
Abstract
Background:
Tongxinluo (TXL), consisting of 12 Chinese Materia Medica items catalogued in the Chinese Pharmacopoeia, is commercially available in China, South Korea, and Russia. Hundreds of randomized clinical trials (RCTs) on TXL in treating cardiovascular diseases were conducted and published in China. This study provides a comprehensive Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)–compliant systematic review with sensitivity and subgroup analyses to evaluate the evidence about whether TXL is more effective than isosorbide dinitrate (ISDN) in treating ischemic heart disease, particularly angina pectoris.
Methods:
RCTs published between 1996 and 2010 on TXL versus ISDN in treating angina pectoris for at least 4 weeks were retrieved from eight bibliographical databases (e.g., MEDLINE,® PubMed, Chinese National Knowledge Infrastructure, Cochrane Library, and WanFang Data). The quality of RCTs was assessed with the Jadad scale. Meta-analysis was performed to estimate the overall effects based on symptomatic and electrocardiographic (ECG) improvements. Subgroup analysis, sensitivity analysis, and meta-regression were conducted on the study characteristics of RCTs.
Results:
Twenty (20) RCTs with a total of 1936 participants were included after eligibility assessment. The Jadad score of all included studies was 2. The means of summary odds ratios (ORs) for comparing TXL and nitrates were 3.30 (95% confidence interval [CI] 2.37–4.58) by symptoms (n=20) and 2.38 (95% CI 1.846–3.09) by ECG (n=18). There was a significant correlation of ORs between symptoms and ECG (ρ=0.77 and p=0.00026). Subgroup analysis, sensitivity analysis, and meta-regression found no significant difference in overall effects among all study characteristics except the years of publication (p=0.0409).
Conclusions:
The meta-analysis of 20 eligible RCTs demonstrates moderate evidence that TXL is more effective than ISDN for treating angina pectoris. This result warrants further RCTs of multicenters/countries, larger sample sizes, and higher quality.
Introduction
ISDN is a sodilator 5 to improve blood flow for getting more oxygen-rich blood to reach the heart muscle. 6 ISDN can be taken orally with a daily dosage of 10–240 mg. 2 TXL comprises Radix ginseng, Hirudo, Scorpio, Steleophaga, Scolopendra, Periostracum cicadae, Radix paeoniaerubra, sandalwood, Lignum acronychiae, frankincense, Semen zizyphispinocsae, and Dryobalanops camphor according to the Chinese Pharmacopoeia 2005. 7 TXL was approved as a New Drug (Drug Approval Number Z19980015) by the Ministry of Health of China in August of 1996. 8 The annual sale of TXL in 2009 was about 1 billion RMB (equivalent to 150 million USD). 9 TXL was listed as one of the National Essential Drugs of China in 2009; thus, the cost of using TXL is partially covered by various Chinese national health systems. The recommended dosage of TXL is 1.56–3.12 g daily for 4 weeks. 7
Since the launch of TXL in 1996, hundreds of randomized clinical trials (RCTs) have been published in Chinese that are often inaccessible to international researchers. Their compliance with the current Consolidated Standards of Reporting Trials 2010 10 is unknown. Systematic reviews on the RCTs of TXL 6,11 –13 were found but were not fully compliant with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement 14 and did not meet the goals in reviewing RCTs that compare TXL with ISDN. The first systematic review 11 was published in 2003, but it included quasi-RCTs. The second systematic review 6 was published in 2007, including 19 RCTs (1996–2007), but they included the studies using multiple drugs in a control group and did not conduct a subgroup analysis. The third systematic review 12 was a Cochrane review that included 18 RCTs (1995–2005), but its included studies combined multiple drugs in treatments. The latest systematic review 13 included 20 RCTs (2003–2008), but its included studies also used multiple drugs without any subgroup or sensitivity analysis. As such, the available systematic reviews cannot directly answer the current research question: Is TXL more effective than ISDN in treating angina pectoris? These four systematic reviews only covered the RCT reports up to 2008. Therefore, a comprehensive systematic review and meta-analysis of RCTs was conducted on testing TXL against ISDN. This study aims to provide a comprehensive, PRISMA-compliant, internationally accessible, and timely systematic review, with sensitivity and subgroup analyses of RCTs on TXL versus ISDN in treating angina pectoris.
Methods
Information sources
Bibliographic databases including WanFang Data, China Academic Journals Full-text Database on the China National Knowledge Infrastructure (CNKI), China Master Theses Full-text Database (CMTD), MEDLINE,® PubMed, Cochrane Library, Science Direct, EMbase, and China Doctor Dissertations Full-text Database (CDMD) were searched for the RCTs published between 1996 and 2010. The last search for all databases was performed on October 18, 2010.
Search strategies
Keywords used in search strategies were in Chinese or English, depending upon the working language of databases, and included 1. 2. 1 in Title/Abstract
The following search strategy was used in searching WangFang Data and other Chinese databases: 1. 2.
3. 4. 5. 1 in Title 6. 2 in Title 7. 5 or 6 8. 3 in Abstract 9. 4 in Abstract 10. 8 and 9 11. 7 and 10
Inclusion and exclusion criteria
Specific inclusion criteria were as follows: 1. RCT study design was explicitly described; 2. TXL and ISDN were compared; 3. Participants were suffering from angina pectoris as diagnosed by the criteria consistent with the World Health Organization guideline
5
; 4. There was at least 50% reduction in frequency of feeling anginal chest pain (symptoms) or significant improvement in ST segment in ECG during an exercise test
2
; 5. Follow-up period was not less than 28 days; and 6. Outcomes included the data of symptom improvements.
Exclusion criteria were as follows: (1) studies were duplicates; (2) other drugs were used with TXL and ISDN; and (3) diagnostic or therapeutic criteria were not reported.
Study selection
Two (2) reviewers (YJ and FB) independently screened all studies according to the eligibility criteria. Disagreements between reviewers were resolved by consensus. Redundant studies were excluded after discovery by juxtaposing author names, sample sizes, and outcomes. Figure 1 shows the screening process of relevant studies retrieved from databases.
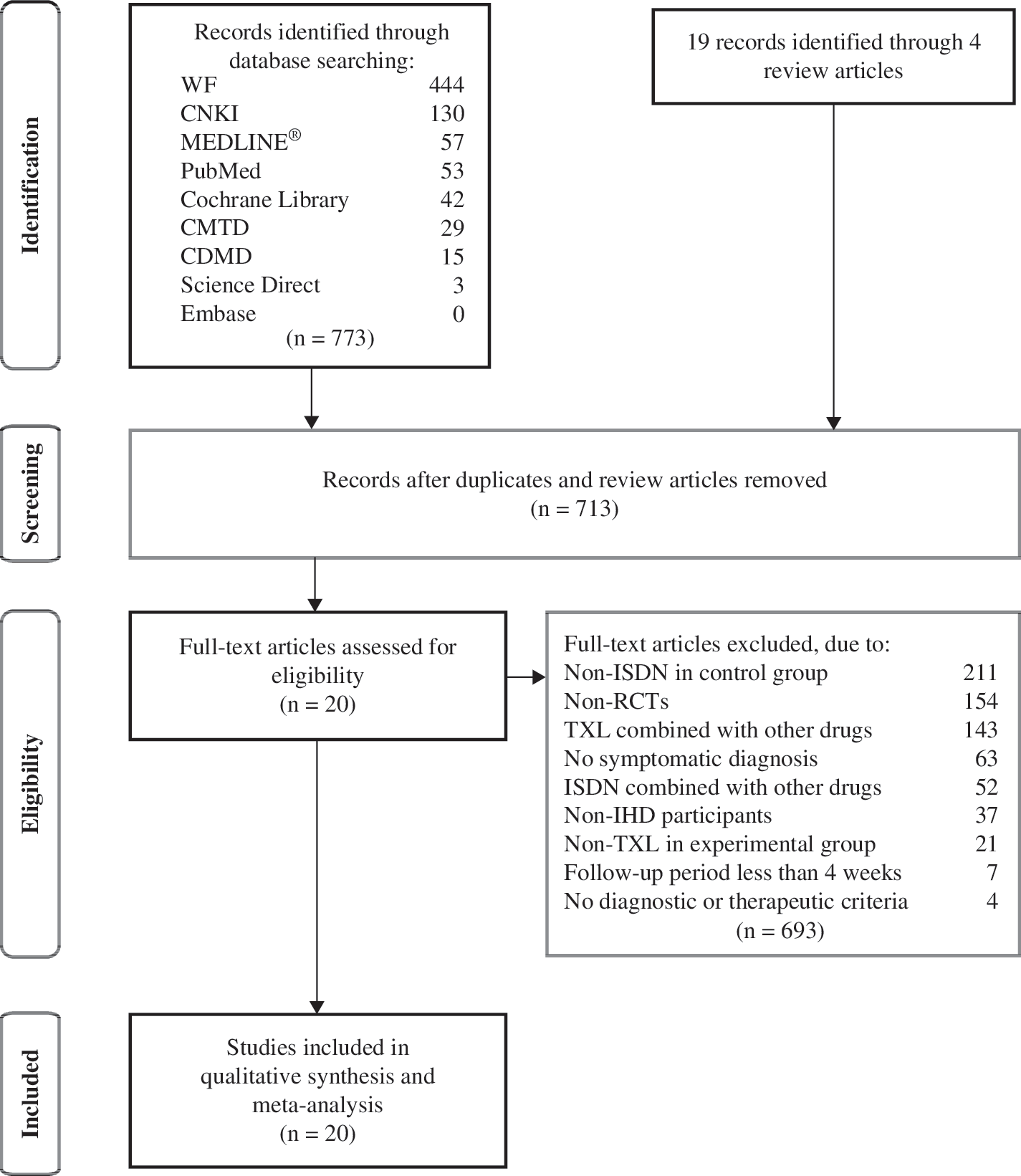
Process of searching and screening studies. WF, WangFang data; CNKI, China National Knowledge Infrastructure; CMTD, China Master Theses Full-text Database; CDMD, China Doctor Dissertations Full-text Database; ISDN, isosorbide dinitrate; RCTs, randomized controlled trials; TXL, tongxinluo; IHD, ischemic heart disease.
Data collection
Two (2) reviewers (FB and YJ) extracted information from the included studies and put them into an electronic spreadsheet using Microsoft Excel software. The other reviewers (SL and FH) checked the extracted data independently. Disagreements were resolved after discussion among reviewers. Extracted data were then transferred to software for statistical analysis.
Data items
Extracted data items comprised (1) publication time and number of authors; (2) participants of the included studies; (3) intervention (dosages and durations); (4) information about randomization, blinding, and dropouts; (5) basic characteristics of participants; (6) types and frequency of adverse events (AEs); and (7) outcome measures including improvements in symptoms and ECG.
Quality assessment of included studies
Two (2) reviewers (YJ and FH) independently assessed the quality of the included studies according to the Jadad Scale 15 and the Cochrane risk of bias tool. 16
Statistical analysis and meta-analysis
Odds ratios (ORs) and their 95% confidence intervals (CI) were used to measure effect sizes. Overall analysis and subgroup analysis employed the random-effects model because heterogeneity was expected. Heterogeneity
17
among studies was assessed by I2 and χ2. Meta-analysis and Forest plot generation were conducted using Review Manager.
5
The number-needed-to-treat (NNT) was computed for significant results.
18
Spearman correlation was performed between ORs of symptoms and ECG. Meta-regression was conducted using Stata software version 11 (StataCorp LP, USA). Statistical software R (
Sensitivity and subgroup analysis
Sensitivity analysis was performed to assess the efficacy of TXL based on OR of symptoms and ECG. Subgroup analysis was conducted to evaluate the overall effects in subgroups based on characteristics of the studies, including follow-up period, sample size, study period, year of publication, number of authors, and improvements in symptoms and ECG.
Meta-regression and risk of bias across studies
Publication bias was analyzed by funnel plots, 19 Begg's test, and Egger's test to visualize and evaluate the efficacy results of meta-analysis. Meta-regression 20 was conducted by residual (restricted) maximum likelihood (REML) with Knapp-Hartung modification 21 to find dependence of the efficacy of TXL on sample sizes, follow-up periods, and years of publication.
Results
Study selection
Figure 1 depicts the process of study search and selection. The database search identified 444 articles from WangFang Data, 130 articles from CNKI, 57 articles from MEDLINE, 53 articles from PubMed, 42 articles from the Cochrane Library, 29 articles from CMTD, 15 articles from CDMD, and 3 articles from Science Direct. In addition, 19 more articles were identified from previous systematic reviews. A total of 792 articles were manually screened. Seventy-one (71) articles were excluded because of redundancy. Eight (8) review articles were excluded. According to the prespecified eligibility criteria described in the Methods section, 20 studies 22 –40 (and Wu XF AM, unpublished thesis) were finally included for quality assessment and meta-analysis.
Study characteristics
Table 1 lists the main characteristics of 20 included RCTs. The included RCTs studies were published in Chinese between 1998 and 2008 with a total of 1936 participants aged between 29 and 85. The mean sample size was 97. The follow-up periods ranged from 28 days to 60 days. The daily dosages of TXL were 3.12 g (in 14 studies), 2.34 g (in 4 studies), 1.56–3.12 g (in 1 study), and 1.56 g (in 1 study). The daily dosages of ISDN were 30 mg (in 17 studies) and 30–60 mg (in 1 study).
TXL, tongxinluo capsule; ISDN, isosorbide dinitrate; AE, adverse event; SYM, symptoms; ECG, electrocardiogram; Number 1 or 0 in “Trial date” means that study reported or did not report the trial date, respectively; Number 1 or 0 in “Comparable” means that the study reported the comparability between the groups (1) or the study did not report that (0).
The outcomes symptoms and ECG changes were assessed. All 20 included studies employed symptoms changes and 18 of these 20 studies also employed ECG changes as therapeutic indicators. Secondary outcomes such as hemorheology, blood pressure, and heart rate variability were available in only some studies.
Quality assessment of included studies
The Jadad scale was used to measure the study quality, and all included studies were scored 2. One (1) study (Wu XF, unpublished thesis) reported single blinding and others did not mention blinding. Another study 38 reported 2 dropouts in the control group. Participants in other studies completed all their treatment. All included studies reported the use of randomization, but none specified the randomization procedures. Cochrane risk of bias tool also gave a similar rating to all included studies: low bias in incomplete outcome data and selective outcome reporting; high bias in the blinding of participants, personnel, and outcome assessors; and unclear bias in sequence generation, allocation concealment, and other sources of bias.
Results of individual studies and their synthesis
Figure 2 shows the overall symptoms; OR was 3.30 (95% CI 2.37–4.58, Z=7.08, p<0.00001; NNT=6.85) with a heterogeneity (I2=23%, χ2=24.71, p=0.17) among the 20 studies with symptoms outcome. I2=23% and p=0.17 (p>0.10) indicates there is not heterogeneity in symptoms in RCTs included. Figure 3 shows that the overall OR of ECG was 2.38 (95% CI 1.84–3.09, Z=6.54, p<0.00001; NNT=5.47) with a heterogeneity (I2=36%, χ2=26.64, p=0.06) among the 18 studies with ECG outcome. The symptoms and ECG were moderately correlated (ρ=0.77) with a high statistical significance (p=0.00026).
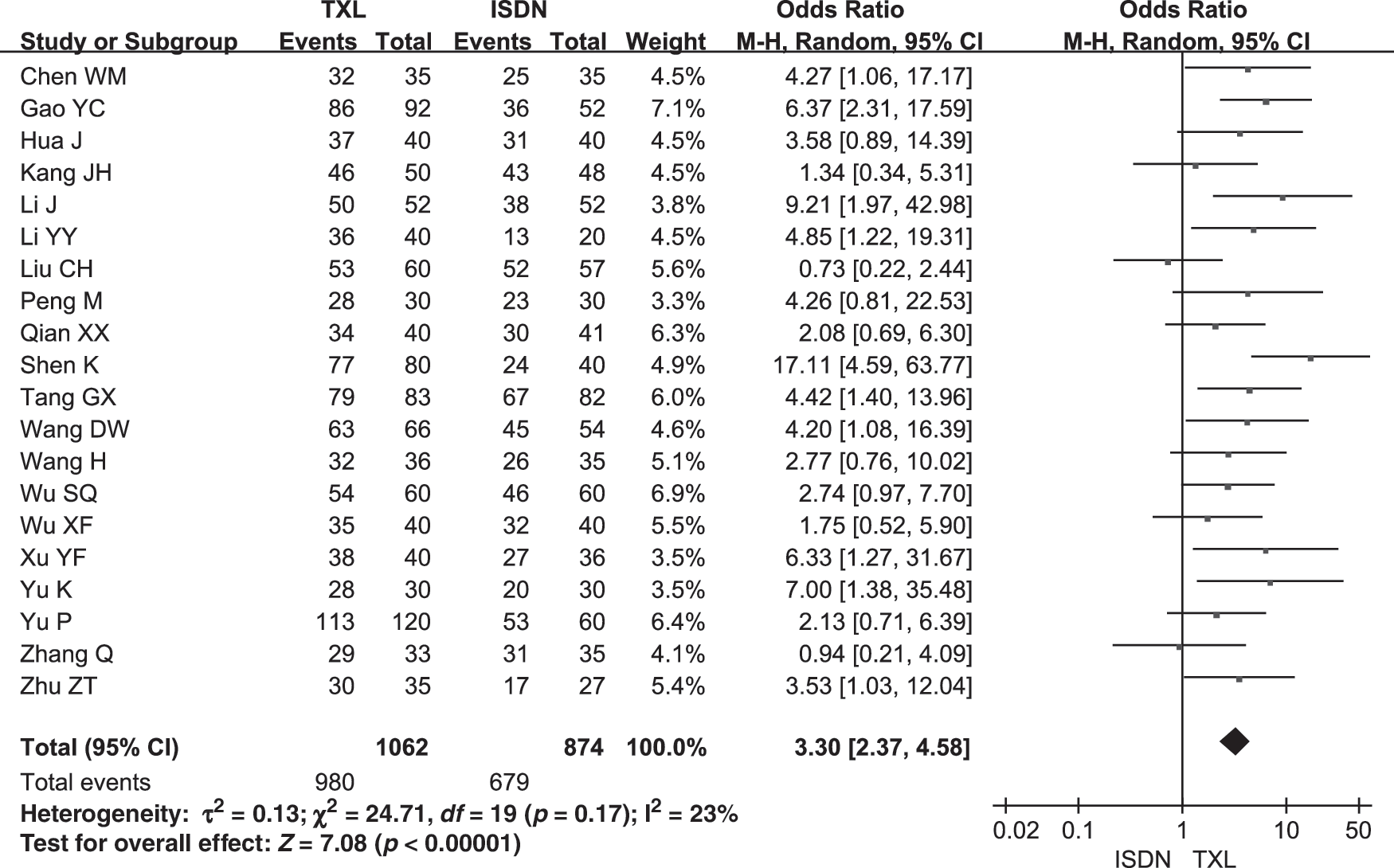
Forest plot of outcome measure symptoms. TXL, tongxinluo; ISDN, isosorbide dinitrate; M-H, Mantel-Haenszel; CI, confidence interval.
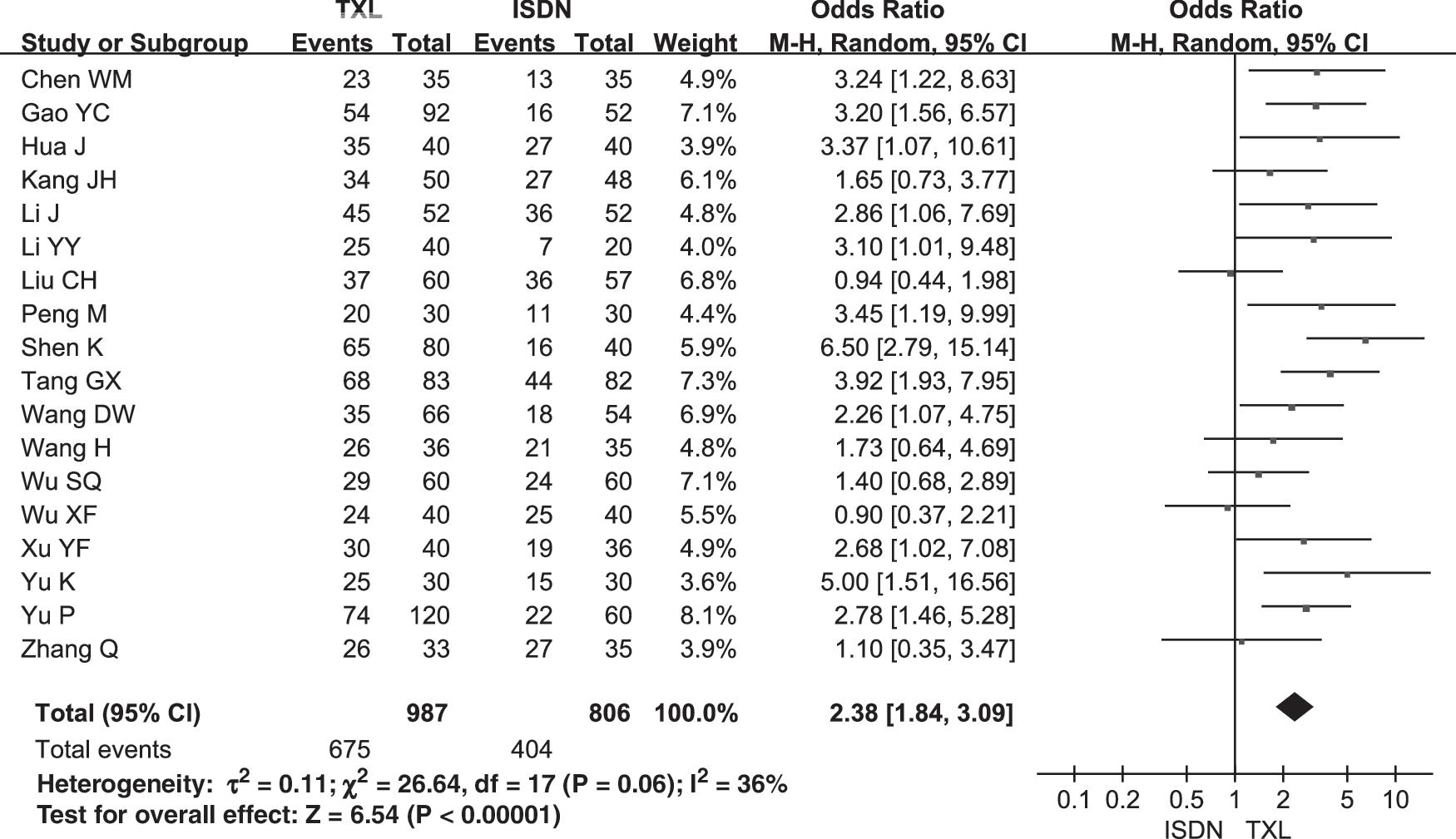
Forest plot of outcome measure electrocardiogram. TXL, tongxinluo; ISDN, isosorbide dinitrate, M-H, Mantel- Haenszel, CI, confidence interval.
The meta-analysis based on OR of the outcomes symptoms and ECG reported in the included 20 articles indicated that TXL is more effective than ISDN in treating angina pectoris. Meanwhile, Spearman correlation analysis showed that symptoms and ECG corroborated with each other to provide positive evidence.
Sensitivity and subgroup analysis
To evaluate the robustness of the results, a sensitivity analysis was performed after raising the standards for symptoms improvement to achieve at least 80% reduction in frequency of feeling anginal chest pain and for ECG improvement to achieve at least nearly normal state. Under this strict standard, the overall symptoms OR remained high as 2.35 (95% CI 1.85–3.00, Z=6.93, p<0.00001; NNT=4.78) with a heterogeneity (I2=31%, χ2=27.73, p=0.09) among the 20 studies. The overall OR of ECG was also as high as 2.36 (95% CI 1.83–3.03, Z=6.68, p<0.00001; NNT=6.57) with a heterogeneity (I2=4%, χ2=15.67, p=0.40) among the 16 studies with the higher ECG standards (i.e., two studies had only the lower ECG standards). The symptoms and ECG OR were moderately correlated (ρ=0.80) with a high statistical significance (p=0.00027).
Based on different follow-up periods, sample sizes, year of publication, number of authors, date of trials, AEs, and TXL daily dosages that would affect the overall effects, subgroup analyses were performed and their results are shown in Tables 2 and 3. Wilcoxon test was conducted based on OR between the subgroups. There were no significant difference in the OR of symptoms except for the factor of publication year (p=0.0409) and ECG between the subgroups. The mean sample size of the 20 included studies is 97, which is much less than 186 as required to achieve a desired power of 0.8. 41 The studies were divided evenly into two subgroups (one with less than mean sample size and the other with more than mean sample size) by their sample sizes for subgroup analysis.
The overall efficacy was meta-analyzed for different sample sizes, different published time, different follow-up periods, different improvement definitions, and so on. Mann-Whitney-Wilcoxon test was performed on ORs of symptoms. Z and p (effect) evaluated the statistics of overall effect; I2, χ2, and p (het) were computed to assess heterogeneity. Sample size of 97 was computed to achieve a power of 0.8.
OR, odds ratio; CI, confidence interval; W, Wilcoxon value; p, p-value for Wilcoxon test; AE, adverse event; TXL, tongxinluo capsule.
The overall efficacy was meta-analyzed for different sample sizes, different published time, different follow-up periods, different improvement definitions, and so on. Mann-Whitney-Wilcoxon test was performed on ORs of symptoms. Z and p (effect) evaluated the statistics of overall effect; I2, χ2, and p (het) were computed to assess heterogeneity. Sample size of 97 was computed to achieve a power of 0.8.
OR, odds ratio; ECG, electrocardiographic; CI, confidence interval; AE, adverse event; TXL; tongxinluo capsule; W, Wilcoxon value; p, p-value for Wilcoxon test.
The corroboration of the results from sensitivity and subgroup analysis suggests that the efficacies among all included studies were robust.
Meta-regression
Table 4 shows the results of meta-regression based on logOR of ECG and study characteristics. Meta-regression was conducted using REML with Knapp-Hartung modification. Factors of publication year, number of authors, and TXL daily dosage made no significant difference (p>0.05).
Meta-regression was conducted by residual (restricted) maximum likelihood (REML) with Knapp-Hartung modification. Ô2, REML estimate of between-study variance; I2, % residual variation due to heterogeneity; adjusted R-squared (R2), proportion of between-study variance explained.
RCTs, randomized controlled trials; OR, odds ratio; ECG, electrocardiographic; TXL, tongxinluo capsule; AE, adverse event.
Risk of bias across studies
Publication biases of major outcomes symptoms and ECG were not significant as assessed by Funnel plots, which found no obvious asymmetry for symptoms (Fig. 4) and ECG (Fig. 5) in the plots. The plots were consistent with the Begg's test (for symptoms: Z=1.17, p=0.243; for ECG: Z=0.34, p=0.733) and the Egger's test (for symptoms: t=0.87, p=0.396; for ECG: t=0.40, p=0.697).
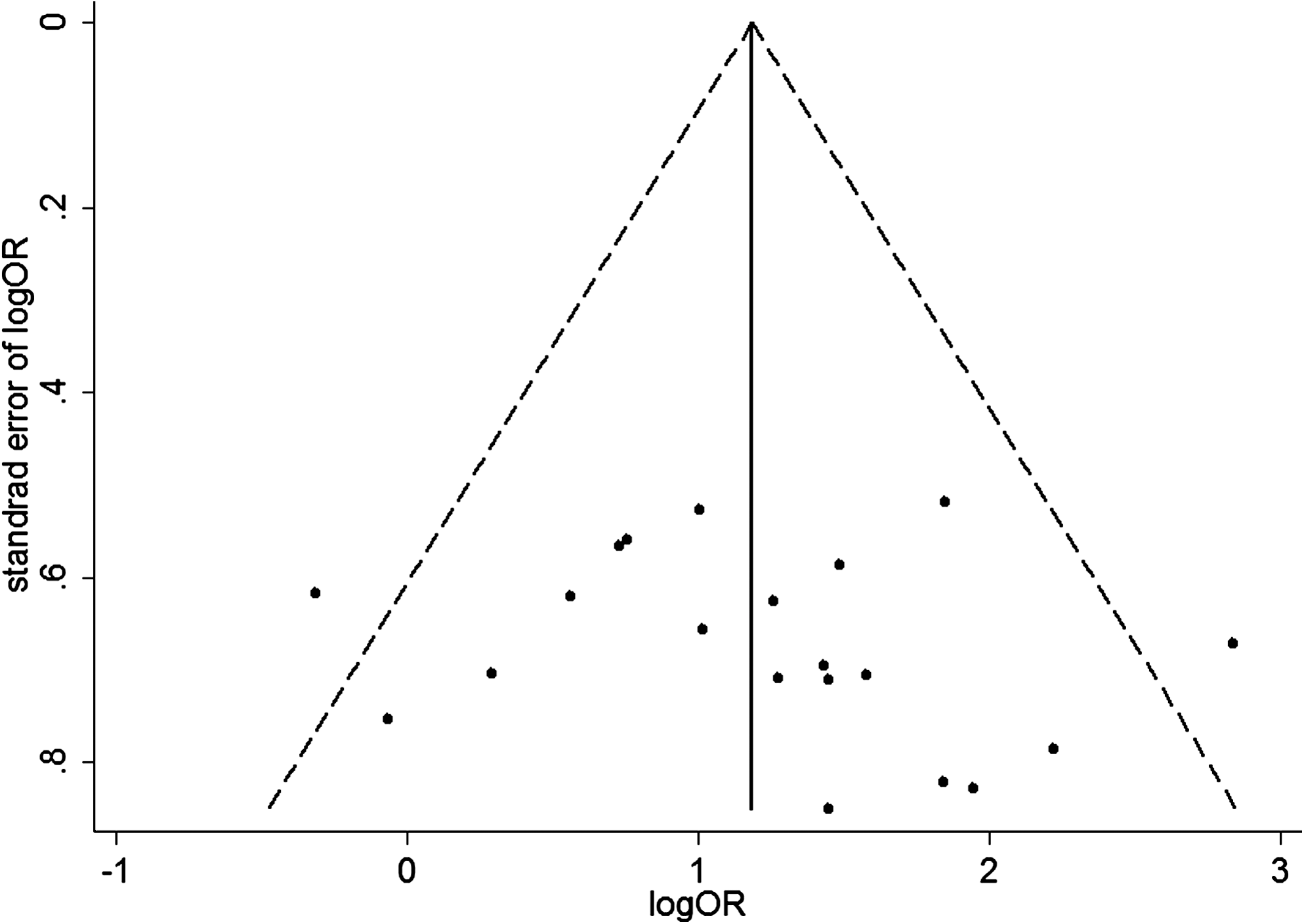
Funnel plot of the included studies with symptoms data. OR, odds ratio.
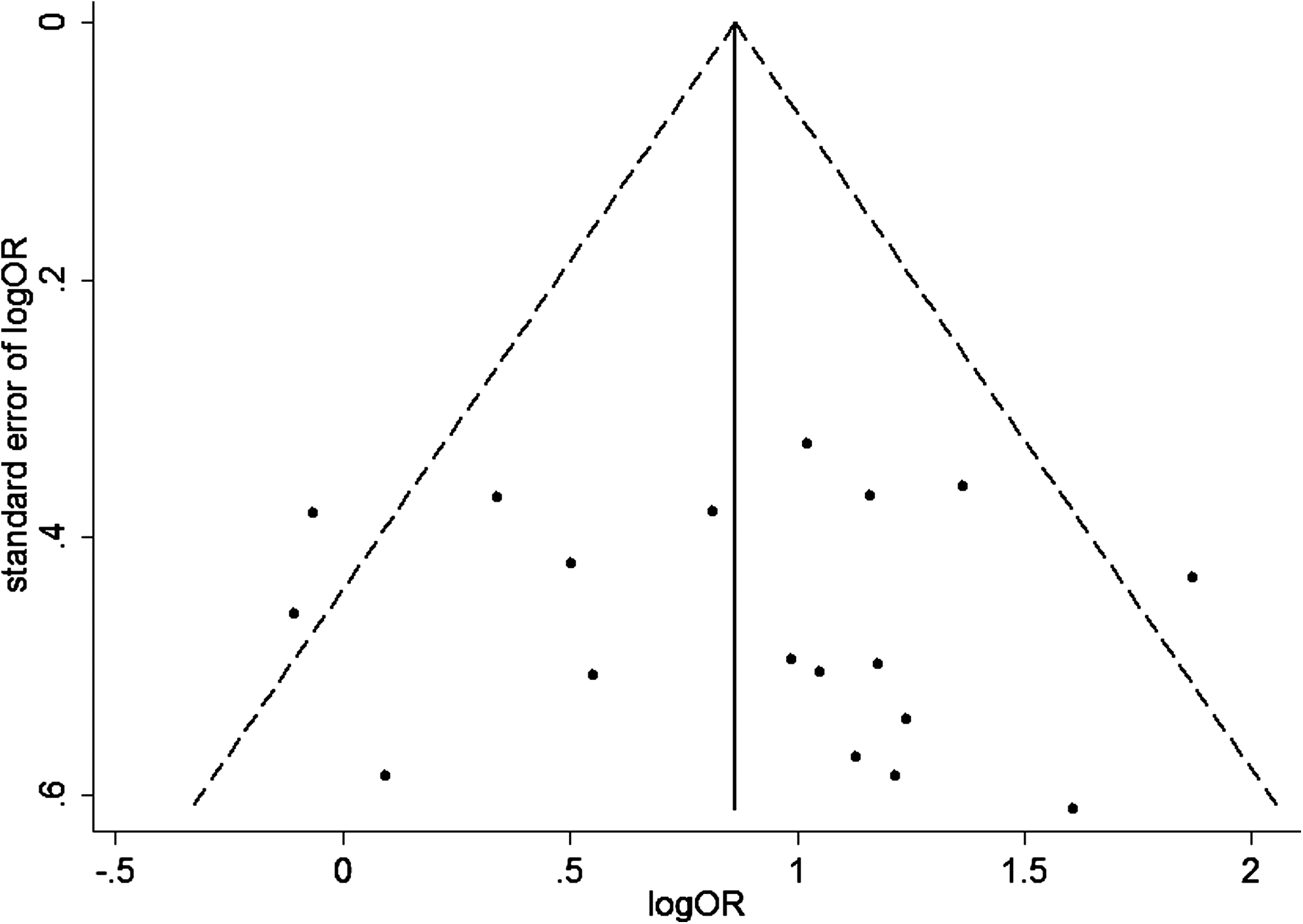
Funnel plot of the included studies with electrocardiogram data. OR, odds ratio.
Adverse events
Eight (8) 23,26,27,30,32,33,39,40 of 20 included studies did not mention any adverse effects. No adverse effects in the experiment group were reported in three studies 31,38 (and Wu XF, unpublished thesis). Four studies 24,31,36 (and Wu XF, unpublished thesis) reported no adverse effects in the control group. Eight (8) studies 22,24,28,29,34,35 –37 reported 14 participants who had stomach discomfort or epigastric discomfort in the experiment group. Eight (8) studies 22,25,28,29,34,35,37,38 reported headache or distension in the head as the AE. Three (3) studies 22,28,29 reported red face. One (1) study 28 reported dizziness. In terms of types and frequency, adverse effects of TXL were less than those of ISDN.
Discussion
This article provides a PRISMA-compliant, internationally accessible, and timely systematic review on the efficacy of TXL over ISDN. Overall OR of symptoms and ECG were 3.30 and 2.38, respectively, with a significant difference between TXL and ISDN (p<0.00001). Sensitivity analysis, subgroup analysis, and meta-regression on various parameters showed this positive evidence to be robust. Results of this systematic review provided a piece of evidence to suggest that TXL is more effective than ISDN in treating angina pectoris.
This systematic review is different from previous reviews in the following aspects: (1) comprehensive search for RCTs published between 1996 and 2010 were performed (previous systematic reviews did not provide a comprehensive literature search, which is one of the most important steps in a systematic review 34 ); (2) only TXL and ISDN were selected as single-drug interventions (previous systematic reviews combined multiple drugs); (3) follow-up periods were at least 28 days (compliant with the recommended treatment course for TXL); (4) subgroup analysis, sensitivity analysis, and meta-regression based on the basic characteristics of included studies were performed (previous systematic reviews provided less analysis) ; and (5) publication biases were assessed not only by Funnel plot but also by the Begg's test and Egger's test.
A major limitation of this systematic review is the quality of included studies. All 20 studies were scored 2 according to the Jadad scale (range 0–5). Neither allocation concealment nor blinding was mentioned in the included studies. This finding of RCT quality for TXL is consistent with previous reports, 42 –45 which found that the RCTs on Traditional Chinese Medicine were of low-to-medium quality. Sensitivity and subgroup analysis based on the quality of studies could not be performed because all the included studies received the same score in quality.
There are some other limitations of included RCTs in this systematic review. Most studies reported that the daily dosage of ISDN was 30 mg at lower normal dosages in everyday clinical practice, which may not represent the best anti-anginal therapy. The follow-up periods ranged from 28 days to 60 days. Ninety-seven (97) of the mean sample size was much less than 186 as calculated according to the theory. 41 No study was completed in multicenter/multicountry settings. Eight of the studies did not mention AEs. The studies mentioning AEs did not report AEs in a formal manner. Thus, the safety of TXL was not evaluated.
To further study the efficacy of TXL, RCTs with larger sample size, multicenters/multicountries, uniform diagnostic and therapeutic criteria, and longer follow-up periods are still required to compare TXL with the best therapy (not only ISDN) to overcome the current study limitations.
Conclusions
The meta-analysis of 20 eligible RCTs demonstrates moderate evidence that TXL is more effective than ISDN for treating angina pectoris. This result warrants further RCTs of multicenters/multicountries, larger sample sizes, and higher quality.
Footnotes
Acknowledgments
The work of S.L. was partially supported by the e-Science Research Theme grant received from the National e-Science Institute, United Kingdom. The work of S.L. and Y.J. was also partially supported by a research grant (“open systematic reviewing of clinical trials”; MYRG190(Y1-L3)-ICMS-LSW) received from the University of Macao.
Disclosure Statement
No competing financial interests exist.