
Abstract
Background/objective:
A functional medicine approach to reduce breast cancer risk is preferable to early detection and treatment in maintaining breast health. Estrogens are implicated in breast cancer initiation through conversion to metabolites that react with DNA to form specific adducts associated with the development of breast cancer. The purpose of this study was to determine the ability of a defined clinical intervention, the AVERTi-Healthy Breast Program (AHBP), to reduce breast cancer risk conditions likely to develop into breast disease.
Methods:
To obtain evidence that risk conditions in breast tissue can be reduced with a defined, multifaceted approach, this small clinical trial of 21 women measured indicators of breast health. A detailed clinical evaluation was conducted with all participants, including identification of physical symptoms, such as areas of tenderness upon palpation. Two laboratory assessments were conducted to determine the efficacy of the AHBP. First, 31 estrogen metabolites, estrogen conjugates, and depurinating estrogen-DNA adducts in urine samples taken before intervention were analyzed. The ratio of DNA adducts to metabolites and conjugates was calculated for each sample. Second, oxidative stress was analyzed by measuring the redox potential of glutathione and cysteine in blood plasma. All assessments were conducted before and after participation.
Results:
The estrogen adduct ratio and redox potential were improved after 90 days on the AHBP. A significant mean reduction of 3.31 (p=0.03) was observed in the adduct ratio, along with a significant improvement in the redox potential of 3.80 (p=0.05). The significant change in the adduct ratio occurred in women whose oxidative stress profile also improved.
Conclusion:
These significant within-individual decreases suggest that the AHBP can reduce the risk for breast cancer in a relatively short time.
Introduction
A
Breast cancer is considered an inflammatory disease, potentially arising from cellular oxidative stress and immunologic responses. 1,2 To appreciate the foundation of this approach, it is essential to review the initiation of breast cancer by estrogen genotoxicity. 3 Epidemiologic evidence shows a dose–response relationship between exposure to estrogens and risk for breast cancer. 4 Evidence from studies of estrogen metabolism, formation of DNA adducts, mutagenicity, cell transformation, and carcinogenicity led to and supports the hypothesis that catechol estrogen quinone metabolites react with DNA to form estrogen-DNA adducts in critical genes, initiating the process leading to breast cancer (Fig. 1). 3 This understanding led the authors to the approach of modifying biological systems that contribute to breast inflammation and formation of estrogen-DNA adducts to reduce the risk for breast cancer.
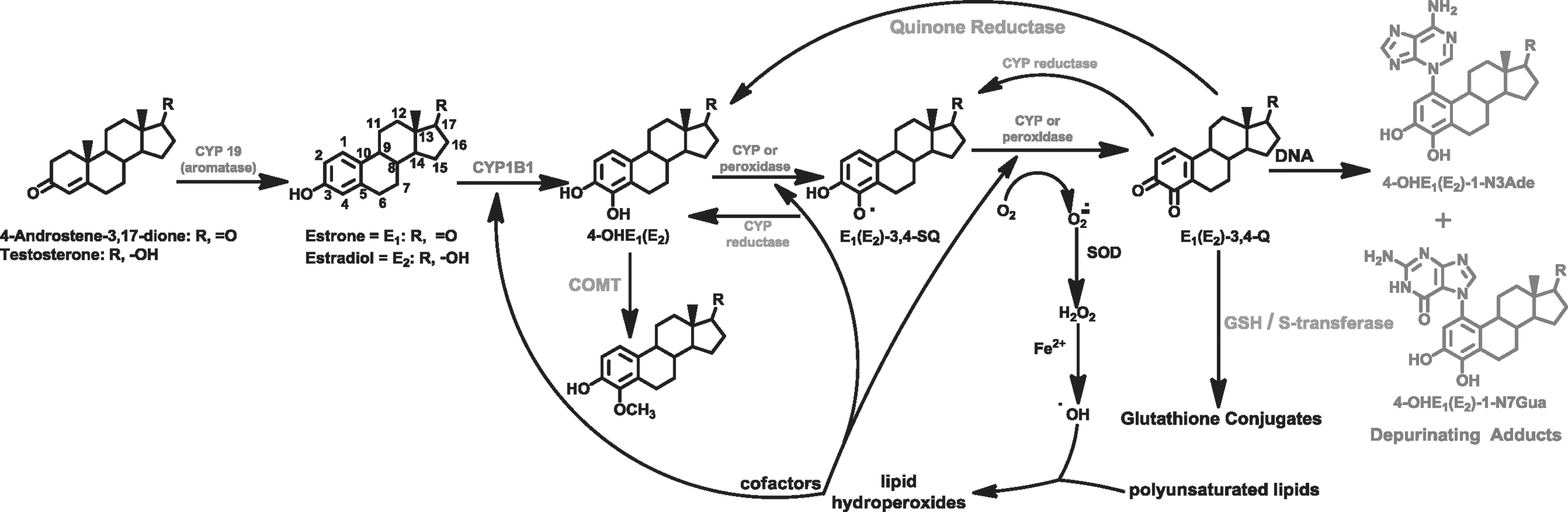
Metabolism of estrogens to catechol estrogen-3,4-quinones, their reaction with DNA to form the depurinating 4-OHE1(E2)-1-N3Ade and 4-OHE1(E2)-1-N7Gua adducts, and the role of oxidative stress in delivering cofactors that increase the level of adducts. COMT, catechol-O-methyltransferase; GSH, glutathione.
Functional medicine 5 –7 is a science-based, personalized health care approach that treats underlying causes of illness through individually tailored therapies to restore health by improving function of interactive biologic systems. Patient and practitioner partner in designing a customized program that integrates clinical science with standards of practice and changes in the individual's environment, diet, and lifestyle to treat illness and promote wellness. Through use of the functional medicine approach, the authors obtained evidence that risk conditions in breast health can be reduced.
This small clinical trial of 21 women was conducted to evaluate the ability of a defined functional medicine intervention, the AVERTi Healthy Breast Program (AHBP) (Fig. 2), to induce biotransformation and reduce oxidative stress, thereby reducing breast cancer risk in manner that can be verified through laboratory and clinical measurements. These measurements were as follows: (1) analysis of 31 estrogen metabolites, estrogen conjugates, and depurinating estrogen-DNA adducts in a urine sample and (2) analysis of oxidative stress by measuring the redox potential of the thiol/disulfide of glutathione (GSH) and cysteine from plasma 8 to determine the individual's capacity for management of oxidative stress. Both measurements were done before the intervention and 90 days after the intervention. The hypothesis of this study is that a functional medicine approach to breast health, using a well-defined intervention (AHBP), can be used to (1) reduce the estrogen-DNA adduct ratio and (2) improve oxidative stress capacity. Consequently, the association between the DNA adduct ratio and oxidative stress measures in women from before to after the intervention was assessed.
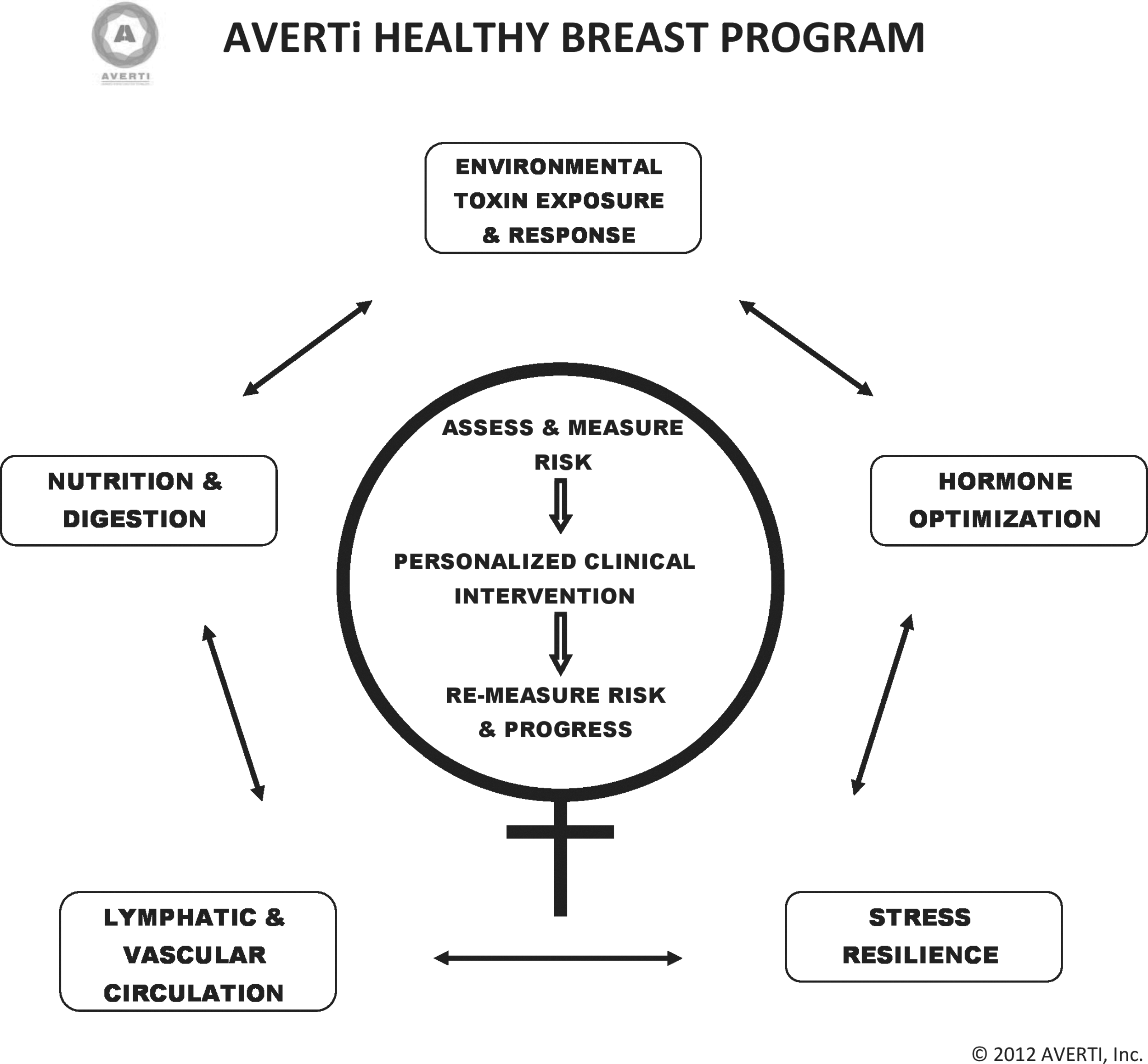
AVERTi Healthy Breast Program (AHBP) reflects five biological aspects of functional medicine in assessment and risk measurement followed by the clinical development of a personalized intervention and the consequent reassessment of progress and re-measurement of risk.
Materials and Methods
Study sample
Participants were recruited from November 2011 until February 2012. Inclusion criteria included age 30–70 years; no current diagnosis of breast cancer as confirmed by mammography, magnetic resonance imaging, or ultrasonography (for those under age 35) performed within the last year; no current use of synthetic hormone replacement therapy; and no experience with the Longevity Healthcare medical practice. Participants were solicited through a local newspaper and a health newsletter. Interested women attended an open information meeting and were later interviewed by S. Muran to determine whether they met the selection criteria and could participate in the study for 90 days. Of the 36 women screened for eligibility, 26 met selection criteria and gave informed consent. The response rate among those who met inclusion criteria was 72%.
After recruitment, participants underwent a comprehensive general health history, a detailed breast health history, baseline laboratory assessment, physical examination, and scheduled clinical appointments to individualize five key intervention activities. These activities targeted lymphatic and vascular circulation, optimized nutrition and digestion, managed environmental toxin exposure and response, provided hormonal balance, and offered stress resilience techniques. Participants were requested to keep a breast health journal, follow clinical recommendations, and attend monthly group education meetings. Twenty-one participants completed the AHBP program.
Post-intervention activities included a self-administered compliance survey and a repeat of baseline sample collections. In this survey, participants scored the frequency with which they carried out five key interventions in the AHBP. Group and confidential individual laboratory results were provided to the participants at the conclusion of the study.
Initial evaluation of each participants included Gail model score 9 information, a comprehensive health history, a detailed breast health history, and a physical examination; laboratory evaluation with complete metabolic profile, complete blood count, and urine analysis; evaluation of nutrition habits, food intolerances, and digestive health; and environmental exposure survey. The baseline breast health profile included the estrogen-DNA adduct ratio and the oxidative stress laboratory test. On the basis of individual assessment, each participant was guided through the AHBP by use of a functional medicine 10,11 clinical approach focused on nutrition and digestive health, hormone balance, circulatory health, environmental exposures, and stress resilience.
Clinical application of the functional medicine matrix 10 evaluated the participants for core clinical imbalances that underlie the expression of disease, including hormonal imbalances; oxidative-reduction imbalance; detoxification and biotransformation imbalances; immune and inflammatory imbalances; and digestive, absorptive, and microbiome imbalances. 11 Individualized recommendations were made to promote breast health through measures that affect specific cell metabolism in the breast. These recommendations increased vascular and lymphatic flow; improved the efficacy of digestion; led to avoidance of food sensitivities and correction of nutrient deficiencies; optimized hormone function; managed environmental toxin exposure through education and assessment of capacity for response; and provided stress resilience techniques. Subsequently, the combined effects decreased the body's inflammatory profile and modified estrogen metabolic pathways.
Clinical evaluation and recommendations were translated into breast health–promoting educational materials and activities easily comprehended and implemented by the participants. This process constituted the AHBP. Participants attended three monthly group education meetings and engaged in follow-up clinical consultations to encourage compliance with recommendations.
Analysis of estrogen compounds
Catechol estrogen metabolites are strongly implicated in the initiation of breast cancer. 3 In particular, the catechol estrogen-3,4-quinones react with DNA to form the adducts 4-hydroxyestrone(estradiol)-1-N3Ade [4-OHE1(E2)-1-N3Ade] and 4-OHE1(E2)-1-N7Gua, which are released by depurination, leaving apurinic sites in the DNA (Fig. 1). These depurinating adducts have been repeatedly associated with the presence of breast cancer. 3
Urine collection for the estrogen metabolites
A fasting urine (approximately 50 mL) specimen was collected in the morning. Urine samples were separated into aliquots, frozen, and transferred to the Cavalieri–Rogan laboratory, University of Nebraska Medical Center on dry ice and stored at −80°C. Thus, each analytical sample was thawed only once before analysis. All of the study samples were analyzed in triplicate in a blinded fashion. All samples were prepared and subjected to ultra-performance liquid chromatography/tandem mass spectrometry analysis. 12
The precision of these analyses is provided by the limit of detection and coefficient of variation for the ultra-performance liquid chromatography/tandem mass spectrometry method. 12 Replicate samples were analyzed in various batches of pre-intervention and post-intervention samples. Therefore, the standard deviations, represented by error bars in Figure 2, are a measure of the variability of the assay.
The ratio of depurinating N3Ade and N7Gua adducts to the sum of their respective metabolites and conjugates in each urine sample was calculated according to the ratio formula 12 and provides a ratio that reflects the degree of imbalance in estrogen metabolism that may lead to cancer initiation.
Plasma collection for the oxidative profile
The amino acid cysteine and the peptide GSH are important in the detoxification of xenobiotics. Their redox state represents the ability of the cell to reduce quinone-containing metabolites. A high ratio of the 4-OHE1(E2)-1-N3Ade and 4-OHE1(E2)-1-N7Gua adducts to estrogen metabolites and conjugates could indicate a state of increased oxidative stress, which should be associated with an increased DNA adduct ratio.
The reduction potentials for the redox couples GSH/glutathione disulfide (GSSG) and cysteine/cystine (Cys/CySS) were calculated by determining the plasma levels of GSH, GSSG, Cys, and CySS. Fasting serum samples were collected in the morning. The serum sample was then treated as described by Jones and Liang 13 with the use of N and S tubes. The S tubes were stored at −40°F. The collected samples were shipped on dry ice to Emory University for evaluation of the thiol/disulfide couples. 13
Variability in determining oxidative stress using the reduction potentials of the redox couples GSH/GSSG and Cys/CySS by analyzing the plasma levels of GSH, GSSG, Cys, and CySS is influenced by the patient's age, the collection process, and the analysis process. 8,13 In this study, the participant's age did not contribute to the variability because each participant provided samples twice in 3 months. Variability in the collection process is the result of three major influences: time of day of the blood draw, food that the patient ate before the blood draw, and method by which the blood was drawn and prepared. All participants had their blood drawn while in the fasting state and in the morning by the same experienced clinician throughout the study.
The variability of the analytical process determining the reduction potential of the redox couples GSH/GSSG and Cys/CySS is reflected in the same participant's results of GSH/GSSG, which did not significantly change over 3 months, compared with the more readily oxidized Cys/CySS, which did significantly change. The three individual analyses for each sample varied slightly.
Statistical analysis
Descriptive statistics
Information was collected from interviews and patient charts. Demographic and risk factor data collected on study participants included age, menopausal status, history of hormone replacement therapy use, parity, history of cigarette smoking, and level of physical activity. Compliance scores were created by summing up the frequency with which each woman reported having adhered to the treatment plan. Higher scores indicated greater compliance. Means and standard deviations of the adduct ratio and oxidative stress markers were calculated for the group at baseline and after the intervention.
Bivariate analyses
The DNA adduct ratio was log transformed to improve normality at baseline and post-intervention. The GSH and cysteine oxidative stress markers were normally distributed. The Pearson correlation coefficient was used to determine the strength of linear relationships between the adduct ratio and oxidative stress markers at baseline and post-intervention. Paired t tests and analysis of variance were used to assess changes in the adduct ratio and oxidative stress markers within a study participant across time points. Repeated-measures analysis of covariance was used to assess whether age or menopause explained any of the variance in the DNA adduct ratio across time points. Mean adduct ratios and redox potentials were calculated before and after AHBP.
To explore relationships between the adduct ratio and oxidative stress markers, the study analysis the samples were stratified by those whose oxidative stress profiles improved and tested whether the adduct ratio significantly changed in the two groups. Mean differences in the oxidative stress markers were calculated using SAS, version 9.4 (SAS Institute Inc, Cary, NC) in each of the two oxidative stress groups, and significant changes in the adduct ratio were calculated using the paired t test for within-participant differences.
Results
Study sample
Twenty-six women met the eligibility requirements and were recruited into the study. Of these, 21 provided complete information and serum and urine samples for the biomarker analyses. Attrition resulted from life events, such as travel, surgery, and divorce. The mean age (standard deviation) was 53.7±8.18 years (range, 34–66 years), and 81% of participants were postmenopausal (Table 1). They were generally healthy, with 57% having never smoked cigarettes and 81% reporting that they exercised regularly.
Biomarker analysis
Adduct ratio
Neither menopausal status nor age was associated with the DNA adduct ratio at pre- or post-intervention. Before the intervention, the mean adduct ratio was 19.3±9.63 (range, 5.15–46.9); after the intervention it was 16.0±7.91 (range, 5.15–32.2) (Fig. 3). At the individual level, a significant mean reduction of 3.31 was observed in the DNA adduct ratio after the intervention (t=−2.10; p=0.03).
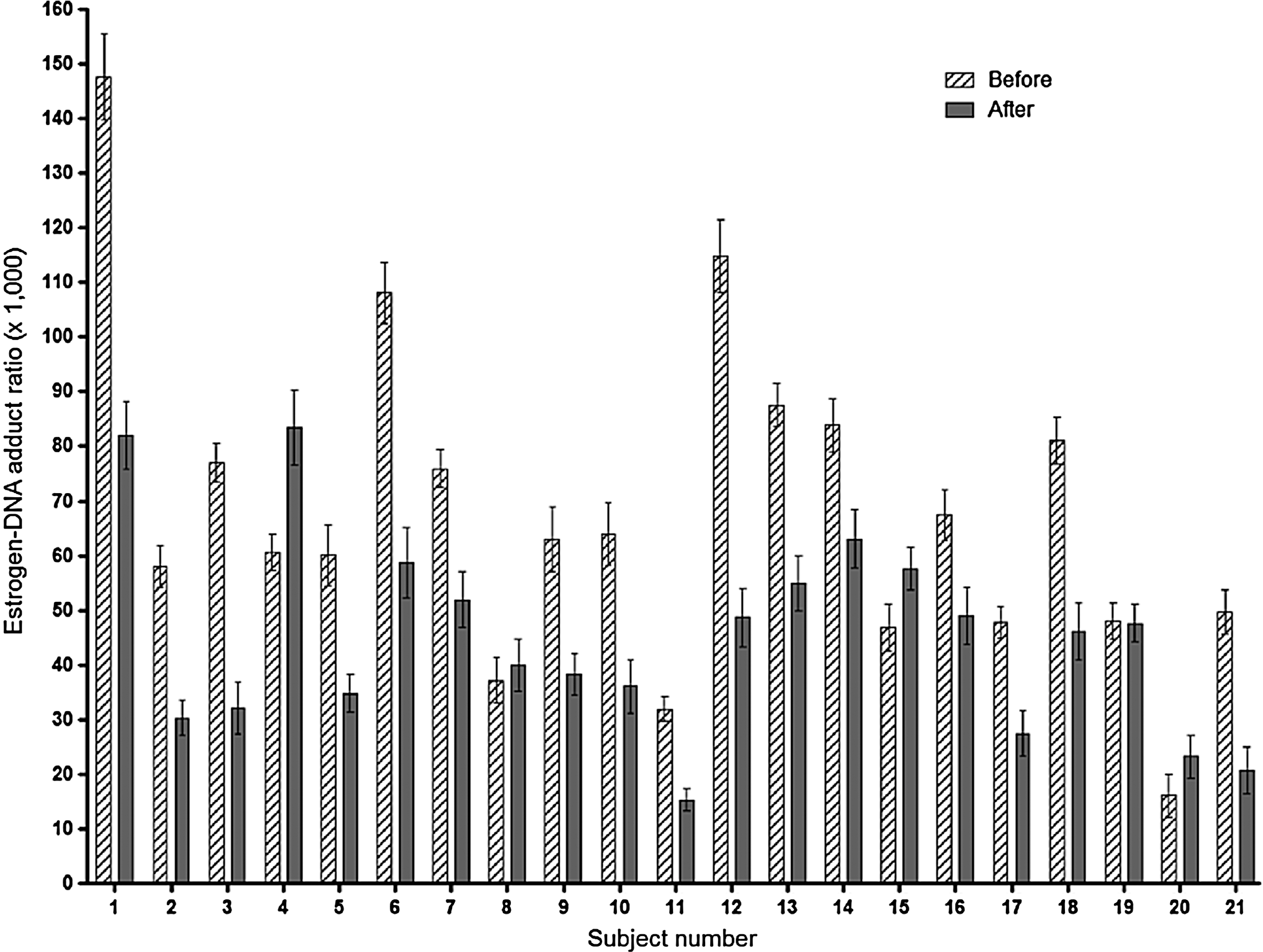
Assessment of DNA adducts ratios (n=21) before women began the AHBP and after having been on the AHBP for 3 months. Error bars represent standard deviations.
Oxidative stress markers
The redox potential for cysteine improved after the intervention. At baseline the mean group value was −70.6±7.46 and after the intervention it was −74.4±6.50); the mean difference within study participants was 3.81 and was statistically significant (t=2.08; p=0.05). GSH remained unchanged from baseline to post-intervention (baseline mean, −133.0±10.7; post-intervention, −133.2±8.91). The redox potential of GSH did not significantly differ within participants.
Adduct levels and oxidative stress markers
The baseline adduct ratio was positively and significantly correlated with the post-intervention redox potential of cysteine (r=0.49; p=0.026). Because we were interested in the combined effects of DNA adduct and oxidative stress levels, we assessed the mean adduct level in participants whose cysteine redox potential improved (values became more negative after the protocol) and in those whose redox potential stayed the same or worsened. Those without an improvement in the redox potential for cysteine showed a minimal and insignificant change in the adduct ratio, but in women whose cysteine profile improved, the adduct ratio significantly decreased (Table 2). Women whose redox potential for cysteine improved reported greater compliance with the program elements than did women who showed no improvement (mean, 29.14±4.59 versus 28.67±3.01). Similarly, women who reduced their adduct ratios also complied more fully with the program than those who did not (mean, 29.8±3.24 versus 27.6±5.35). Statistically, this represents a potential parallel trend of therapeutic engagement and measurable outcome.
As calculated using the Nernst equation, negative values indicate better capacity to manage oxidative stress. Therefore, improvement in oxidative stress capacity means a more negative value and a positive value reflects a decreased ability to manage oxidative stress. Values expressed with a plus/minus sign are expressed as the mean±standard deviation.
p=0.05.
Cys/CySS, cysteine/cystine.
Discussion
This study showed that the functional medicine–based AHBP (Fig. 2) could improve two early breast cancer indicators: estrogen-DNA adduct ratio and redox potential. These results suggest that lower adduct ratios both before and after the intervention were positively correlated with a good ability to handle oxidative stress and inflammation, as indicated by good ratios of reduced cysteine compared to oxidized cysteine (Table 2). Better ability to handle oxidative stress can affect estrogen metabolism by decreasing the likelihood of oxidation to catechol estrogen quinones, thus decreasing the formation of estrogen-DNA adducts. Significant within-individual decreases were seen in the DNA adduct ratio and in oxidized cysteine in women who complied with at least one component of the program with at least 90% frequency. Of the six components of the treatment plan, women reported compliance with two of them at least 90% of the time and three others at least 75% of the time. Only a single aspect of the program showed around a 50% compliance rate. At the conclusion of this pilot study, 95% of the participants reported that they would be likely to continue with the AHBP, indicating that it is an intervention that is sustainable.
The within-individual participation in the AHBP appears to correlate to the decrease of oxidation stress and inflammation, thus decreasing the formation of estrogen DNA adducts (Table 2, Fig. 3), which are associated with the development of breast cancer (Fig. 1).
Both estrogen-DNA adduct ratio and oxidized cysteine have been established as breast cancer risk factors. Of the 21 healthy women who completed this study, 15 showed significant improvement in their oxidative stress profiles. In the improved group, there was a marginally significant reduction in the DNA adduct ratio after the 90-day program, although the adduct ratios were similar in these two groups before the intervention. These statistically significant within-individual decreases demonstrate that the adduct ratio can be altered in a relatively short period. Similarly, the redox potential of cysteine increased significantly, showing that it is amenable to improvement in only 90 days. The fact that these events occurred together suggests that a common underlying mechanism may exist, but additional studies are needed to elucidate the causal pathways. This study was exploratory and the first to attempt to modify early breast cancer risk factors and connect oxidative stress to the level of imbalance in the estrogen metabolism pathway as measured by the estrogen-DNA adducts. The significant interaction between changes in estrogen-DNA adduct ratio and compliance with the program suggests that the varying results could be a matter of adherence.
Despite the small sample size, analysis of these markers at two time points lends power to the study. This is evidenced by the finding that cysteine showed a positive change while GSH did not. GSH is more stable to oxidation than is cysteine, and levels of GSH are maintained within stringent parameters in plasma. 14 GSH levels are similar in women without breast cancer and with advanced breast cancer but are significantly different in women with early-stage breast cancer. 15 Therefore, the current results in 21 healthy women are consistent with previous reports showing that GSH measured in serum is resistant to measurable changes in oxidation state in short periods and that cysteine is more labile.
The means and standard deviations for the adduct ratio in this pilot study were similar to those in previous studies in which the means in control women ranged from 13.5 to 24.7 and standard deviations ranged from 8.9 to 32.0. 12,16,17 The significant reduction observed in this study after application of the AHBP in a healthy sample (Fig. 3) is remarkable given the sample size and the low levels of the adduct ratio at baseline. More dramatic effects are anticipated in women who are at higher risk for breast cancer because of genetic and other reproductive risk factors. Furthermore, this is the first study to show a significant reduction in the estrogen-DNA adduct levels in women who show improved management of oxidative stress. These initial findings warrant further investigation in a larger sample that includes both a control group and women who score higher on the Gail model scale or have a family history of hormonal cancers. Future studies using the AHBP are needed to validate reproducibility.
Evidence gathered in this study has the potential for development of a symptom indicator profile for breast health, which could expedite the clinical intervention process by efficiently identifying personalized areas of emphasis within the five key intervention activities.
Identification and reduction of measurable breast cancer risk factors through a defined, and potentially reproducible, clinical approach have the potential to maintain breast health and reduce the incidence of breast cancer by using easily attainable and cost-effective measures.
Footnotes
Acknowledgments
The authors thank Seth Adams of Xymogen Corp; Judy Dean, MD, of Santa Barbara Women's Imaging Center; Jim Hannah, MD, of Central Coast Pathology; Dean Jones and Yongliang Liang of Emory University School of Medicine; and Gaea Powel of Central Coast Thermography.
Author Disclosure Statement
No competing financial interests exist.