
Abstract
Objectives:
Two of the most pressing public health challenges in the United States are treating human immunodeficiency virus (HIV) infection and illegal substance use. High rates of complementary and alternative medicine (CAM) use have been reported by individuals who suffer from both of these diseases. The goal of this study was to examine the relationship between CAM use and illegal substance use in a cohort of women with HIV or at risk for HIV disease. Based on previous research, it was hypothesized that CAM use may decrease substance use.
Design:
This was a longitudinal cohort study.
Subjects:
The subjects comprised Women in the Women's Interagency HIV Study.
Outcome measures:
The role of CAM use in illegal substance use was examined. Due to the hierarchical structure of the dataset, logistic regression analysis adjusting for repeated measurements (generalized estimating equation model) was carried out to assess associations of CAM use and illicit drug use.
Results:
There were 2176 women included in the analysis. After excluding for marijuana use, CAM use was associated with less drug use (odds ratio 0.82; 95% confidence interval: 0.73, 0.90).
Conclusions:
The results supported our hypothesis that CAM users are more health conscious and thus less likely to use illicit drugs. Future studies should target both specific drugs and CAM modalities to help finalize this association.
Introduction
High rates of CAM use have been reported by individuals who use illegal drugs. One large survey of intravenous drug users found that 45% also used CAM modalities. 12 Clinical trials have examined the role of specific CAM modalities in reducing substance abuse, including acupuncture in treating cocaine abuse, magnesium in reducing opiate use, and transcranial magnetic stimulation in treating nicotine dependence. 13 –17 However, the findings of these studies are inconsistent, and definitive conclusions about CAM use in drug abuse cannot be reached.
In previous research in the Women's Interagency HIV Study (WIHS), CAM users were found to demonstrate health-seeking behaviors and a tendency to utilize increased health services. 18,19 The goal of this study was to examine the relationship between CAM use and illegal substance use.
Materials and Methods
Study design
The WIHS was designed to examine the natural and treated history of HIV disease among women in response to its rising epidemic in 1994–1995. Its study design is detailed elsewhere. 20 The original enrollment recruited 2054 HIV-infected and 569 HIV-uninfected women from six study sites (Chicago, Los Angeles, San Francisco, Washington, DC, Brooklyn, and the Bronx) around the United States. Women visited a study site every 6 months; during each visit, structured interviews were performed to collect data on sociodemographic characteristics, substance use and sexual behaviors, health care utilization, antiretroviral therapy, other treatments, and disease outcomes. In addition, physical and obstetric/gynecologic examinations were performed by the medical staff and biological specimens collected. The local institutional review board at each site approved the study protocol, and all women gave their written informed consent. In the WIHS, comprehensive information on CAM use was collected annually (at only odd-numbered visits) from study enrollment until March 2002.
Variable definitions
Outcome variables
Information about substance use has been asked about from the start of WIHS and is ongoing. At study enrollment, participants were asked if they had ever used illicit drugs in their life. Frequency of illicit drug use in the previous 6 months was assessed at each study visit. Participants who used any illicit drugs including marijuana, cocaine, crack, opium, heroin, methadone, amphetamine, and methamphetamine were considered as substance users. During each visit, participants were asked questions regarding their illicit drug use as, “Since your (MONTH) study visit, have you used (any illicit drug name)?”
Independent variables
For each of the CAM treatment approaches, participants were asked whether they had used that approach at least once in the past 6 months. CAM use was divided into three categories: ingestible CAM medication (herb medications and nonherb medication), body practice, and spiritual healing. Ingestible CAM medication reported in this study included St. John's Wort (Hypericum perforatum), coenzyme Q10, melatonin, herbs (Chinese/Asian, Native American, South American, Indian/Ayurvedic), cat's claw, chamomile, combination Chinese herbs, dandelion, Echinacea (with or without goldenseal), garlic, ginkgo (Ginkgo biloba), ginger, ginseng, goldenseal, milk thistle, valerian, woodroot, evening primrose oil, red clover, black cohosh, dehydroepiandrosterone, niacin, N-acetyl-cysteine, glutamine, acidophilus, alfalfa, algae (blue algae, blue–green algae), aloe vera, astragalus (Astragalus membranaceus), bee pollen, β-carotene, chromium, cranberry, megadose vitamins, omega-3-type oils, protein powder, spirulina, thymus glandular, zinc, lecithin, cod liver oil,
CAM was defined for this analysis in three different ways: (1) whether the participant used any CAM; (2) classified into three CAM categories (i.e., ingestible medication, mind–body practice, and spiritual healing practice; and (3) by number of CAM categories.
Covariates
Covariates possibly affecting illicit drug use were selected based on prior research, such as quality of life measurements, sociodemographic variables include age at visit, race, education, income, employment, and insurance. Education achievement at study enrollment was coded as less than high school, completed high school, and college and above. Annual gross income was dichotomized at the poverty line (≤$12,000 per year). Age was measured in 10-year intervals. Clinical variables included HIV status, HIV viral load, CD4+ T-cell counts, and antiretroviral therapy (non–highly active antiretroviral treatment [HAART] or on HAART). HAART was defined according to Department of Health and Human Services/Kaiser Family Foundation guidelines. 21 The viral load was dichotomized as ≥80 copies/mL versus <80 copies/mL. Self-reported symptoms of depression were measured using the 20-item Center for Epidemiological Studies Depression Scale, 22 with a total score of ≥16 used to define the presence of depressive symptoms.
Statistical methods
Due to the hierarchical structure of the WIHS longitudinal data, logistic regression analysis adjusting for repeated measurements (generalized estimating equation model) was carried out to assess associations of CAM use and illicit drug use, and adjusted odds ratio and their 95% confidence intervals were obtained. Univariate models were fit first for variables selected, and only variables significant in the univariate models were included in the multivariate models to examine the impact of CAM use on illicit drug use. Illicit drug use was defined as any illicit drug use reported at the visit. Fitted probabilities of CAM use, type of CAM categories, number of CAM categories, and illicit drug use were estimated using logistic regression. All analyses were conducted using SAS (version 9.2, Cary, NC).
Results
Characteristics of study population
There were 2176 women who enrolled in the WIHS between 1994 and 1995 and had CAM use visits; characteristics of these participants are described in Table 1. The different CAM categories were relatively stable over visits, as shown in Figure 1. At baseline, 52% of all women were CAM users, 30% were ingestible CAM users, 21% body users, and 37% were spirit users. Among all study visits, 51% were CAM users, 29% were ingestible CAM users, 22% were body users, and 34% were spirit users. At study baseline, 79% women were HIV positive. Their median age was 36 years, and 52% of them were black, non-Hispanic. As shown in Table 1, at baseline, 30% of non–drug users were employed compared to 16% of users (p < 0.0001), and illicit drug users had 63% depression rates compared to 49% in nonusers (p < 0.0001).
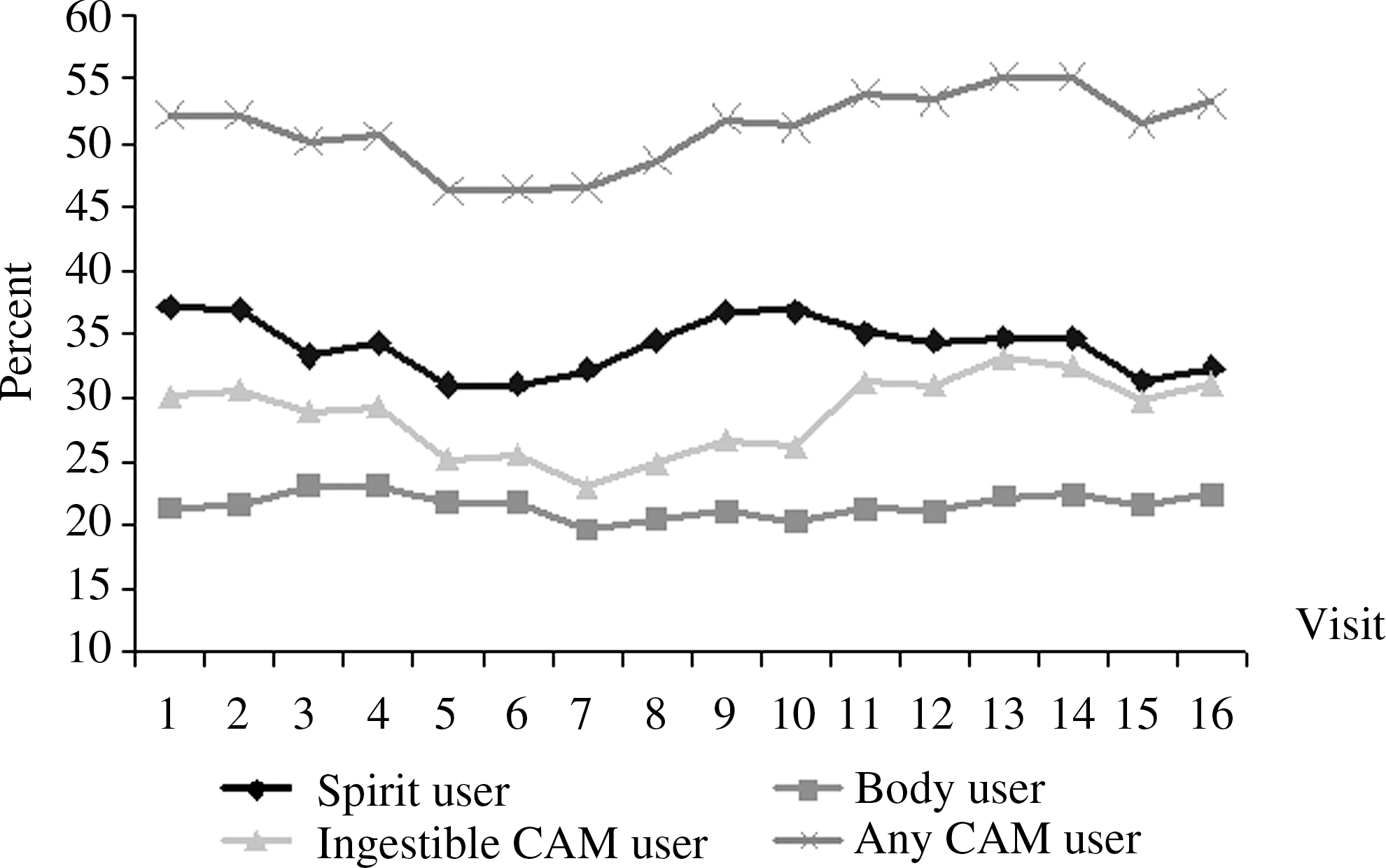
Complementary and alternative medicine (CAM) use among Women's Interagency HIV Study women, October 1994–October 2002.
Some variables have missing values.
All p-values <0.05 except insurance status.
Center for Epidemiologic Studies–Depression ≥16.
IQR, interquartile range; HIV+, human immunodeficiency virus positive.
Multivariate analysis
In the multivariate analyses where all drug use was combined, the only significant outcome was a 10% greater chance of drug use in individuals who used body practice modalities (odds ratio [OR]: 1.10; 95% confidence interval [CI]: 1.01, 1.20) Table 2. However, it appears that marijuana use was the major cause, as when marijuana use was excluded, CAM use is associated with less drug use. For example, any CAM use is associated with 19% less chance of drug use (OR: 0.81; 95% CI: 0.73, 0.90). Additionally, using three CAM categories was associated with a 33% lower chance of drug use (OR: 0.67; 95% CI: 0.54, 0.83). There were no changes in results when examined by HIV status (data not shown).
Covariates, age at visit per 10 years, depression, race, HIV status, employment status, quality of life, income level, and insurance status.
CI, confidence interval; CAM, complementary and alternative medicine.
Discussion
The relationship between CAM use and illegal substance use in this cohort was examined. It was hypothesized that CAM users may be more health conscious and thus less likely use illicit drugs; interestingly, this association among drug users existed if marijuana users were excluded. When marijuana was included, a small association among body practice and drug use was found, but in the opposite direction.
Previous research has examined the role of drug abuse in HIV care, primarily focusing on medical adherence and the role of HIV disease progression among drug users. 23 –25 A previous study in WIHS found individuals in drug abuse programs were more likely to report adherence to antiretroviral medications. 26 Additionally, another WIHS study found that women who abused alcohol had lower levels of adherence. 27 Both of these studies are consistent with the hypothesis that health-conscious patients will use CAM modalities and fewer illicit drugs. In fact, individuals who used all three CAM categories had a 33% less chance of illegal substance use.
Marijuana is widely accepted as a complementary or alternative modality for a variety of diseases. 28 –30 Thus, it is not surprising that marijuana use associates differently than other drug use, as marijuana use is often considered a CAM modality, while the other illegal drugs are not. Initially marijuana users were included, as were all illegal drugs; however, it was excluded in the second model to better examine the role of CAM use on more traditional drugs of abuse.
Research results are divided about the role of CAM in traditional medical compliance. 31 –35 Furthermore, it is difficult to combine different CAM modalities in one analysis. This issue was addressed by using various CAM categories; nonetheless, many different types of CAM exist within each category, and may have different effects on drug use. Further research will need to clarify these CAM and drug categories to better examine their association with each other.
This study had some limitations that deserve mention. First, self-reported CAM and drug use data were used, both of which are sensitive medical issues that participants may not have felt comfortable disclosing. However, the relationships between the WIHS participants and their interviewers have been built on trust and respect over many years, which allows sensitive information to be obtained. Thus, previous WIHS research has shown that self-reported medication use is consistent with objective measures of HIV outcome, such as CD4+ T-cell count, HIV viral load, and self-reported physical functioning, 36 and that self-reported substance use has a high degree of validity using a toxicology analysis for cocaine and opiates on a subset of WIHS participants. 37 Also, participants used a variety of CAM modalities with low frequency of specific modalities. By combining CAM modalities into CAM categories, some of the specificity that specific modalities might have allowed were lost. Due to the nature of the cohort analyses, it often takes substantial time to acquire a large enough sample size and thus these data are nearly 7 years old. Additionally, there may be some unmeasured but important variables not included in the analyses.
Conclusions
HIV-infected women and women at risk of HIV in the WIHS had a high prevalence of CAM use, and this use was associated with less illegal substance use. The increasing interest in using specific CAM modalities in treating substance abuse makes studying the role of CAM in abuse important for future research. Additionally, the role marijuana plays in these individuals deserves further investigation.
Footnotes
Acknowledgments
Data in this article were collected by the Women's Interagency HIV Study (WIHS) Collaborative Study Group with centers (Principal Investigators) at New York City/Bronx Consortium (Kathryn Anastos); Brooklyn, NY (Howard Minkoff); Washington DC Metropolitan Consortium (Mary Young); The Connie Wofsy Study Consortium of Northern California (Ruth Greenblatt); Los Angeles County/Southern California Consortium (Alexandra Levine); Chicago Consortium (Mardge Cohen); Data Coordinating Center (Stephen Gange). The WIHS is funded by the National Institute of Allergy and Infectious Diseases (UO1-AI-35004, UO1-AI-31834, UO1-AI-34994, UO1-AI-34989, UO1-AI-34993, and UO1-AI-42590) and by the National Institute of Child Health and Human Development (UO1-HD-32632). The study is co-funded by the National Cancer Institute, the National Institute on Drug Abuse, and the National Institute on Deafness and Other Communication Disorders. Funding is also provided by the National Center for Research Resources (UCSF-CTSI Grant Number UL1 RR024131). The contents of this publication are solely the responsibility of the authors and do not necessarily represent the official views of the National Institutes of Health.
Disclosure Statement
No competing financial interests exist.