
Abstract
Introduction:
Patients with psoriasis often use botanical therapies as part of their treatment. It is important for clinicians to be aware of the current evidence regarding these agents as they treat patients.
Methods:
A systematic literature search was conducted using the PubMed, MEDLINE, and EMBASE database for randomized clinical trials assessing the use of botanical therapeutics for psoriasis. The search included the following keywords: “psoriasis” and “plant” or “herbal” or “botanical.” Citations within articles were also reviewed to identify relevant sources. The results were then further refined by route of administration, and the oral (systemic) botanical agents are reviewed herein.
Results:
A total of 12 controlled and uncontrolled clinical trials addressing the use of oral, systemic botanical agents for psoriasis were assessed in this review. While overall evidence is limited in quantity and quality, HESA-A, curcumin, neem extract, and, to a lesser degree, Traditional Chinese Medicine seem to be the most efficacious agents.
Conclusion:
The literature addresses a large amount of studies in regards to botanicals for the treatment of psoriasis. While most agents appear to be safe, further research is necessary for evidence-based recommendation of oral botanical agents to psoriasis patients.
Introduction
P
Up to 62% of patients with psoriasis turn to complementary and alternative medicine (CAM) to supplement or replace traditional treatments. 5 CAM agents include botanical treatments, Traditional Chinese Medicine (TCM), dietary supplements, climatotherapy, and mind–body interventions, of which botanical agents are most commonly used for psoriasis. 5,6 In addition to dissatisfaction with traditional Western treatments, patients may choose CAM therapeutics due to a perceived lower side-effect profile or a preference for “natural” agents. 7
Patient preference is an important part of a treatment decision, as the most effective treatments are those that the patient chooses to use on a regular basis. Patients may rely upon alternative therapies in addition to conventional therapies. A systematic review of the literature was performed in order to provide an up-to-date review of the current clinical evidence regarding the use of oral botanical agents for psoriasis. The review also aimed to identity which agents showed the most efficacy for use in psoriasis.
Methods
A systematic English-language literature search was conducted of PubMed, MEDLINE, and EMBASE through August 2016 to collect evidence-based data on the various botanical treatment modalities for psoriasis. Key search terms included (“botanicals,” “plants,” “herbs,” “traditional medicine,” “complementary medicine,” “Traditional Chinese Medicine,” or “Ayurveda”) and “psoriasis.” The initial search yielded 1973 articles. Selection criteria were limited to controlled and uncontrolled clinical trials testing only plant-based oral treatments for psoriasis. Blinding was not necessarily an inclusion criterion. Studies that were not in English, did not conduct trials on humans, or did not test plant-based treatments were excluded from the review. Reference lists in review articles were searched to identify any additional studies. 8 –10 Search terms were also used in combination. After critical evaluation of the remaining articles, 34 articles were selected that met criteria, and the review was further restricted to 12 articles that tested oral or systemic botanical agents. A flow chart depicting the selection criteria for trials is provided in Figure 1. Table 1 offers a comprehensive summary of each of the trials with different oral botanicals for plaque psoriasis.
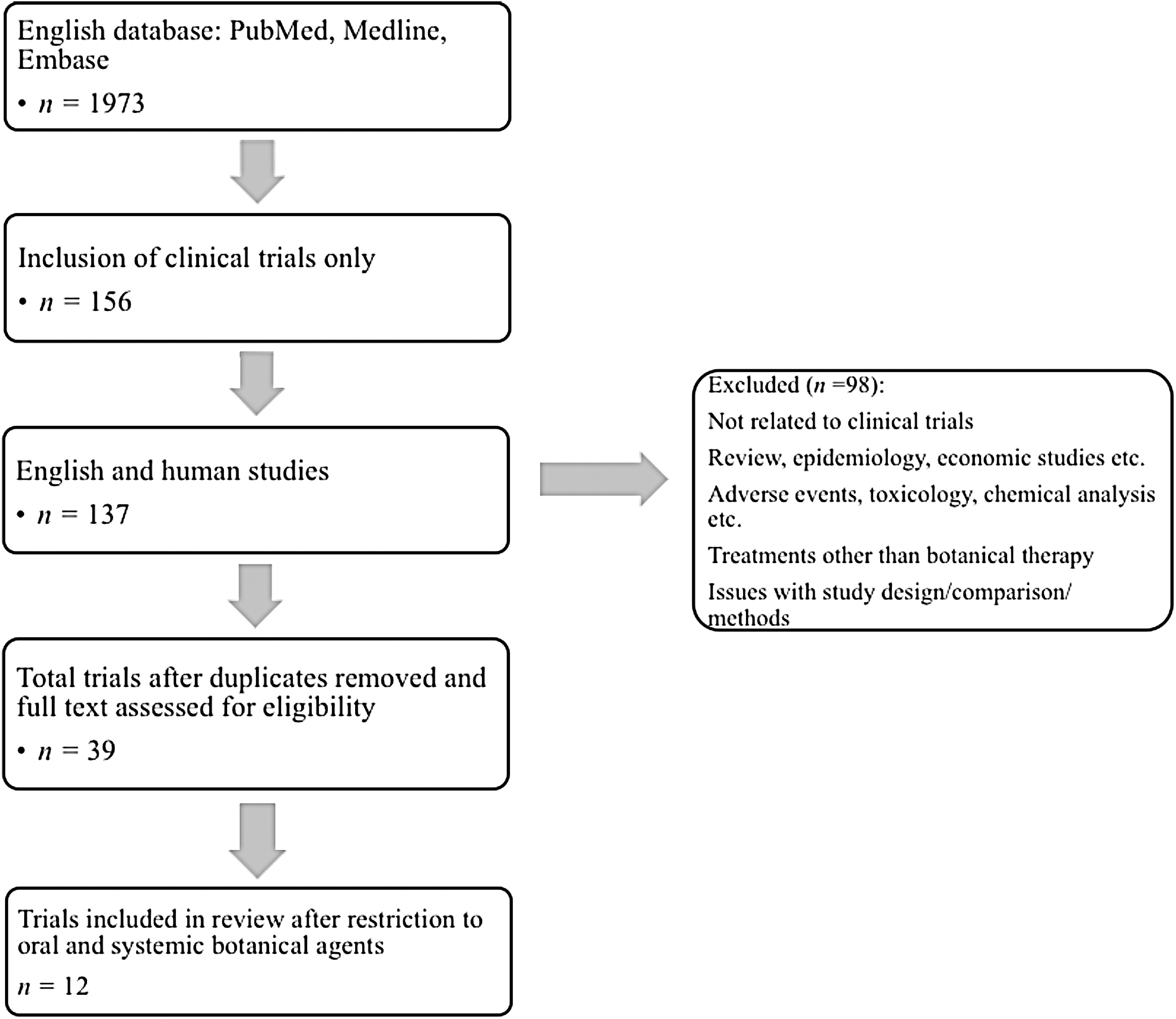
Flowchart of selection of clinical trials.
PASI, Psoriasis Area and Severity Index; DLQI, Dermatology Life Quality Index; PGA, Physician Global Assessment; TCM, Traditional Chinese Medicine; MTX, Methotrexate; N, number of subjects that were included in each trial; GI, gastrointestinal; TNF-α, tumor necrosis factor alpha; IL-8, interleukin 8.
Assessment of the quality of the clinical trials included in the review was determined by the score of Jadad et al. (Table 1). 11 The Jadad quality measure assigns a score to clinical trials that ranges from 0 to 5, where 0 indicates inferior quality and 5 indicates superior quality. It addresses three primary components for a trial: randomization, double-blinding, and a description of withdrawals or dropouts. Randomization and double-blinding gain an additional point each if there is a description of the methods used to form the randomization or the double-blinding.
Results
The studies were conducted in academic hospitals around the world. The countries represented were the United States, Israel, Italy, Iran, the United Kingdom, India, and China. The severity of psoriasis that was treated ranged from mild to severe chronic plaque psoriasis. Most trials used the Psoriasis Area and Severity Index (PASI) tool to measure the severity of psoriasis (ex. PASI 75 is the percentage of patients who achieve 75% improvement from their baseline score). The age of patients in these studies overall was at least 18 years.
Alga Dunaliella bardawil
D. bardawil is a specific type of motile, unicellular green algae that is found in marine waters. The algae accumulates high concentrations of β-carotene, a retinoid precursor with a safe adverse effect profile. 12 Synthetic retinoids have long been used for the treatment of psoriasis, but are limited by potential side effects. Greenberger et al. reported the results of a controlled clinical trial examining daily intake of one Dunaliella capsule compared to placebo capsule in 34 patients with mild, chronic plaque psoriasis. 13 After 6 weeks of treatment, there was a significantly higher reduction in the mean PASI score in the Dunaliella group compared with the placebo group (61.3% vs. 34%, respectively; p = 0.002). The difference in the Dermatology Life Quality Index (DLQI), however, was not significant. There were no significant changes in liver function tests or in lipid profiles among patients, and no adverse events were reported.
Marine oil and primrose oil
Essential fatty acids and their metabolites found in oils may be involved in the pathogenesis of psoriasis. Marine oil and primrose oil, rich in omega-3 and omega-6 fatty acids, respectively, may have the ability to reduce the production of proinflammatory eicosanoids that are involved in the pathogenesis of psoriasis. Oliwiecki and Burton reported the results of a clinical trial comparing combination marine oil and evening primrose oil to placebo in 37 patients with chronic stable plaque psoriasis. 14 All patients received placebo capsules for the first 4 weeks of the study and were then randomized to continue placebo or take the trial medication, 12 capsules daily for 24 weeks. While no adverse effects were reported, the researchers did not note any significant improvement in the clinical severity of psoriasis with the combined marine oil and primrose oil capsules (p > 0.05).
Curcumin
Curcumin (dihydroferuloyl-methane), the active ingredient found in the spice turmeric, may have utility in the treatment of psoriasis by acting on the main component of psoriasis pathogenesis, T cell mediated inflammation. It is thought to inhibit nuclear factor kappa B (NF-κB), keratinocyte proliferation, phosphorylase kinase, and angiogenesis. 15 Kurd et al. performed an uncontrolled clinical trial assessing the efficacy of curcumin capsules, 4.5 g daily for 12 weeks, in 12 patients with moderate to severe plaque psoriasis. 16 Only two subjects achieved PASI 75 or a PGA of excellent at week 12. Adverse events included gastrointestinal upset or heat intolerance. Antiga et al. reported the results of a clinical trial on methylprednisolone aceponate 0.1% ointment with adjuvant curcumin tablet compared to methylprednisolone aceponate 0.1% ointment with placebo tablets in 63 patients with mild to moderate plaque psoriasis. 17 Patients were divided into two arms: arm 1 received methylprednisolone ointment, once daily on the lesions, plus 2 g per day of curcumin tablets, while arm 2 received methylprednisolone ointment and placebo for 12 weeks. At 12 weeks, both arms had significant improvement in median PASI compared with baseline (p < 0.05). However, reduction of PASI was higher in arm 1 (curcumin) than it was in arm 2 (placebo) patients (p < 0.05). One patient in arm 1 had diarrhea.
HESA-A
HESA-A is a compound manufactured and available in Iran. HESA-A is composed of mineral constituents (50%), organic herbal constituents (45%), and water (5%). The herbal components include Carum carvi (Persian cumin) and Apium graveolens (celery). This compound has anticancer effects, and may have anti-inflammatory and anti-proliferative properties that could be used in the treatment of psoriasis. 18 Ahmadi et al. reported the results of a controlled clinical trial comparing HESA-A to placebo in 28 patients with chronic plaque psoriasis. 19 Patients were assigned to take either a 25 mg/kg HESA-A tablet or placebo tablet twice daily for 6 months. After 6 months, researchers noted that 64.2% had clearance of psoriatic plaques and 35.8% had mild disease remaining in the HESA-A group, while the placebo group showed no disease improvement. Barikbin et al. performed an uncontrolled trial on HESA-A with 19 patients with chronic plaque psoriasis. 20 Patients took a 30 mg/kg tablet daily for 4–30 weeks. At the conclusion of the study, the PASI score had decreased in 73.7% of patients but increased in 26.3%. The only statically significant correlation was between the duration of treatment and PASI improvement (p = 0.024). No adverse events were reported in either study.
Neem
Azadirachta indica, also known as neem, is an evergreen tree that is native to India, where it has long been used for agricultural and medicinal purposes. One of the major components of neem leaf is nimbidin, which is believed to have hypoglycemic, anti-ulcer, and antitumor effects, and is a more effective inhibitor of prostaglandin synthetase than acetyl salicylic acid. 21 Pandey et al. reported the only clinical trial assessing the use of neem for plaque psoriasis. 22 The trial involved 50 patients with uncomplicated plaque psoriasis who were instructed to take either placebo or neem leaf extract capsules three times daily with the addition of a topical regimen that included 5% crude coal tar and 3% salicylic acid in a Vaseline base for 12 weeks. While both groups showed decreased PASI scores indicative of response to the topical regimen at treatment endpoints, the mean PASI score was significantly better for the neem group compared with the placebo group at 8 weeks (9.7 vs. 12.24, respectively; p < 0.05) and 12 weeks (4.74 vs. 9.47, respectively; p < 0.001). No adverse events were reported.
Tripterygium wilfordii Hook F
T. wilfordii Hook F (TwHF) is a Chinese herb that is commonly used for inflammatory and immune disorders, especially in China. Triptolide is the most known potent active ingredient in the herb extract and has immunosuppressive and anti-inflammatory effects in vitro and in animal models. 23 Wu et al. reported the results of a controlled clinical trial comparing TwHF to acitretin in 115 patients with moderate to severe plaque psoriasis. 24 Patients were instructed to take TwHF 20 mg three times a day plus a placebo tablet or acitretin 30 mg once a day along with a placebo tablet for 8 weeks. At the end of the treatment, median PASI score improved in the TwHF group by 50.4% compared with baseline (p < 0.0001) and in the acitretin group by 42.7% compared with baseline (p < 0.0001). The difference in median PASI improvement between the groups was not significant (p = 0.317). No serious adverse events occurred, though the TwHF group noted elevated levels of aspartate transaminase and triglycerides, while the acitretin group noted elevated alanine transaminase, cholesterol, and high-density lipoprotein.
TCM
A frequently selected alternative therapy in China and Taiwan, TCM has been used to treat psoriasis for centuries. 25 Consisting of both topical and oral formulations, TCM utilizes a mixture of many herbs and many formulations tailored to each patient. Many of the Chinese herbs have been used in the treatment of psoriasis, and possess anti-inflammatory properties and abilities to modulate cytokine production or inhibit angiogenesis. 26 Four clinical trials available in the literature fit the criteria for this review. Song et al. conducted an uncontrolled clinic trial with 15 patients with plaque psoriasis assessing both an oral and topical regimen of TCM. An oral decoction was taken twice daily, which consisted of Rhizoma Smilacis Glabrae, Folium Isatidis, Rhizoma Menispermi, Oldenlandia,Rhizoma Curcumae, Rhizoma Polygoni Cuspidati, Cornu Saigae Tataricae, Gypsum Fibrosum, Herba Solani Lyrati, and Herba Duchesneae Indicae. 27 Topical treatment included both a herbal bath and applying a herbal ointment twice a day. The bath consisted of Cacumen Platycladi, Rhizoma Curcumae, and Nepal dock root, and the ointment was made from Rhizoma Curcumae oil and Galla Chinensis extract. After 3 months of treatment, patients with both acute and chronic disease showed significant decreases in PASI score and plaque index (p < 0.01). In the largest clinical trial, Dai et al. reported the results comparing Yinxieling decoction (consisting of radix rehmanniae recen, angelica sinensis, radix paeoniae rubra, ligusticum wallichii, radices lithospermi, curcuma zedoary, chloranthus spicatus, rhizome smilacis glabrae, smoked plum, liquorice, and others) to placebo in 120 patients with plaque psoriasis. 28 The decoction or placebo was ingested twice daily for 8 weeks. After 8 weeks, there was a significant decrease in the PASI score compared with baseline (p < 0.05) in patient groups taking the decoction, while no significant decrease was noted in the placebo group. Ho et al. reported the results of a controlled clinical trial comparing an oral TCM (consisting of indigo naturalis, ephedra, ginger, cinnamon, mustard seed, and others) to methotrexate (MTX) and placebo in 61 patients with chronic plaque psoriasis. 29 Patients took either TCM capsules, MTX (up to 30 mg/week), or placebo weekly for 6 months. After 6 months, improvement was 73.9% for the MTX group, 15.1% for the TCM group, and 32% for the placebo group compared to each respective baseline. MTX was significantly more effective than TCM and placebo, while no significant difference was noted between TCM and placebo groups. Adverse events were reported by 65% of the MTX group, 48% of the TCM group, and 30% of the placebo group. The most common reported events in the MTX group included gastrointestinal upset and liver enzyme abnormalities, while the TCM and placebo groups reported increased incidence of infections and liver function abnormalities. It should be noted that the botanicals selected for this study differ in their traditional nature and function from the other studies. According to TCM, psoriasis is considered a hot disease and is most often treated with cold medicinal agents. Ho's group selected ephedra, ginger, cinnamon, and mustard seed, which are all considered in TCM theory to be hot in nature. Zhang et al. conducted a controlled clinical trial comparing an oral TCM (consisting of dandelion, forsythia fruit, isatis, imperata rhizome 30 g, and others) to acitretin combined with the same TCM in 80 patients with plaque psoriasis. 30 Patients were divided into two groups, with group A taking an acitretin 20–30 mg capsule and TCM capsule, and group B taking a TCM capsule once daily for 8 weeks. After 8 weeks, PASI scores significantly improved in both groups compared with each respective baseline (p < 0.01), with no significant difference between groups. However, group A had greater total efficacy compared with group B (p < 0.01). The most common adverse events associated with TCMs were gastrointestinal upset, with diarrhea being most common.
Discussion
Psoriasis is a notoriously difficult-to-treat chronic skin condition. In a recent psoriasis survey, 25% of dermatologists reported management of psoriasis patients as complicated, and 68% felt that psoriasis patients needed more time and support than other patients did. 3 Dermatologists treating moderate to severe psoriasis have undoubtedly encountered patients who have inquired about alternative therapeutics to traditional Western medicine. In the same psoriasis survey, 87.8% of patients and 98% of dermatologists felt a strong or moderate need for better psoriasis treatments. 3 As increasing amounts of patients look to CAM modalities to offer relief for their psoriasis, dermatologists should become familiar with evidence-based recommendations for different CAM options. A systematic review of the literature was performed for clinical trials investigating oral botanical therapeutics in the treatment of plaque psoriasis.
This review of both controlled and uncontrolled clinical trials in the literature revealed that the most highly studied oral, systemic botanicals include TCM with four studies, curcumin with two studies, and HESA-A with two studies. Though studies were limited and reliability of the data was low, the oral agents that demonstrated the most efficacious potential include HESA-A, curcumin, and neem extract. TCM was more effective in three out of four studies and thus may have potential for psoriasis treatment as well. Before any of these agents are routinely recommended to patients, further large controlled clinical trials are necessary to evaluate efficacy and safety better.
The most common adverse event for the oral botanicals was gastrointestinal intolerance. Diarrhea was noted as a side effect with curcumin and TCM. Accounts of serious adverse events were absent in most studies or very low in a few, with the most concerning effects including an increased incidence of infections in a specific TCM concoction and significant increase in the level of aspartate transaminase and triglycerides with T. wilfordii Hook. Due to the small duration of use for some herbals, the small size of most studies, questionable reporting, and methodologic weaknesses, strong conclusions cannot be made. There have been several case reports of more concerning cutaneous conditions, nonspecific for treating psoriasis, including lichenoid drug eruptions from oral botanical agents. 31,32
Limitations to this review must be considered. Unpublished/unavailable studies, case reports, case series, retrospective studies, or reports in languages other than English were not included. Many of the clinical trials included cannot be held to the highest methodologic reporting standards, as only one study met criteria for a Jadad score of 5. Another limitation is that there is no confirmation that the products are pure and unadulterated, and the purity of the products used in the studies could not be confirmed. Not every study included utilized a PASI score to measure improvement in psoriasis, making it difficult to compare studies that utilized it against those that did not. Many of the reviewed studies were pilot studies with small sample sizes, and more definitive conclusions require further study in a larger population of patients. Additionally, four of the studies included did not compare treatment to placebo, making it difficult to draw conclusions on efficacy.
In conclusion, while CAM therapeutics demonstrate potential for treatment of psoriasis, the evidence is still in its infancy. As the attention and demand for CAM treatments increase, it becomes critical for dermatologists to be aware of the evidence-based recommendations of efficacy and adverse events with regards to these treatments. Given the early potential benefit that some CAM agents have shown in this review, further rigorous randomized controlled trials are warranted.
Footnotes
Author Disclosure Statement
To the best of our knowledge, no conflicts of interest, financial or other, exist. This manuscript has not been previously published and is not under consideration in the same or substantially similar form in any other peer-reviewed media.