
Abstract
Despite significant advances and development of novel anti-emetics, nausea and vomiting (emesis) is a major side-effect of cancer chemotherapy. At times, severe nausea and vomiting may also lead to reduction in adherence to the treatment regimen, and this will concomitantly affect the patient's survival. The rhizome of Zingiber officinale, commonly known as ginger, is globally an important spice. It has been used for centuries in the Indian, Chinese, Arabic, Tibetan, Unani, and Siddha systems of traditional medicine to treat nausea and vomiting induced by different stimuli. Preclinical studies with experimental animals (dogs and rats) have shown that the various extracts of ginger and the ginger juice possess anti-emetic effects against chemotherapy-induced nausea and vomiting. Gingerol, the active principle, is also shown to possess anti-emetic effects in minks. However, with regard to humans, while most studies have been supportive of the preclinical observations, a few have been contradictory. The exact mechanism responsible for the anti-emetic effects of ginger is unknown; however, the ginger phytochemicals, especially 6-gingerol, 8-gingerol, 10-gingerol, and 6-shogaol, may function as a 5-hydroxytryptamine (5-HT3) antagonist, NK1 antagonist, antihistaminic, and possess prokinetic effects. The present review for the first time attempts to address the anti-emetic observations and the variability in response of the anti-emetic effects of ginger in cancer chemotherapy. An attempt is also made to address the lacunae in the published studies and emphasize aspects that need further investigations for ginger to be of use in clinics as an anti-emetic agent in the future.
Introduction
Ginger, scientifically known as Zingiber officinale Rosce, is an important spice in the various Asian types of cooking. Ginger has a long history of medicinal use, and the literature suggests that it has been used as a medicinal agent for nearly 2500 years. Ginger is an integral part of the various traditional and folk systems of medicine in China and India for conditions such as headaches, colds, respiratory and rheumatic disorders, arthritis, bronchitis, muscle pains, fever, infectious diseases, constipation, and asthmatic respiratory disorders. 3 –7 Ginger is also a household medicinal agent and is widely used for dyspepsia, flatulence, abdominal discomfort, and nausea. It has been recommended for use as a carminative, diaphoretic, antispasmodic, expectorant, peripheral circulatory stimulant, astringent, appetite stimulant, anti-inflammatory agent, diuretic, and as a digestive aid. 3,4
Ginger contains several phytochemicals, the most important groups of which are the nonvolatile and volatile compounds. Upon extraction, pungent, nonpungent, and an essential oil fraction are obtained from the nonvolatile fraction. The sequesterpene derivatives such as zingiberene, curcumene, β-sesquiphelandrene, and β-bisabolene are responsible for the aroma and form a major part of the volatile fraction, while the monoterpene derivatives α-pinene, β-lemene, farnesene, β-phelandrene, myrcene, β-pinene and sabinene are in lower concentrations. The nonvolatile pungent phytochemicals of ginger consists of the biologically active components, predominated by gingerols, shogaols, paradols, and zingerone (Fig. 1). These compounds are responsible for the warm, pungent sensation in the mouth. Because of the presence of a β-hydroxy keto group, gingerols are thermally labile and readily undergo dehydration to form the corresponding shogaols. Shogaols may be further converted to paradols by hydrogenation and are similar to gingerol. The major pharmacologic activity of ginger appears to be due to gingerol and shogaol, and the relative proportions of gingerols, shogaols, and paradols in ginger extracts are determined by a number of factors, including the geographic origin, the maturity of the rhizomes at the time of harvest, and the method by which the extracts are prepared. 3 –7
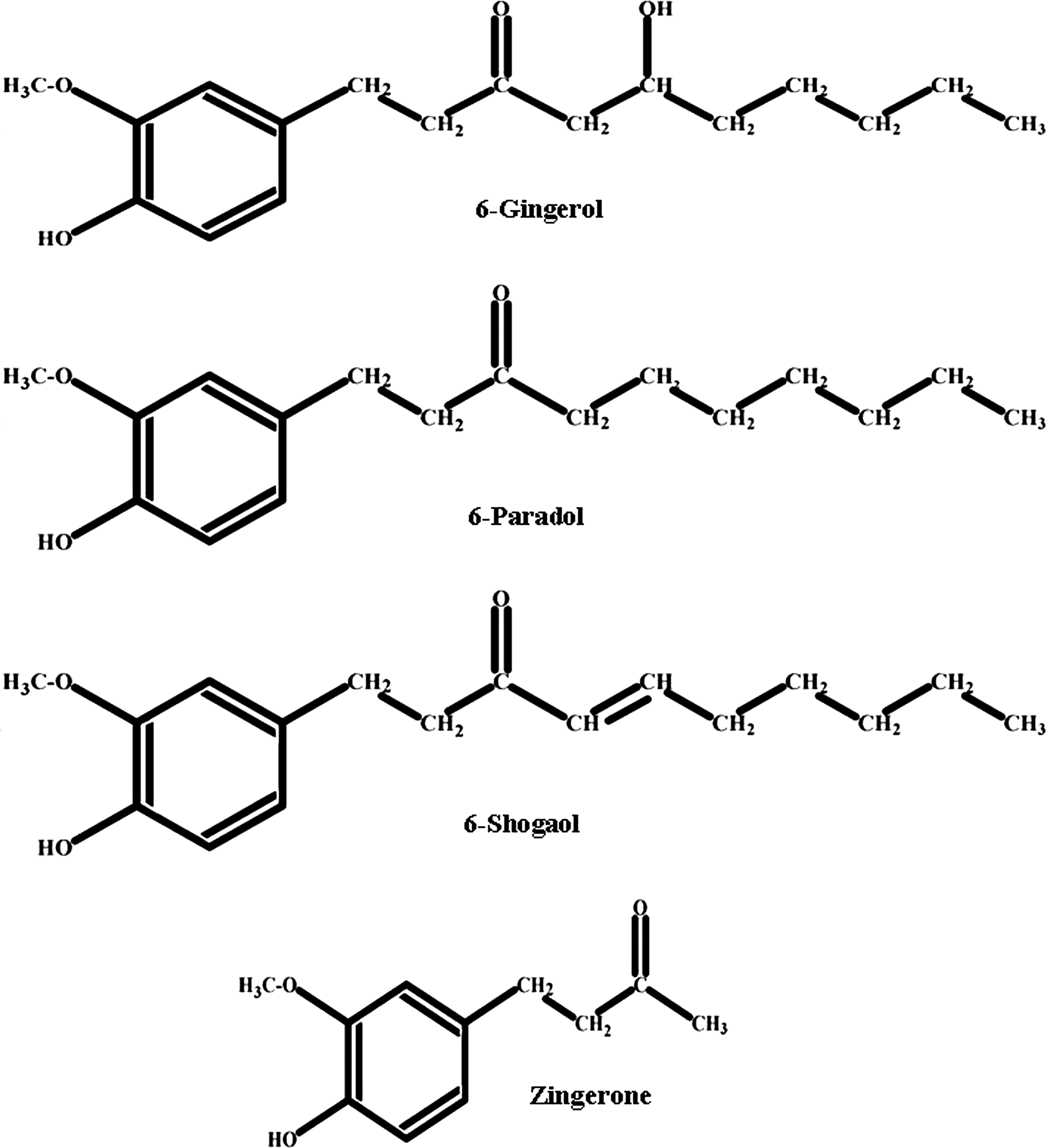
Important phytochemicals present in ginger.
Ginger as an Anti-Emetic Agent
Ginger has been also used to treat gastrointestinal disorders, mainly nausea and vomiting associated with abdominal spasm, motion sickness, and pregnancy. 3,4 In Traditional Chinese Medicine, a distinction is made between the fresh and dried root of this plant. The fresh root (Sheng Jiang) is particularly used to treat nausea and vomiting, although the dried root (Gan Jiang) can be used for this purpose as well. Clinical studies have shown that ginger possesses an anti-emetic effect in many circumstances such as morning sickness, 8 sea sickness, 9 in pregnancy, 10 postoperatively, 11 –14 and in motion sickness. 15 Preclinical studies suggest that ginger is effective in preventing cisplatin-induced emesis in mongrel dogs 16 as well as gastric emptying in rats. 17 However, pilot clinical studies in patients with cancer have been mixed. In the following paragraphs, a brief summary on the various studies with ginger in the prevention of radiation and chemotherapy-induced emesis is given.
Ginger in the Prevention of CINV: Animal Studies
Studies with mongrel dogs have shown that the acetone, 50% ethanolic, and aqueous extracts of ginger (25, 50, 100, and 200 mg/kg body weight
Studies have also shown that the hydroalcoholic extract of ginger (150, 200, 250, 300 mg/kg body weight) mitigated the γ−radiation-induced conditioned taste aversion in Sprague-Dawley rats and that a sex dichotomy existed. Intraperitoneal administration of the ginger extract 1 hour before 2-Gy γ−irradiation was effective in blocking the saccharin avoidance response for 5 post-treatment observational days. A concentration- and time-dependent protection was observed and the optimal effects were observed at 200 and 250 mg/kg body weight for the male and female rats, respectively. 19,20 The effect of ginger was comparable to that of the standard anti-emetic drugs ondansetron and dexamethasone. 20
Clinical Studies
With regard to human studies, the efficacy of ginger in preventing the CINV has been contradictory. In one of the earliest studies, Pace 21 reported that ginger was effective in reducing CINV in patients with leukemia. The patients were randomized to receive oral ginger or placebo in addition to prochlorperazine. The results showed that when compared to those receiving placebo, a significant reduction in nausea was observed in patients receiving ginger. 21 Later studies by Meyer et al. 22 and Pecoraro et al. 23 have also supported the use of ginger as an anti-emetic agent in patients undergoing chemotherapy.
Manusirivithaya et al. 24 performed a randomized, double-blinded crossover study in 48 patients with gynecologic cancer receiving cisplatin-based chemotherapy. All patients received standard anti-emetics in the first day of cisplatin administration, and the patients were grouped into two cohorts. One (1) group received capsules of ginger root powder orally 1 g/day for 5 days, starting on the first day of chemotherapy, while in the other group placebo was given on the first day and metoclopramide was given orally thereafter for 4 days. The patients were then crossed over to receive the other anti-emetic regimen in their next cycle of chemotherapy. 24
At the end of the study period, of the 43 evaluable patients who received both cycles of treatment, success in controls of nausea and emesis were not significantly different between the two regimens in both acute and delayed phases. However, in the cohorts that received metoclopramide, restlessness was a conspicuous side-effect and occurred frequently when compared to the cohorts that had received ginger. The present study showed that addition of ginger to a standard anti-emetic regimen has no advantage in reducing nausea or vomiting in acute phase of cisplatin-induced emesis and also that in the delayed phase, ginger and metoclopramide have no difference in their efficacy. The authors suggest that ginger was effective in the delayed phase, is devoid of ill effects, and that a larger clinical trial is necessary. 24
In a randomized, crossover, double-blind study with 50 patients, Sontakke et al. 25 also observed that oral administration of ginger (1000 mg) 20 minutes before chemotherapy and 6 hours after chemotherapy was effective in preventing emesis induced by the chemotherapeutic regimen containing cyclophosphamide in combination with other chemotherapeutic agents. All patients in the study received cyclophosphamide (500–1000 mg IV) and the interval between two successive cycles was 21 days. The investigators randomly assigned the patients to receive either ginger or metoclopramide or ondansetron during the first study cycle. They were then crossed over to the other anti-emetic treatments during the next two successive cycles. At the end of the study, the investigators observed complete control of nausea in 62% of patients on ginger, 58% with metoclopramide, and 86% with ondansetron. Complete control of vomiting was achieved in 68% of patients on ginger, 64% with metoclopramide, and 86% with ondansetron. Ginger was observed to be devoid of any adverse effects, suggesting that it is safe and effective. 25
In support of these observations, Levine et al. (2006), in their study with 28 patients with cancer receiving emetogenic cytotoxic agents, have also observed that combining a protein-rich diet (protein drink ProSure®; 15 g protein) and 1 g of dried ginger root twice daily decreased the delayed nausea of chemotherapy, and reduced the use of anti-emetic medications when compared to the cohorts receiving only the protein diet. The combination of anti-nausea effects of high-protein meals with ginger enhanced the normal gastric myoelectrical activity and decreased gastric dysrhythmias. 26 Very recently, Pillai et al. 27 have also observed that ginger root powder was effective in reducing the severity of acute and delayed CINV when provided as a adjunct to ondensetron and dexamethasone in patients with bone sarcoma receiving the highly emetogenic chemotherapy containing cisplatin/doxorubicin. Together these reports clearly suggest the usefulness of ginger as an adjuvant to the conventional anti-emetic agents.
However, contradicting observations have been reported recently by Zick et al. 28 The investigators evaluated the efficacy of ginger in preventing delayed CINV by performing a randomized, double-blind, placebo-controlled trial in 162 patients receiving 5-hydroxytryptamine (5-HT3) receptor antagonists and/or aprepitant. Participants were randomized to receive either 1.0 g ginger, 2.0 g ginger daily, or matching placebo for 3 days. The authors observed that ginger provided no additional benefit for reduction of the prevalence or severity of acute or delayed CINV when given with 5-HT3 receptor antagonists and/or aprepitant. 28
Mechanistic Studies
The exact mechanism responsible for the anti-emetic effects of ginger is unknown. However, studies suggest that the ginger phytochemicals 6-gingerol, 8-gingerol, 10-gingerol, and 6-shogaol may function as a 5-HT3 antagonist, NKI antagonist, and have antihistaminic and prokinetic effects. 29 In vitro studies with N1E-115 cells expressing 5-HT3 receptors showed that these phytochemicals caused a concentration-dependent inhibition of the 14 C-guanidinium influx through 5-HT3 receptor channels. 29 These phytochemicals also inhibited the SR57227A (4-amino)-(6-chloro-2-pyridyl)l-piperidine hydrochloride)-induced contractions of the guinea-pig ileum and the potency was as follows: [6]-shogaol≥[8]-gingerol>[10]-gingerol≥[6]-gingerol. These compounds were observed to possess weak anticholinergic and antineurokininergic activities in the guinea-pig ileum. The authors suggest that these phytochemicals exert their anti-emetic effect at least in part by acting on the 5-HT3 receptor ion-channel complex, probably by binding to a modulatory site distinct from the serotonin binding site and also that this may include the indirect effects via receptors in the signal cascade behind the 5-HT3 receptor channel complex such as substance P receptors and muscarinic receptors 29 (Fig. 2). Studies have also shown that 6-gingerol enhanced gastrointestinal motility and possessed antihydroxytryptamine activity in isolated guinea pig ileum. 8 It also caused a dose-dependent suppression and decrease in the levels of NK1 receptor in both the ileum and area postrema of minks treated with cisplatin. 18 Galanolactone, a diterpinoid isolated from ginger, is also reported to be a competitive antagonist at ileal 5HT3 receptors. 8 Additionally, the volatile oil and the ginger compounds terpinolene, β-pinene, and α-phellandrene are also reported to interact with 5-HT3 receptor and to possess antispasmodic effect on the rat ileum. 30 Together, all these observations indicate that ginger possesses the effect of both ondensatron and domperidone, and is beneficial in reducing CINV.
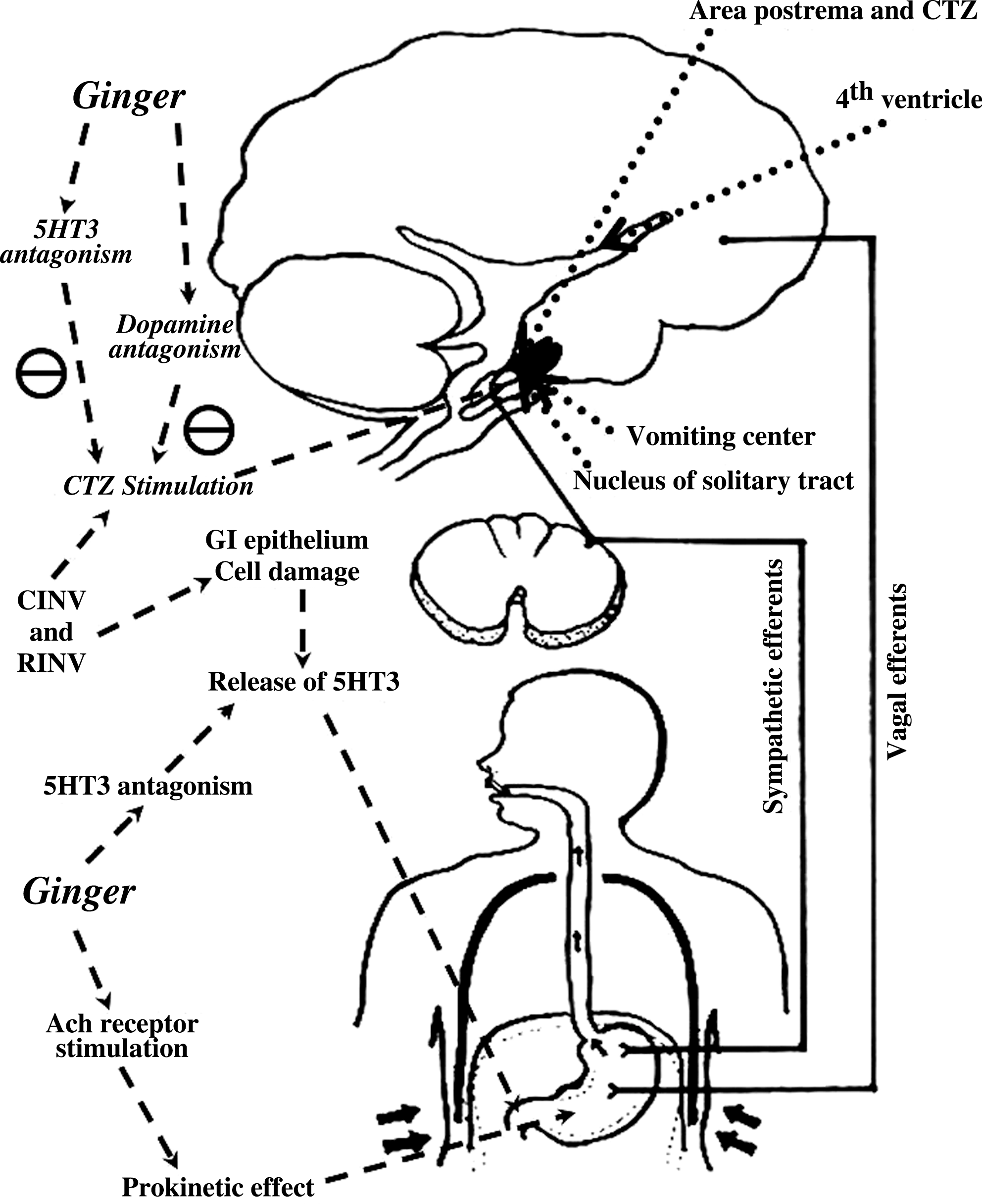
Mechanisms responsible for the prevention of chemotherapy-induced nausea and vomiting (CINV) in ginger. Slashed circles signify “inhibit.” 5-HT3, 5-hydroxytryptamine, CTZ, chemoreceptor trigger zone; GI, gastrointestinal; RINV, radiotherapy-induced nausea and vomiting.
Conclusions
Preclinical studies have shown that ginger is effective as an anti-emetic agent and that it possesses 5HT3 antagonistic activity, which is responsible for reducing CINV. Its prokinetic activity makes it similar to metaclopramide minus the extrapyramidal adverse effects. Together these reports indicate that ginger is a promising anti-emetic herbal remedy. However, the clinical data are insufficient to draw firm conclusions. Studies should be planned with a large number of patients receiving radiotherapy and chemotherapeutic agents with different emetogenic profiles.
The pharmacologic activity of ginger appears to be due to gingerol, paradols, and shogaol. The final ratio of these compounds in ginger is determined by a number of factors, including the geographic origin, the maturity of the rhizomes at the time of harvest, and the method by which the extracts are prepared. The gingerols are thermally labile and readily undergo dehydration to form the corresponding shogaols. The extent of this conversion is likely to have a significant impact on the medicinal benefits of ginger, as the two compounds vary in their bioavailability, pharmacokinetics, and pharmacologic properties.
The opposing results observed with human studies on anti-emetic effects against CINV may be due to the variations in the bioactive compounds, because these studies were performed in different countries. In view of these observations, it is imperative that a quality control be established for the presence of active phytochemicals in the varieties of ginger used in experiments. The availability of metabolite standards for quantification of the important phytochemicals will make the study more reliable and reproducible. Additionally, preclinical studies should also be performed to understand the efficacy of important phytochemicals as anti-emetics.
Due to its abundance, low cost, and safety in consumption, ginger remains a species with tremendous potential and countless possibilities for further investigation. Ginger has the potential to develop as a nontoxic anti-emetic agent against chemotherapy and radiation-induced nausea, when gaps existing in knowledge are bridged. The outcomes of such studies may be useful for the clinical applications of ginger in humans against cancers and may open up a new therapeutic avenue. In addition to its anti-emetics effects, ginger is observed to possess chemopreventive, radioprotective, and cytoprotective effects against doxorubicin-induced nephrotoxicity and testicular toxicity. All these beneficial effects will also ameliorate the radiation- and chemotherapy-induced adverse effects.
Footnotes
Acknowledgments
The authors RH, PLP, and MSB are grateful to Rev. Fr. Patrick Rodrigus (Director), Rev. Fr. Denis D'Sa (Administrator), and Dr. Jaya Prakash Alva (Dean) of Father Muller Medical College for providing the necessary facilities and support. AGR is thankful to Dr. Kumar and Dr. Sarswathi G. Rao for their help and support. RA is grateful to Director, INMAS, Delhi for support. Funding and support received from the Defence Research and Development Organization (DRDO), Government of India is acknowledged.
Disclosure Statement
The authors declare that they do not have any conflict of interest.