
Abstract
Australia's mental health burden is high. One-fifth of all Australians report that they have suffered from at least one mental illness in the last 12 months and mental illnesses account for 27% of years of healthy life lost to disability.[1] Despite these statistics, less than 40% of people with mental illnesses receive mental health care, compared with 80% for common physical conditions.[2]
The burden of mental disorders is exacerbated by a mental health system that is deficient in a number of respects. First, the lack of integration between health professionals, health services and patients leads to poor information sharing and suboptimal treatments across the care contin-uum.[3], [4] For example, patients are often required to disclose very personal information numerous times to strangers, face frustrating attempts to prove they deserve help and have inadequate access to health informa-[2], [5], [6] Implementing programmes that aim to enhance collaboration between independent parts of the mental health system has improved patient care;[7] however, such programmes have failed to impact upon mental health system reform, largely because of sustainability problems.[4] Further efforts towards sustainable integration are required to increase the accessibility and efficiency of Australian mental health services.
A second deficiency of the mental health system is that outcome measurement is irregular and, consequently, longitudinal records of patients’ mental health status are limited.[8] Clinicians are rarely trained or encouraged to administer the numerous reliable and valid measures of mental health status that are now available.[9], [10] It is strongly recommended that regular outcome measurement become routine clinical practice to facilitate mental health tracking of individuals, communities and populations, triage for early interventions, and evaluation of best practice.[8]
A third deficiency is that the current reactive model of care in which consultations are provided only when patients actively seek them is inappropriate for chronic conditions, such as depression, which are characterized by periods of acute symptomatology followed by remission.[8], [11] The National Action Plan for Depression (1998–2003) stressed the need for health systems to follow patients through the continuum of care, providing specialist care during acute episodes and relapse prevention strategies and ongoing progress monitoring during remission.[12]
E-health systems show promise in facilitating health care reform and can help overcome the three deficiencies outlined. The provision of centralized online medical records and secure online communication systems can integrate patients and health care providers across the continuum of care.[13] The delivery of online assessment questionnaires enables regular outcome measurement and can provide patients and clinicians with feedback on progress.[14] Such systems enable patients to receive ongoing care beyond acute episodes with minimal face-to-face contact. Progress can be tracked remotely by case managers who can follow up patients who are likely to need additional support. Such systems maximize the application of limited health resources by targeting those who need help when they need it. E-health services are currently being used by health care providers and patients and the use of the Internet in health is increasing.[15] An estimated 84% of Internet users seek health information using this medium.[13] The utility of e-health systems has been recognized,[16] and such systems have been implemented in government initiatives such as HealthConnect and Health-Insite. Publicly accessible Australian mental health sites that provide health promotion and/or online therapy include Sentiens (http://sentiens.com), beyondblue (http://www.beyondblue.org.au), the Black Dog Institute (http://www.blackdoginstitute.org.au), andMoodGYM (http://moodgym.anu.edu.au). There is accumulating evidence that online therapy can be effective in reducing depression severity.[17], [18]
A comprehensive Australian e-health system, called RecoveryRoad, provides a centralized e-medical record, an e-consultation system and e-progress monitoring. The system, which has been in use since 2002, facilitates a proactive and long-term approach to the management of chronic conditions. This paper describes the implementation and evolution of the depression module, and presents early outcomes from its implementation within the public and private mental health sectors of Western Australia.
METHOD
RecoveryRoad for depression is an e-health system designed to be used by patients and clinicians as an adjunct to usual treatment. It aims to increase the effectiveness and efficiency of treatment. Table 1 shows a summary of the features it provides for patients and clinicians. The system aims to facilitate self-management and provides patients with a secure online consultation system, automated patientadministered progress monitoring questionnaires with feedback, systematic psychoeducation, and evidence-based therapy (cognitive behavioural therapy, CBT). Treating clinicians across the continuum of care can access secure online information on their patients’ progress and can use the e-consultation system to communicate with patients and other clinicians. Regular monitoring of patient progress beyond the acute phase by case managers enables early detection of problems and consequent proactive early intervention.
Summary of the features of the patient and clinician sides of RecoveryRoad for depression
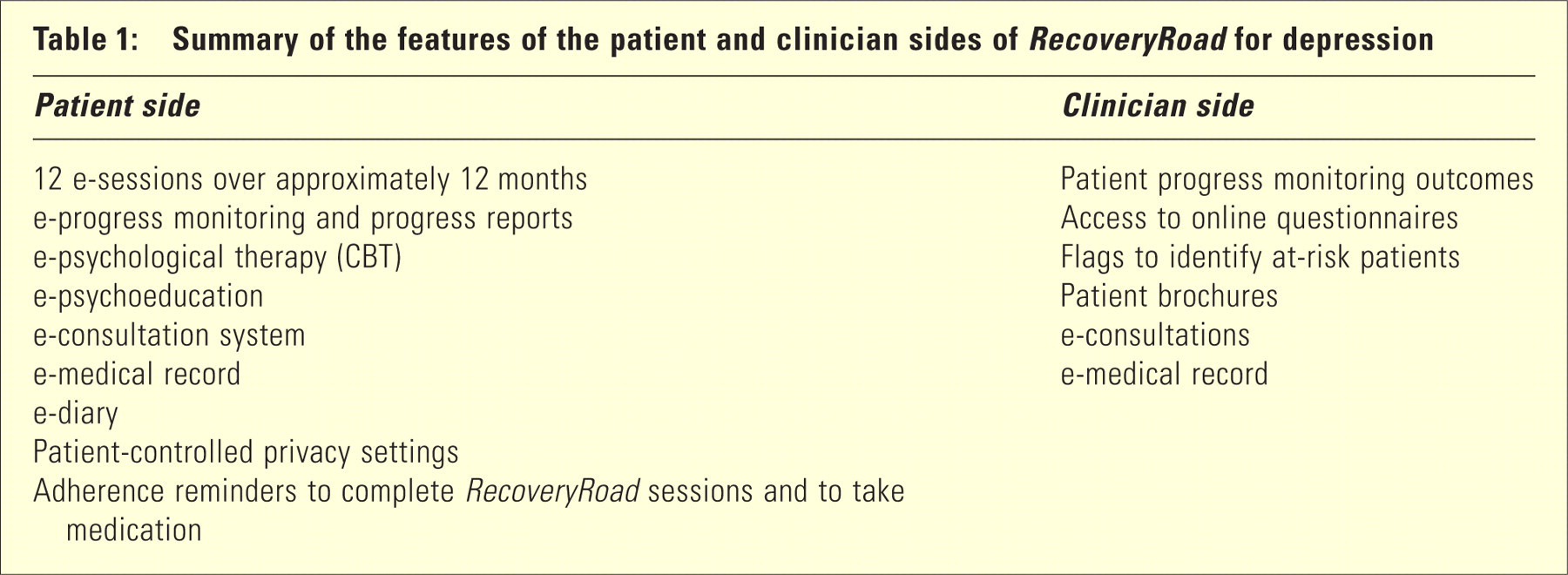
RecoveryRoad provides patients with 12 online sessions over approximately 12 months. In each session, patients complete online progress monitoring questionnaires and receive feedback on their results. In its first evolution, the system provided patients with written feedback on all outcome measures and a progress graph showing depression severity scores over sessions. More recently, feedback on outcome measures was bolstered with a summary progress report, generated for each patient upon completion of each session. Following the completion of progress monitoring questionnaires, patients can access psychoeducation, which is delivered on a session by session basis. Additional online features include CBT, a secure e-consultation system, an e-diary, a record of currently and previously prescribed medications, additional psychoeducational brochures with practical tips on overcoming common difficulties, a progress graph, email reminders to take medication, and patient-controlled privacy settings. Patients’ erecords are made available to their treating clinician/ s. The privacy settings enable patients to grant orrevoke specific clinicians’ access to each component of their records. Each time patients log on, they are asked whether they have taken their medication as directed.
Upon commencement of RecoveryRoad, sessions are scheduled weekly and gradually become less frequent as follows: sessions 1–4 are weekly, sessions 5–6 are fortnightly, sessions 7–10 are 4-weekly, and sessions 11–12 are 12-weekly. Reminders to complete each session were added as the system evolved. Initially, patients received no adherence reminders. Automated email adherence reminders were then introduced, followed by the addition of a case management system. Case managers were mental health nurses or psychologists who monitored patients’ adherence to RecoveryRoad and contacted those who had been nonadherent for approximately 1 week. Contact was initiated via email and followed up with a telephone call if the emails remained unanswered.
Clinicians could access patients’ progress monitoring outcomes and e-health records and, as the system evolved, names of patients who had severe depressive symptomatology, severe functional impairment or self-reported medication changes. Clinicians could use online resources such as a wealth of questionnaires and printable mental health information brochures. Clinicians also had access to a secure econsultation system, which they could use to respond to patients’ enquiries.
Procedure
All participating patients were referred to Recovery-Road by their treating clinician as an adjunct to usual treatment. Inclusion criteria were as follows:
Currently receiving treatment for depression under the care of a mental health professional; Previously or currently satisfying the diagnostic criteria for a major depressive episode; Access to a computer and the Internet; Willing to use the Internet as part of treatment; Willing to provide informed consent; Sufficient cognitive functioning and proficiency in English; and At least 18 years of age.
Four primary outcomes were measured: RecoveryRoad adherence, self-reported medication adherence, depression severity, and clinician and patient ratings of satisfaction with the system. Depression severity was measured using the Depression Severity Scale (DSS), which has been validated against the Depression, Anxiety and Stress Scale (DASS).[19] Based on 141 responses, the DSS was found to be reliable (α = 0.94), and convergent validity between the DSS and the depression subscale of the DASS was high (r = 0.86).
Ratings of satisfaction were obtained from patients in the public and private sectors using an online questionnaire. At the time of distribution, satisfaction questionnaires were administered either to all patients within the private sector or all patients within the public sector. Questionnaires were completed by those patients who were adhering to the system at the time of distribution. Ratings of satisfaction were obtained from all clinicians in the public and private sectors who had, at the time of distribution, referred patients.
RESULTS
One hundred and forty-four patients were referred to RecoveryRoad for depression by their treating clinician. Ninety were female, and their ages ranged from 19 to 64 years (mean = 42 years). Most (n = 118) were referred from private psychiatric practices, 23 were referred from public psychiatric services (19 were from an adult outpatient clinic and four were from a psychiatric hospital), and three were from general practice. Of the original 144 patients referred, seven withdrew prior to using the system and 23 did not complete a session. Data from two patients were lost due to technical difficulties. The gender and age of those who used the system did not differ significantly from those who did not (Gender: Kolmogorov-Smirnov Z = 0.85, p = 0.47; Age: t (142) = –1, p = 0.44).
Figure 1 shows patients’ adherence to sessions as a function of type of adherence reminders received.[20] The rate of adherence decline was greater for patients who received only automated reminders than those who received case management. By session eight, adherence for case management was 34% higher than automatic reminders. A Cox regression survival analysis revealed a significant hazard ratio of 2.43 (95% CI = 1.01–5.84) for automated reminders relative to case management when controlling for baseline depression severity. Medication adherence at each session ranged from 91% at session one to 100% at session six (mean = 96%).
Adherence to RecoveryRoad across sessions as a function of adherence reminders (automated reminders, n = 69; or case management, n = 29). Note that for session 8, n = 26 for the case management condition, as three patients in this group were yet to complete session 8.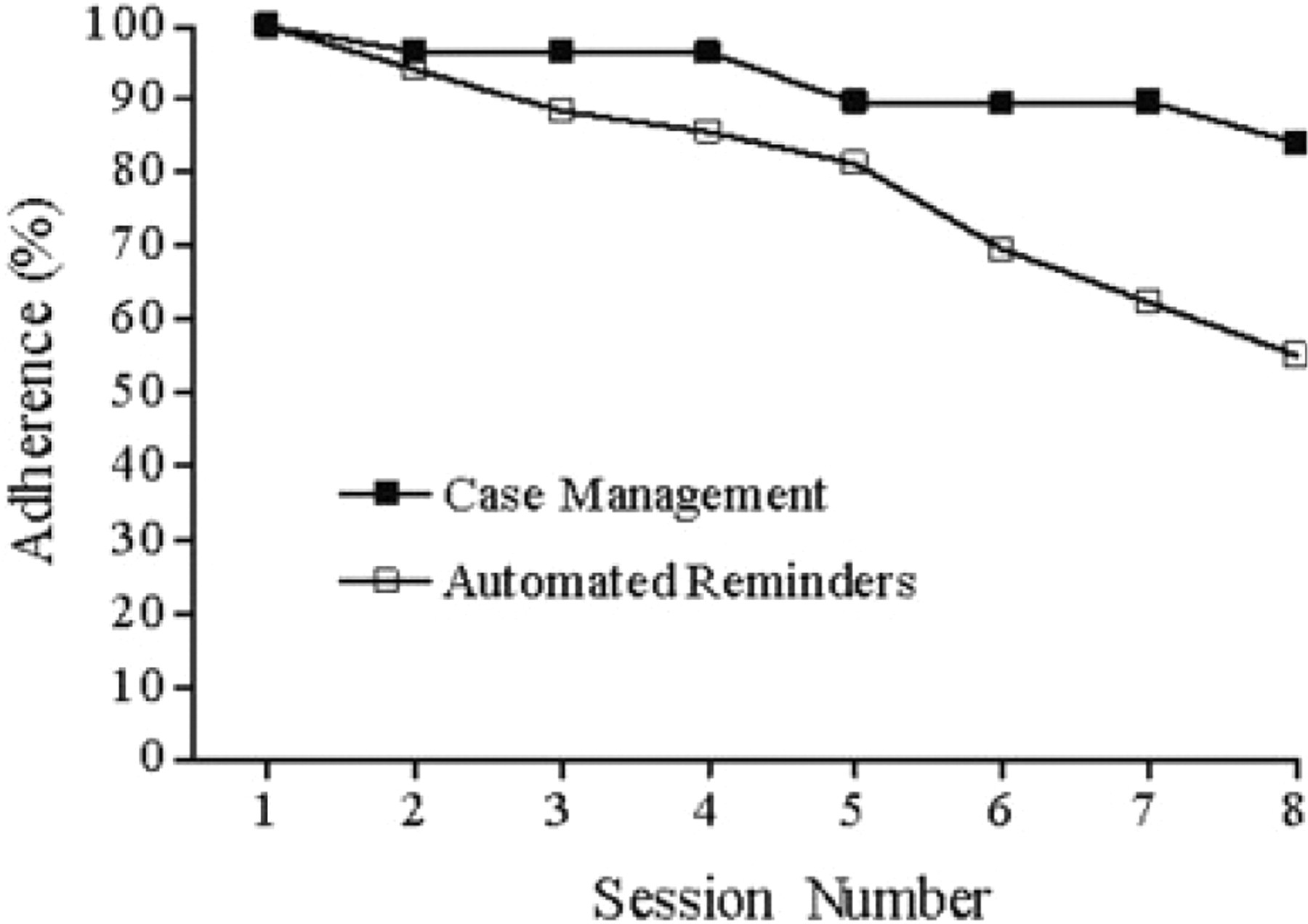
Figure 2 presents the mean Depression Severity Scale score for all patients who completed at least eight sessions (n = 72). Mean DSS was severe at session one and declined to mild by session eight, a large reduction in depression severity (d [within-subject] = 1.03). Fifty-eight per cent of patients had subclinical levels of depressive symptomatology at session eight.
Depression severity of patients who completed at least eight RecoveryRoad sessions (n = 72) showing ±1 SEM.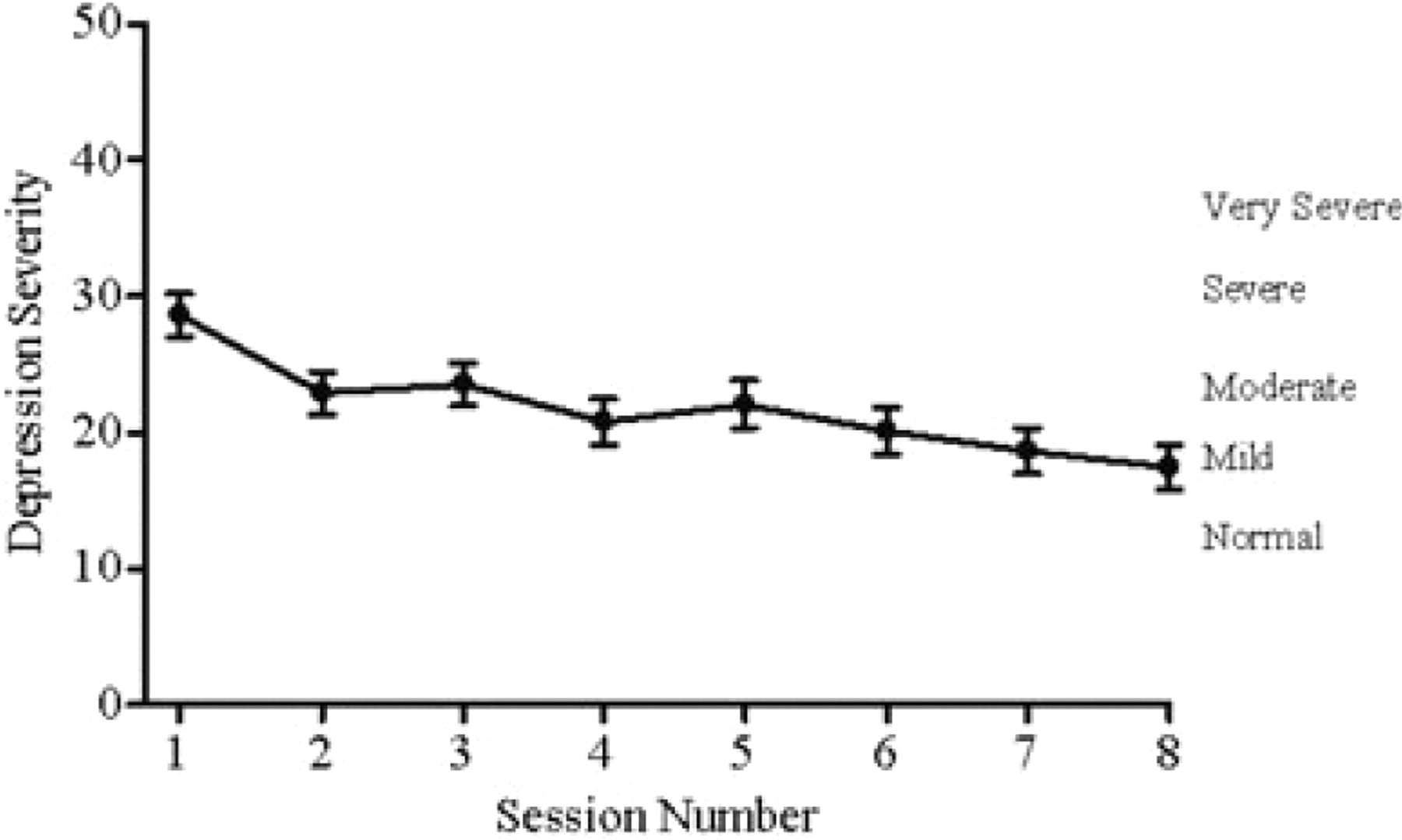
All surveyed clinicians reported that they were satisfied with the system; 83% reported that it helped their relationship with their patients, and 100% reported that it helped their patients to better manage their condition.
DISCUSSION
Adherence rates to RecoveryRoad were higher than previous reports of Internet-based mental health interventions. Previous online mental health programmes report adherence rates of 1% in non-trial settings and 22% in trial settings.21–23 For Recovery-Road, 84% of patients receiving case management and 55% of patients receiving automated reminders completed at least eight sessions. The provision of case management to patients proved to be an important feature in maintaining adherence.
Self-reported medication adherence after eight sessions (approximately 23 weeks) was very high, at over 90%. Adherence is a major concern as non-adherent patients receive incomplete treatments, which are less efficacious, and may develop negative beliefs about treatments (e.g. ‘antidepressants are unnecessary’) that affect their willingness to adhere to subsequent attempts.[24] In a review, median adherence to pharmacological treatments for depression was 63%.[25] Katon et al. reported a medication adherence rate of approximately 73% after 6 months for a group provided with increased support that included psychoeducation and monitoring.[26], [27]
A large reduction (d = 1.0) in depression severity was found in the patients who completed eight sessions of RecoveryRoad. Christensen et al. found an overall moderate effect size (d = 0.4), for a 6-week Internetbased CBT intervention for depression for users who were not receiving any other treatment;[17] the effect size was larger in those who completed the intervention (d = 0.6). A review of computerized CBT interventions for depression (not necessarily delivered on the Internet) reported effect sizes ranging from 0.64 to 2.22.[28] Compared with these interventions, the clinical improvements observed in the present research are at least as good as those found for online and/or computerized CBT interventions. However, it must be kept in mind that patients in the present research received usual treatment in addition to RecoveryRoad. Feedback on RecoveryRoad from patients and clinicians was positive. The majority of patients surveyed were satisfied with the system itself and reported that it increased their knowledge of depression, and enhanced their relationship with their clinician. This is encouraging given that patients are often dissatisfied with the information and care they receive.[2], [5], [6] Clinicians were also satisfied with the system, reporting that it enhanced their relationship with their patients and improved their patients’ ability to manage their illness. While based on small numbers of respondents, the feedback provides a promising indication that e-health services have the support of the clinicians and patients who use them.
The main strength of the current research is that it was conducted in a naturalistic setting in which patients used RecoveryRoad at their own pace and place of choice (e.g. at work or at home) while receiving usual care from their treating clinician. It is likely that the data collected are representative of realworld conditions and subsequently have a high degree of external validity. Weaknesses include the inherent bias associated with those patients and clinicians who actually used the system, the small sample size from which the satisfaction data were collected, and the changes in the system that evolved during the trial. The inability to control for the ‘usual treatment’ delivered was also a methodological shortcoming. Also, it needs to be made clear that the system is not a replacement for clinical care, merely an adjunctive tool.
Future research will include analyses of outcomes over longer periods of time, large-scale randomized control trials, and cost-effectiveness evaluations. Such research will further investigate the impact of case management on adherence to the system, and factors that contribute to non-adherence to treatments and poor health outcomes.
Footnotes
Acknowledgements
The authors would like to thank the Office of Mental Health, Western Australian Department of Health and the Commonwealth Department of Health and Ageing for their financial contribution to the research. Please note that the views expressed are those of the authors and do not necessarily reflect the opinions of the Office of Mental Health or the Commonwealth Department of Health and Ageing.