
Abstract
Objective:
Renal colic caused by ureteral stone is commonly encountered in the emergency department (ED). This study was designed to measure meridian electrical conductance of patients with ureteral stone in emergency settings.
Design:
A cohort of patients who had ureteral calculus and acute renal colic and who had visited the ED was enrolled in this study. A device, the design of which is based on the Ryodoraku theory, was used to measure the meridian electrical conductance of patients in the ED. Sixty (60) patients (aged 42.0 ± 12.6 years) who had a primary ED diagnosis of ureteral calculus or renal colic were enrolled. Thirty (30) healthy volunteers (aged 40.8 ± 11.7 years) were recruited to serve as controls.
Results:
Statistical analysis showed that (1) the average electrical conductance of the patient group was statistically lower than that of the control group (p < 0.01), (2) the average index of sympathovagal balance of the patient group was statistically higher than that of the control group (p < 0.01), (3) the average coefficient of variation of the electrical conductance and index of sympathovagal balance in the patient group was statistically different from that in the control group (p < 0.01), and (4) the patients who needed intervention had a higher autonomic nervous imbalance than the patients who had spontaneous stone passage (p < 0.01).
Conclusions:
Measures of electrical conductance, especially the index of sympathovagal balance, may be used as valuable supplementary diagnostic methods for selective intervention in patients with acute renal colic.
Introduction
In Traditional Chinese Medicine, skin conductance was significantly high at acupuncture points. 6 Skin conductance response, a measure of the skin's conductance between two electrodes, is typically measured by applying a small direct current (DC) signal through two electrodes placed on the skin. 7 Skin conductance changes according to the activity of the subjects' autonomic (sympathetic) nervous system. 8 It has been used to investigate changes in human moods or the mechanism of the autonomic system. 9 Recently, a prospective, randomized pilot trial of acupuncture of the kidney–bladder distinct meridian to relieve lower urinary tract symptoms 10 was investigated based on the Ryodoraku (meridian) theory. The properties of meridians can reflect the condition of certain organ(s) when their mutual relations and changes with microelectrical current are analyzed and compared. 11 The electrical state of the acupuncture points of a human subject is measured by a computerized testing instrument with a very low electrical current. Our previous study showed that during a weight reduction program, meridian electrical conductance increased with the decrease in body mass index in obese people. 12
Many studies have provided mapping transforms between the electrical information associated with various medical syndromes, signs, symptoms, and diseases. 6 However, no research concerning the application of meridian electrical conductance theory for the diagnosis of renal colic has been reported. In the present study, we used a device based on the electrical conductance theory 11 to measure the meridian electrical conductance for patients with renal colic. The purpose of this study was to evaluate whether measurement of electrical conductance of patients with renal colic on ED presentation could predict a patient's course of treatment.
Methods
Study design and subjects
All procedures were approved by the Ethics Committee on Human Experimentation of the Lin Shin Hospital, Taiwan (Lin Shin IRB No. 000011). Written informed consent was signed by the patients themselves or their next of kin before the study. This study was conducted in a regional hospital with certified emergency physicians that provided care for approximately 30,000 patients per year. The certified urologists were consulted if necessary in the ED. From February 2008 to September 2008, adult patients (ages between 14 and 80) visiting the ED were consecutively enrolled when they suffered from acute colicky pain. Urinalysis, plain abdominal film, ultrasonography, and/or helical CT were arranged to confirm the diagnosis of ureteral calculus. They were recorded by the same emergency physician. Patients who had a history of nephrectomy or renal tumors, ureteral calculus with hydronephrosis within 3 months, metal material implant, or other conditions such as peritonitis, systemic inflammation, edema of limbs, abnormal skin diseases, and overweight with body–mass index more than 27 were excluded. Sixty (60) patients were enrolled in the study group. On the other hand, 30 control people were recruited to serve as control group at the same time. They did not have any special history (exclude the past history with urolithiasis) and did not take any medicine and did not drank wine or coffee within 1 week before measuring. To compare with the experimental group, the age and the proportion of gender of the control group were selected.
Measurements
The electrical conductance of 24 acupoints in the 12 left meridians and the 12 right meridians were measured with a device (MEAD, the 6th generation, Medpex Enterprises, Taiwan). The meridians are as follows: lung (L, H1), pericardium (P, H2), heart (H, H3), small intestine (SI, H4), triple energizer (TE, H5), large intestine (LI, H6), spleen (SP, F1), liver (LIV, F2), kidney (K, F3), urinary bladder (B, F4), gallbladder (G, F5), and stomach (S, F6) (Fig. 1). The conductivity at the acupuncture point is directly proportional to the amperage of the DC that flows through the skin when 12 V is applied to the points one by one. The conductance values were calculated and expressed as the scale between 0 and 200. The average electrical conductance value of 24 meridians in each subject was calculated. The index of sympathovagal balance was defined as the highest average limb electroconductivity on the dorsal or ventral side, which was divided by the lowest during the MEAD analysis. All procedures were performed in an air-conditioned environment with temperature between 23°C and 26°C. The humidity was also kept constant.
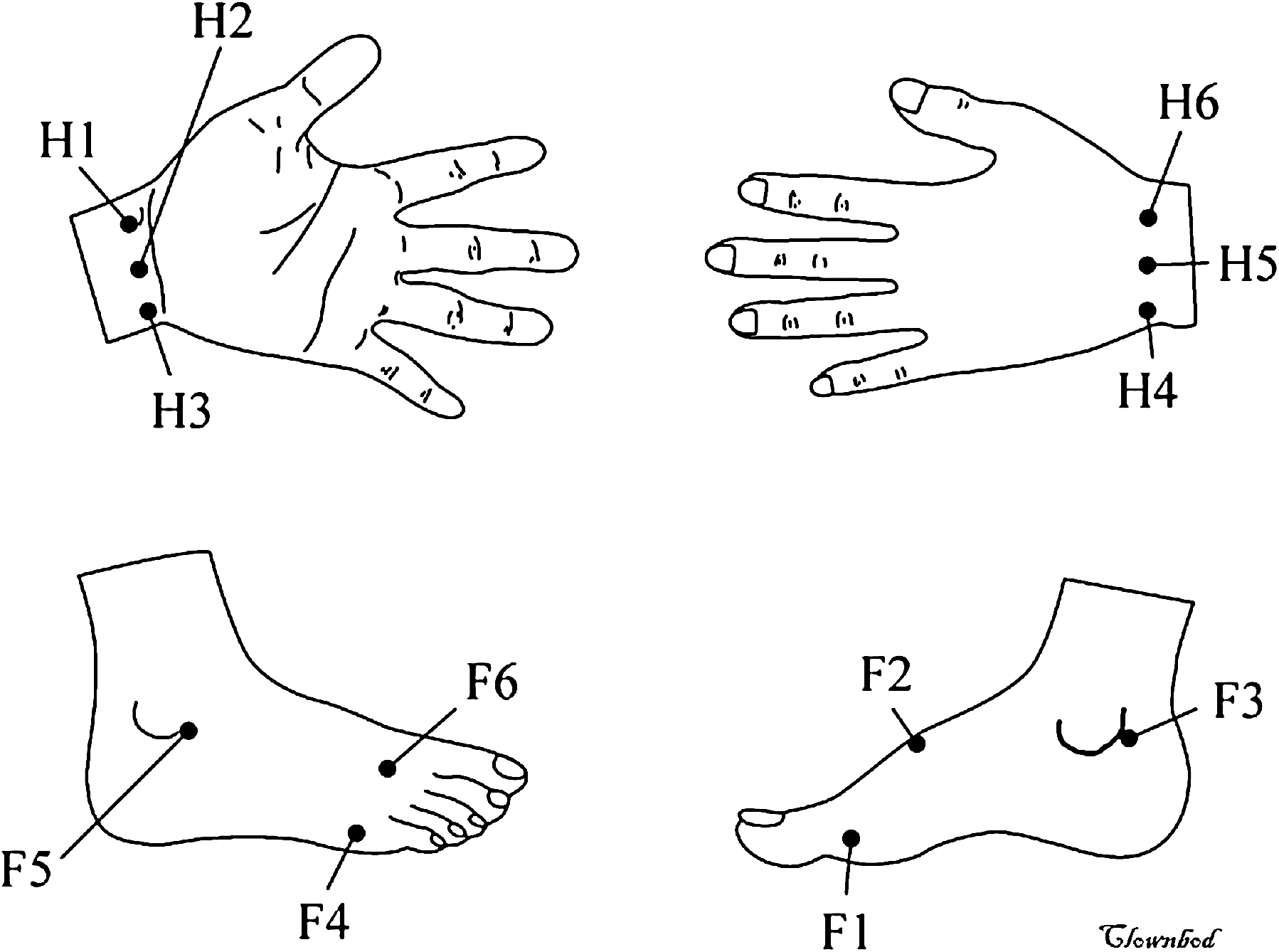
Based on traditional Chinese meridian theory, there are 6 acupoints on each limb (both right and left limbs are symmetric). H1: lung; H2: pericardium; H3: heart; H4: small intestine; H5: triple energizer; H6: large intestine; F1: spleen; F2: liver; F3: kidney; F4: urinary bladder; F5: gallbladder; F6: stomach.
The 10-cm visual analog scale (VAS) was recorded for all patients on the data collection form by the same emergency physician. Ultrasonographic studies were practiced for all patients then. The criteria for hydronephrosis given by Ellenbogen et al. were used. Grade 0 and 1 were classified as normal and mild degree, respectively; grade 2 and 3 were classified as moderate and severe, respectively. 13
Study protocols
Under the ED management, patients with renal colic underwent urinalysis, plain KUB radiography, and renal echo routinely to confirm the diagnosis of ureteral calculus. Patients were asked to rate their pain on a continuous 10-cm VAS at the start of their clinical examination. Additionally, patients were treated with narcotics and intravenous nonsteroidal anti-inflammatory drugs except the VAS was less than 2. Meridian electrical conductance analysis was practiced for all patients. Selective use of IVP was arranged if patients assigned. The outcome was divided into three groups: (1) ureteroscopy, (2) extracorporeal shock wave lithotripsy (ESWL), and (3) discharge with oral medicine. Urological intervention (ureteroscopy and ESWL) was decided by a urologist. Those patients who were discharged with oral medicine accepted a 4-week follow-up (Fig. 2).
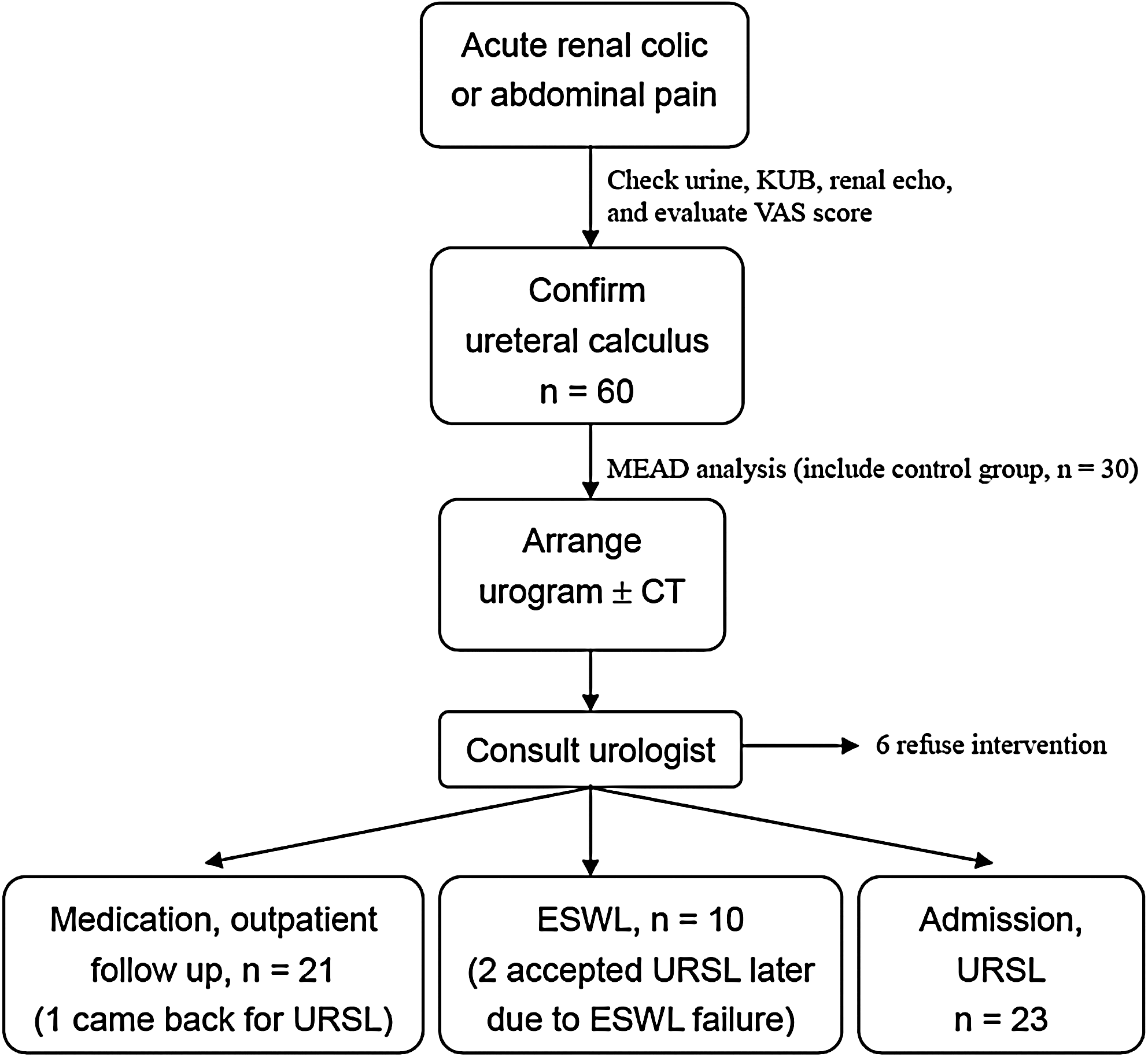
Protocol of the study flow. KUB, kidney–ureter–bladder film; VAS, visual analog scale; MEAD, meridian energy analysis device; CT, computed tomography; URSL, ureteroscopic lithotripsy; ESWL, extracorporeal shock wave lithotripsy.
Data Analysis
Data are presented as mean ± standard deviation or as median and interquartile range (25th–75th percentiles), depending on the distribution of the data. Kolmogorov-Smirnov test was used to determine the normalcy of data distribution. Categorical variables were compared between 2 groups using χ 2 test or Fisher exact test when appropriate, whereas continuous variables were compared using independent-samples t-test for normally distributed data or Mann–Whitney test for non-normally distributed data. Among 3 groups with normally distributed data, analysis of variance was used and the post-hoc method was practiced to see the differences. The Kruskal-Wallis test was used for 3 groups with non-normally distributed data. The variables with univariate comparison p < 0.1 between 2 groups (intervention and discharge with oral medicine) were eligible for inclusion in a forward selection multiple logistic regression model, which identified the clinical factors in the ED that were independent indicators of advanced intervention. The receiver operating characteristic (ROC) curve for the statistically independent electrical conductance (EC) variables associated with intervention was also drawn. A p value less than 0.05 was considered statistically significant.
Results
During the 8-month study period, 60 patients who visited the ED with ureteral calculus and renal colic were enrolled in this study. There were 40 males and 20 females with a mean age of 42.0 ± 12.6 years (range, 23–79 years). In the control group, there were 20 males and 10 females with a mean age of 40.8 ± 11.7 years (range, 23–68 years). The average electrical conductance of the 60 patients was 17.4 ± 12.8 μA (Fig. 3). The index of sympathovagal balance of the patient group was 3.7 ± 2.4. In the control group, average electrical conductance was 48.8 ± 20.1 μA and the index of sympathovagal balance was 2.0 ± 0.5 (Table 1). There were significant differences between these 2 groups.
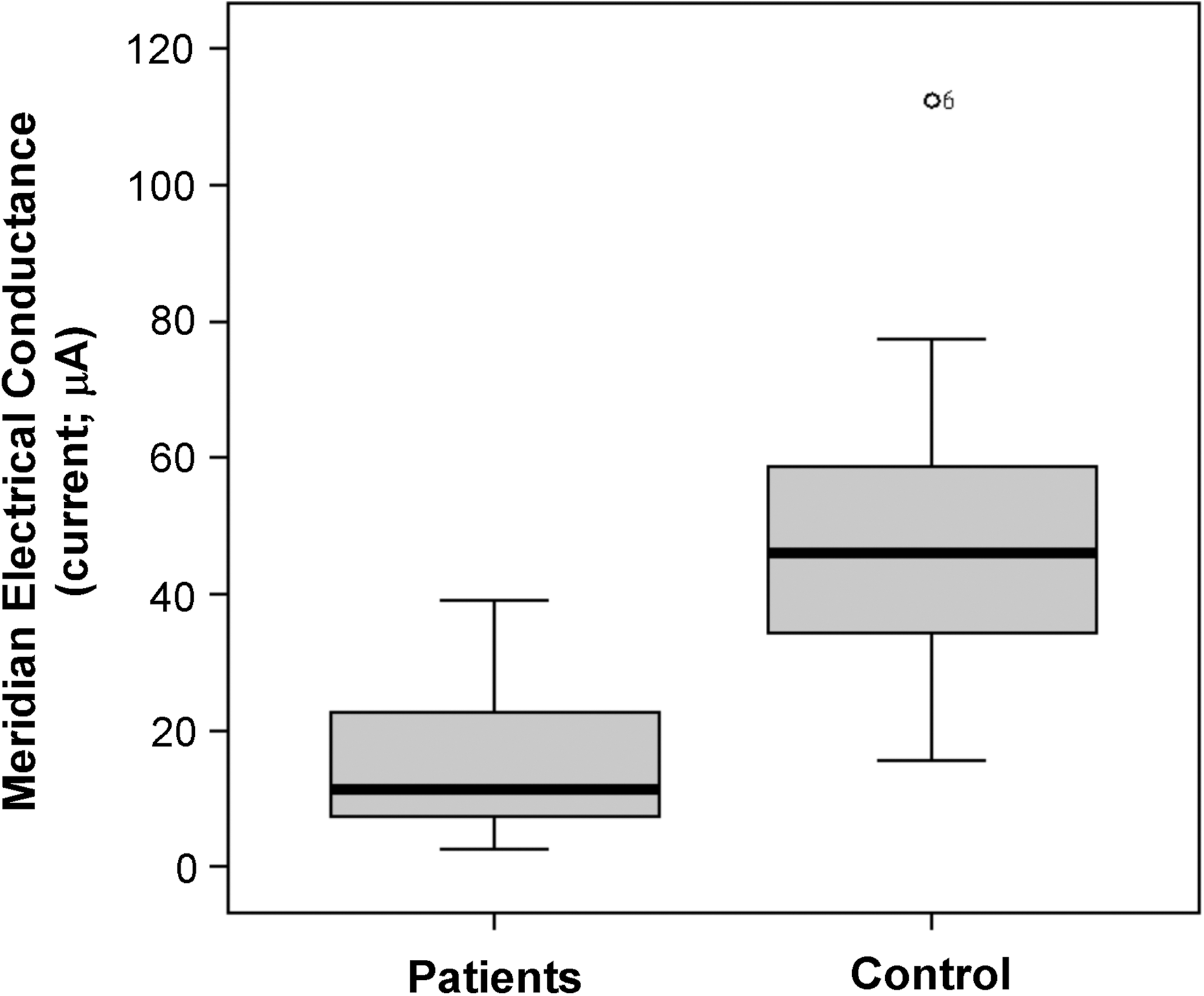
Mean meridian electrical conductance (current; μA) in patients with ureteral calculus and control subjects. p < 0.01.
SD, standard deviation.
The patients diagnosed with ureteral calculus were further studied. There were 6 patients for whom urological intervention was recommended, but they were discharged against advice. Of the 54 patients who were included in the final study, 23 accepted ureteroscopy, 10 accepted ESWL, and 21 were discharged with oral medicine. No patient received open surgery or percutaneous nephrostomy. Among them, 2 patients with ESWL failure later received ureteroscopy and 1 patient who had been discharged with oral medicine came back to accept ureteroscopy during follow-up. In the ESWL group, the stone size ranged from 0.50 cm to 1.59 cm. The patient with 1.59-cm ureteral calculus accepted ureteroscopy 2 days later due to ESWL failure. In the ureteroscopy group, the smallest stone size was 0.30 cm. The intervention group (ureteroscopy and ESWL) had a higher VAS score, grade of hydronephrosis, and autonomic nervous imbalance than the nonintervention group (spontaneous stone passage) (Table 2).
Post-hoc (Scheffe) analysis showed that the oral medicine group had significant difference from the others.
URSL, ureteroscopic lithotripsy; ESWL, extracorporeal shock-wave lithotripsy; ED, emergency department; KUB, kidney-ureter-bladder radiographic film; IVP, intravenous pyelography (urogram); VAS, visual analogue scale; SD, standard deviation.
Multiple logistic regression models showed that the index of sympathovagal balance was a significant independent indicator for patients with renal colic to accept urological intervention. The ROC curve in predicting intervention was constructed, and the area under the curve (AROC) was found to be 0.804 (95% confidence interval [CI], 0.680–0.929). In our study, if the index was more than 3, the odds ratio (OR) for predicting a patient's management was 11.111 (95% CI, 2.925–42.202) (Fig. 4A). In addition, the ROC curve of VAS in predicting urological intervention in patients with ureteral calculus is shown; the AROC is 0.679 (95% CI, 0.529–0.829) (Fig. 4B).
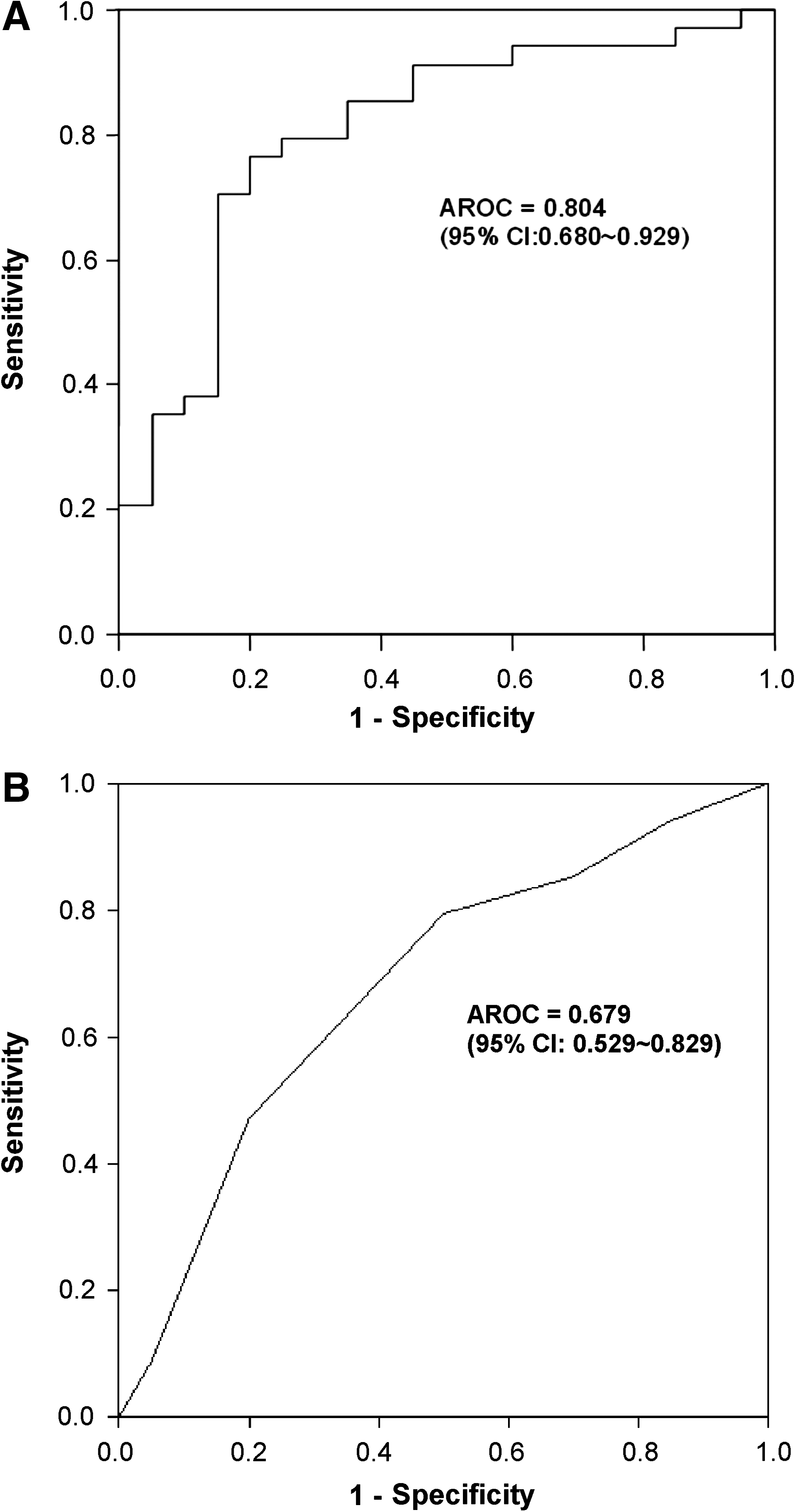
The receiver operating characteristic (ROC) curve of (
Discussion
In our study, renal colic occurred in patients mostly in the early morning (∼63%). These patients had obvious lower electroconductivity and higher index of sympathovagal balance. The index predicts obstructing ureteral calculi with a sensitivity of 73.5%, specificity of 80.0%, positive indication rate of 86.2%, negative indication rate of 64.0%, and accuracy of 75.9%.
Renal colic is commonly observed in the ED. 1 The majority of patients with ureteral calculus present with moderate to severe flank pain. The pain is produced by physical stretching of the nerve endings caused by increasing endoluminal pressure of the urinary tract and by increased tension in the wall of the ureter as a result of ureteral obstruction. 2 Emergency physicians are usually the first to evaluate this condition in the ED. The pain has traditionally been managed with narcotics and nonsteroidal anti-inflammatory drugs. 3 In our study, the most commonly used drugs were pethidine (50 mg/amp, intramuscular [i.m.] or intravenous [i.v.]) and ketorolac (30 mg/amp, i.m. or i.v.). If VAS was above 8, the patients always needed 2 or more pain relieving drugs. Pain relief was often achieved soon after the injection. Although some management guidelines for ureteral calculus have been published and the widespread use of laboratory and imaging studies suggested, there are factors that limit the emergency clinicians from arranging further examination. 5 Some reports have shown that up to 40% of patients with urolithiasis have difficulty passing their calcul. 14 Urgent intervention is needed in a patient with an obstructed ureteral stone. Delayed intervention will increase the risk of acute pyelonephritis and renal damage. 2,5,14
While renal colic is often diagnosed by its clinical presentation and physical examination, urinalysis, initial plain KUB film, ultrasonography, urogram, and/or CT should be used to confirm and evaluate ureteral calculus. 15 The size of the ureteral calculus is a major criterion for intervention. The majority of stones that are more than 5 mm (some literatures recommend ≥ 6 mm) in diameter are difficult to pass spontaneously. 1,2,4,14,15 Some stones are radiolucent, and only about 40% of ureteric stones could be found on the KUB films in the present study. Therefore, physicians should arrange further imaging examinations for patients with invisible calculus if the equipment is available. According to our results, the existence of hydronephrosis can help to decide whose ureteric stones need intervention. All patients with a moderate or severe grade of hydronephrosis needed intervention (100%, 19/19). By contrast, only 40% of patients with a mild or normal grade of hydronephrosis needed intervention (40%, 14/35). Thus, if a patient does not have obvious hydronephrosis, it is difficult for the ED doctors to decide whose condition needs advanced treatment. Additionally, besides ensuring the availability of necessary equipment, it is also important to train the physicians to use them. Moreover, in case a patient has had a recent ureteral calculi attack (often within 1 month), it is difficult to distinguish acute from chronic hydronephrosis during diagnosis. Therefore, sonography has its limitations in the accurate diagnosis of ureteral calculi by emergency physicians.
Previous studies have shown that VAS could be used to predict intervention in renal colic patients during their admission to the ED. 2,14 In the present study, the AROC of VAS that could be indicative of urological intervention in patients with ureteral calculus was 0.679 (95% CI, 0.529–0.829), suggesting that the index of sympathovagal balance is superior to VAS. In addition, VAS score is subjective and has some interfering factors. The MEAD could be used to obtain patient information more objectively since it is noninvasive, economical, and easy to use. In 1949, a research group found that abnormalities or diseases of the viscera were reflected in measurable changes of bioelectric current. In 1956, after further advancement and study with source points and bioelectric currents, the famous Ryodoraku theory was published. 11 The sweat gland is a target organ of the peripheral autonomic system and is innervated by cholinergic fibers. Increased intradermal acetylcholine causes the glands to secrete sweat, which in turn leads to an increase in skin electrical conductance and a decrease in skin resistance. By measuring skin resistance, the peripheral autonomic innervations can be evaluated indirectly. The obvious advantage of the neurometer is its noninvasiveness.
Many previous studies have shown that the nervous system is somehow related to the meridian system. 6,8 A healthy body function often has a good conductivity of heat or electrical energy. 16 Our study is the first to demonstrate that the measurement of meridian electrical conductance could be a means of evaluating how the meridian, and therefore the nervous system, is related to renal colic. In that case, skin electrical resistance, skin moisturization, and subskin tissue water content could be important during measurement. 11
Patients with acute renal colic have high sympathetic activity in the body. Although patients accepted pain control initially, the phenomenon persisted for hours. 17 This result showed that the index of sympathovagal balance, especially the index ≥3, was a significant independent indicator for patients with renal colic to accept urological intervention (OR = 11.111). In summary, we recommend using the following parameters to identify those renal colic patients who require intervention after evaluation in the ED: (1) if the size of the calculus is ≥10 mm and hydronephrosis exists, ureteroscopic intervention is suggested; (2) if the size of the calculus is between 5 mm and 10 mm and the index of sympathovagal balance is ≥3, intervention should be considered. Either ESWL or ureteroscopic lithotripsy should be selected after urologist consultation; (3) if the calculus is invisible or of smaller size, but the index of sympathovagal balance is ≥3, advanced imaging studies (intravenous urography or unenhanced helical CT) need to be arranged. Further intervention may be considered if the ureteral calculus cannot be passed spontaneously; (4) if renal colic patients have small calculi and low index of autonomic imbalance, they can be discharged and provided with a urological follow-up for 4 weeks.
Recent studies have demonstrated the advantage of noncontrast helical CT. 18 CT detects obstructing ureteral calculi with a sensitivity of 98%, a specificity of 100%, and positive and negative indication rate of 100% and 97%, respectively. 2 We cannot substitute meridian energy analysis for the role of CT because the index has lower sensitivity and specificity than CT. However, the disadvantages of CT are its higher cost, ionizing radiation, and lack of time in some institutions. Because the MEAD is easy in practice, it can be used to evaluate renal colic patients first.
In our study, about 30% patients had the prior stones. However, further metabolic evaluation should be undertaken. The patients should be encouraged to drink enough fluid to prevent renal colic again and irreversible renal damage.
Conclusions
The measurement of electrical conductance, especially the index of sympathovagal balance, may be used as a valuable complementary diagnostic method for selective intervention in patients with acute colicky pain. Imaging studies and ultrasonography combined with electrical conductance analysis provides physicians with important information for judging the patient's condition. The index of sympathovagal balance could be a good indicator of urological intervention in patients with ureteral calculi in the ED. This would result in reduced health care costs due to fewer complications, ED visits, and unnecessary referrals. Nevertheless, extensive large-scale clinical trials are warranted and should be encouraged.
Footnotes
Acknowledgments
This study was supported by the National Science Council, Taiwan, NSC97-2320-B-039-022-MY3 and NSC98-2815-C-039-097-B; China Medical University CMU97-267, CMU97-279, and CMU98-CT-10. The authors thank Miss Yi-Chun Chang for technical assistance in manuscript preparation.
Disclosure Statement
No competing financial interests exist.