up the issue of the baby not having speech and therefore needing ‘particular techniques to be able to engage baby in the therapy’. Another respondent stated that training would be helpful to ‘improve my skills, establish the importance and legitimacy of this therapy as distinct and important’ and another stated that it would ‘broaden perspective’ more than ‘RANZCP training’. One respondent stated that it would be helpful only ‘as long as it is broadly based and not just psychodynamically orientated’. Another respondent stated ‘there appears to be no clarity or uniformity to this practice at present –no standard assessment or clear indications for its use and form e.g. short/longterm/group etc’.
Quantitative analyses
The only associations that came close to reaching statistical significance were professional qualifications (psychiatrists vs. non-psychiatrists) and psychotherapy qualifications, and gender and professional qualifications. The respondents showed a trend towards an association between professional qualifications and psychotherapy training, that is, not being a psychiatrist was associated with having additional psychotherapy training χ2 (1, n = 47) = 2.962, p = 0.085. The respondents showed a significant association on the question concerning gender and professional qualifications between being female and in the non-psychiatrist group χ2 (1, n = 47) = 2.962, p < 0.01. No significant associations were found between psychotherapy qualifications and sex; professional qualifications and indications for mother–infant psychotherapy; professional qualifications and model of psychotherapy used; professional qualifications and other interventions used; professional qualifications and overlap with mothercraft advice; professional qualifications and inclusion of the father.
DISCUSSION
The survey had a reasonable response rate and was balanced between psychiatrists and nonpsychiatrists. Mail surveys attempt to avoid interviewer bias through their design; however, they may still be subject to socially desirable answers. Such bias may apply in this case if professional prestige acts as an influence producing answers which suggest a higher level of competency and sophistication. There was an attempt to address this response bias through the use of open-ended questions and anonymity. In addition, since the field itself consists of a small number of professionals, the numbers surveyed were small and conflned to one geographical region.
The survey attempted to sample the entire population of clinicians in the field. Nevertheless, given the difficulty in defining this group, it was unlikely that this was achieved. While one should be cautious in drawing broad conclusions from the findings, it needs to be said that a large proportion of the clinicians who provide mental health services to the population of mothers and infants in the state of Victoria, Australia, have been surveyed.
The most important findings were qualitative in nature. These focused on the difficulty of psychotherapy practice in a relatively new field with little available training. The coherency of models and understanding of MIPT practice varied very widely in the responses. There were no clear trends in the practice of MIPT in Melbourne. There also did not seem to be a preponderance of influence, trends or models from the UK and Europe, or the USA. There appeared to be a wide set of practices, but little use or knowledge of the specific models of MIPT which have been developed, for example Watch, Wait and Wonder or Interaction Guidance.[15], [16]
A lack of an understanding of maternal psychopathology as an indication for referral was evident despite the fact that there is clear evidence regarding the impact and significance of maternal psychopathology other than depression on mother–infant interactions and infant symptomatology.[3], [14] Therefore, an expansion of indications for MIPT to these at risk dyads and a greater focus on education and professional development in the area of broader based assessment is required.
Results also indicated a range of understandings of infant psychopathology. This varied in sophistication from ‘unsettled baby’ to ‘the baby's distress/dysregu-lation/depression’. It is also to be noted that no respondents listed infant psychopathology alone as a reason for referral. No respondents referred to ‘Zero to Three’ diagnostic classifications[17] nor to ‘functional disorders of infancy’. This may suggest there is an insufficient understanding of both the diagnostic system and the clinical range required for specific infant referral for MIPT.
While training was felt to be overwhelmingly a good thing, few had undertaken training. There was, however, a wide appreciation of influential authors in the field and the range of indications for which MIPT can be used. The reported diversity of practice may reflect the different practice settings of the respondents, their training or their idiosyncratic preferences. There is a clear need for MIPT to define its target population and likely efficacy.
This study has highlighted the difficulty within perinatal psychiatry and associated professions in defining MIPT. There is a lack of differentiation between interventions that target prevention, early intervention or treatment or those aimed at addressing maternal psychopathology, infant psychopathology, relationship disturbance or all three. In addition, the survey results indicate that MIPT practice may not be fully understood by those who practice it, perhaps in part due to a lack of training and coherent understanding of models evident in the responses.
Overall, the survey results suggest that there is a significant need for development and training in MIPT, at least within Victoria, and this need crosses professional disciplines.