
Abstract
Purpose:
The purpose of this study was to investigate the safety of daiobotampito in the treatment of acute diverticulitis of the colon.
Methods:
We conducted a single-center, open-label, prospective study. Ten patients who suffered from diverticulitis of the colon were recruited. The patients were treated with fasting, antibacterial agents, and daiobotampito extract for 10 days in or out of hospital. The patients individually recorded their body temperature, grade of abdominal pain, number of times that analgesics were used, and number of stools daily. We checked whether the patients had adverse reactions such as abdominal pain or diarrhea.
Results:
No patients experienced serious adverse reactions. One patient had moderate abdominal pain and diarrhea soon after daiobotampito intake. This patient discontinued daiobotampito on day 4, and the pain and diarrhea quickly resolved. The abdominal pain of this patient was worse 6 days before treatment, and the pain was almost relieved with initial daiobotampito treatment.
Conclusions:
Daiobotampito is a safe treatment option for early stage, acute diverticulitis.
Introduction
A
Ogawa et al. reported the efficacy and safety of daiobotampito (Da Huang Mu Dan Tang in Chinese), one formula of Japanese traditional Kampo medicine, in the treatment of acute diverticulitis retrospectively, but its safety has not been investigated prospectively. 6 We prospectively investigated the safety of daiobotampito in the treatment of acute diverticulitis of the colon.
Methods
Trial design
This single-center, open-label, prospective study was conducted as a phase II trial at the Tokyo Saiseikai Central Hospital. The study protocol was approved by the Research Ethics Committee of the Tokyo Saiseikai Central Hospital. Written informed consent was obtained from all participants before beginning the study. The study was conducted in accordance with the Declaration of Helsinki. Study registration with the University Hospital Medical Information Network Center clinical trial registry (UMIN-CTR, number UMIN000014808; available at
Participants
Patients who suffered from diverticulitis of the colon were recruited at the Tokyo Saiseikai Central Hospital in Tokyo, Japan. They were diagnosed with ultrasound and computed tomography (CT). We excluded patients less than 20 years or more than 75 years old, patients who needed surgical intervention and/or intensive care, or patients in a fragile condition, such as chronic anorexia, chronic diarrhea, insulin dependent diabetes mellitus, pregnancy, puerperium, immunodeficiency, and kidney deficiency (estimated glomerular filtration rate [eGFR] less than 20 mL/min/1.73 m2). Patients allergic to daiobotampito were also excluded.
Study procedures and intervention
All participants underwent blood, ultrasound, and a CT scan to evaluate diverticulitis severity on day 1 (Fig. 1). Patients were treated with fasting, antibacterial agents (intravenous ampicillin/sulbactam or oral amoxicillin/clavulanate), and 7.5 g of daiobotampito extract per day (TJ-33; Tsumura & Co, Tokyo, Japan) for 10 days in or out of the hospital. 7 Patients were permitted to use loxoprofen as an analgesic agent. The patients received intravenous feeding or drank electrolytic solution of at least 1500 mL per day. Doctors determined, based on the patient's condition, the day that patients could resume eating. We followed the patients for 11 days. Patients independently recorded their body temperature, grade of abdominal pain from 0 (no pain) to 10 (max during diverticulitis episode), number of times that analgesics were used, and number of stools daily. If they suffered from strong abdominal pain, they stopped daiobotampito.
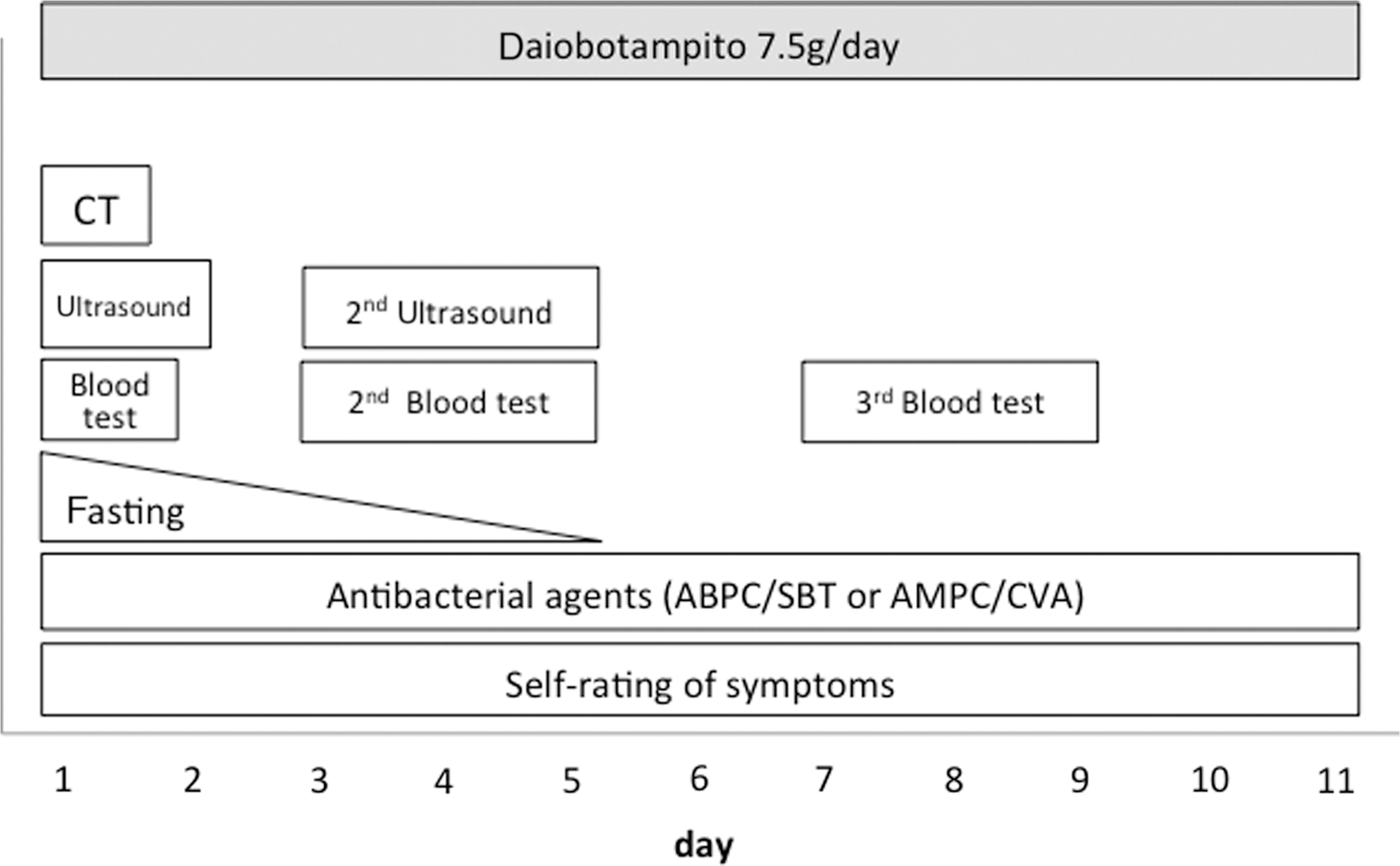
Study procedure and intervention. CT, computed tomography.
Doctors of Kampo medicine usually evaluate patients' medical conditions and physical strength before daiobotampito administration to determine the appropriate dosage. However, in this trial, the doctors did not evaluate the patients' conditions in the Kampo manner; rather, they used TSUMURA daiobotampito extract granules according to the dosage listed on the drug package insert. 7
Materials: Daiobotampito
Daiobotampito is traditionally used to treat intestinal inflammation and as a laxative agent. We used daiobotampito extract granules (TJ-33; Tsumura & Co). 7 TJ-33 contains 3.5 g of a mixture containing dried Benincasa seed extract (Benincasae Semen) 6.0 g, peach kernel (Persicae Semen) 4.0 g, moutan bark (Mutan Cortex) 4.0 g, rhubarb (Rhei Rhizoma) 2.0 g, and anhydrous mirabilitum 1.8 g.
Endpoints
We assessed, as a primary endpoint, whether the patients had adverse reactions such as abdominal pain or diarrhea, per the Common Terminology Criteria for Adverse Events (CTCAE) version 4.0. We also determined, as secondary endpoints, periods of abdominal pain, use of analgesic agents, occurrence of fever (more than 37.0°C), number of stools, C-reactive protein (CRP), white blood cell count (WBC), size of abscesses, deteriorations of diverticulitis, discontinuation of daiobotampito, continuation of antibacterial agents, and days until patients resumed eating.
Sample size
The authors determined that 10 patients indicated an appropriate number for this pilot study; however, the authors are aware that this number is limited. A phase III trial will be planned in the future.
Results
Ten participants (seven men and three women) were enrolled between September 2014 and March 2015 and treated with daiobotampito (Table 1). The patients had no serious adverse reactions, such as CTCAE grade 4 (life-threatening consequences or urgent intervention indicated) or 5 (death related to adverse events). One out of the 10 patients had CTCAE grade 2 abdominal pain (moderate pain-limiting instrumental activities of daily living) and CTCAE grade 2 diarrhea (increase of four to six stools per day over baseline; moderate increase in ostomy output compared with baseline) soon after daiobotampito intake. This patient discontinued daiobotampito on day 4. Pain and diarrhea quickly resolved with discontinuation. Abdominal pain was worse 6 days before treatment, and the pain was almost relieved when the patient was initiated daiobotampito. The other nine patients had strong diverticulitis-related abdominal pain when initiating daiobotampito, and these patients did not have adverse reactions.
CRP, C-reactive protein; WBC, white blood cell count.
Five patients experienced reduced pain (pain scale ≦5) by day 3 (Fig. 2). Three patients had pain (pain scale ≧1) until day 11. Two patients used analgesics for diverticulitis pain. One used analgesics on day 1 only, and the other used analgesics until day 7. Four patients were febrile (≧37.0°C) on initiation of the treatment. Only one of these patients was febrile on day 2, and all patients were afebrile after day 3. Stool frequencies were 0 to 8 per day, but the patients felt no serious symptoms other than the patient who stopped daiobotampito (Fig. 3). CRP, WBC, size of abscesses, and other diverticulitis conditions of all patients did not deteriorate after administration of daiobotampito. No patients continued antibacterial agents after day 11. The patients resumed eating on days 3 to 6. No patients' blood parameters, such as aspartate aminotransferase, alanine aminotransferase, and creatinine, worsened after daiobotampito intake.
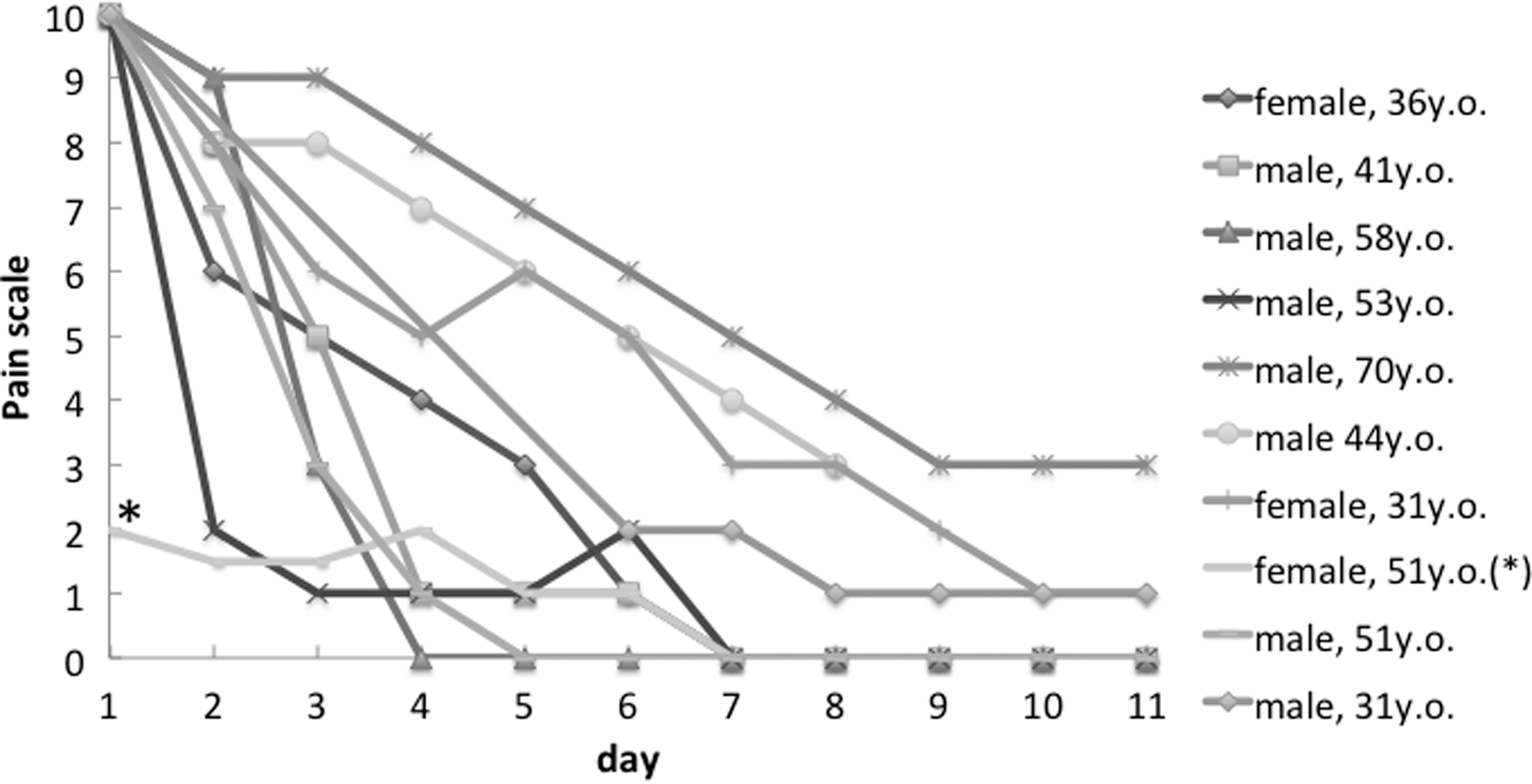
Pain after daiobotampito administration. Fifty-one-year-old woman (*) stopped daiobotampito intake because of diarrhea.
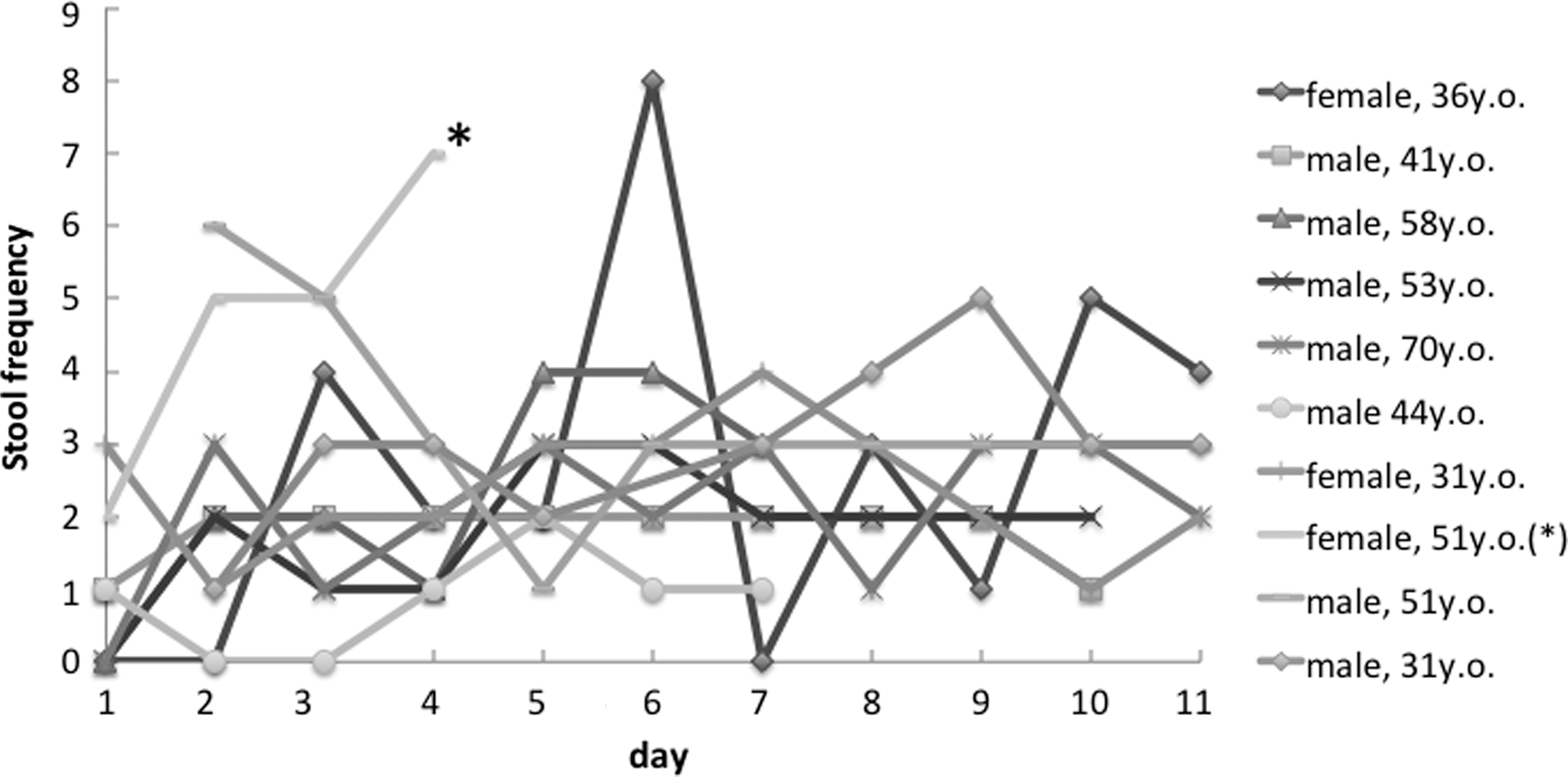
Stool frequency after daiobotampito administration. Fifty-one-year-old woman (*) stopped daiobotampito intake because of diarrhea.
Discussion
The primary purpose of this study was to determine the safety of daiobotampito as a treatment for diverticulitis. We showed, prospectively, that early stage diverticulitis associated with strong pain could be treated safely with daiobotampito. We also demonstrated that patients with almost cured diverticulitis might get diarrhea and abdominal pain with administration of daiobotampito.
Daiobotampito (Da Huang Mu Dan Tang in Chinese) was described in “Jin Gui Yao Lue” (Kinkiyoryaku in Japanese), which means “prescriptions from the golden cabinet.” Jin Gui Yao Lue was written in ancient China and is a basic and an important book in traditional Asian medicine. Traditionally, daiobotampito has been used for intestinal inflammation and abscesses, such as diverticulitis, appendicitis, and perianal abscess. However, it is currently used infrequently, and there are few studies about daiobotampito. Only three reports about daiobotampito were located in PubMed on May 18, 2016. 6,8,9
Daiobotampito consists of five crude drugs: Rhei Rhizoma, Moutan Cortex, Persicae Semen, Benincasae Semen, and anhydrous mirabilitum. Rhei Rhizoma, the rootstock of Rheum palmatum, is the main crude drug of daiobotampito. Rhei Rhizoma contains sennosides, rheinosides, anthraquinones, and lindleyins and has purgative, antibacterial, and anti-inflammatory effects. 10,11 Sennosides and rheinosides work as purgatives, so Rhei Rhizoma is presently used mainly as a purgative agent. 11,12 However, in ancient China, it was used to mitigate inflammation, such as that caused by infection. 13 Anthraquinones, including rhein, aloe-emodin, and emodin, work as antibacterial and antifungal agents. Cyong et al. reported the antimicrobial activity of rhein for Bacteroides fragilis and Candida albicans, which are two important pathogens in the intestinal flora of humans. 14 Anthraquinones and lindleyins work as anti-inflammatory agents. 15 –19
In this study, daiobotampito was not a strong purgative agent in patients with strong inflammation of diverticulitis, such as strong abdominal pain. Daiobotampito was a strong purgative agent only in patients with weak inflammation. The functions of Rhei Rhizoma might vary depending on the condition of the intestine, such as inflammation and gastrointestinal microbiome. Possibly, daiobotampito behaves as an antibacterial and anti-inflammatory agent in early stage diverticulitis, but it may behave as a purgative agent in late-stage diverticulitis or without inflammation of the colon.
Moutan Cortex, the root cortex of Paeonia suffruticosa, contains paeonol, paenoside, paeonolide, paeoniflorin, oxypaenolniflorin, benzoylpaeoniflorin, benzoyl-oxy-paeoniflorin, and apipaeonoside and possesses anti-inflammatory and anti-allergic activity. 20 –23 The compounds of Moutan Cortex reduce the production of histamine, nitric oxide (NO), and prostaglandin E2 (PGE2). Furthermore, the Moutan Cortex compounds reduce the expression of inducible nitric oxide synthase (iNOS), cyclooxygenase-2 (COX-2), tumor necrosis factor-α (TNF-α), interleukin-1β (IL-1β), interleukin-6 (IL-6), interleukin-8 (IL-8), and phosphorylated inhibitor of IκBα, and the activation of nuclear factor (NF-κB).
Persicae Semen, the seed of Prunus persica, contains amygdalin, glycosides, prunasin, sterols, and emulsin and has anti-edema, lenitive, and anti-inflammatory activities. 24,25
Benincasae Semen is the seed of Benincasa cerifera. Benincasa cerifera is also called Benincasa hispida and has been used in traditional medicine in East and South Asia. In South Asia, the fruit of Benincasae cerifera is used to treat edema, insanity, epilepsy, gastrointestinal problems, and infectious disease. 26,27 In East Asia, the seed of Benincasae cerifera is used to treat inflammation and hypertension. 28 It can serve as an inhibitor of angiotensin-converting enzyme and angiogenesis, and as an antioxidative, antipyretic, analgesic, and antimicrobial agent. 29 –31
Anhydrous mirabilitum acts as a stool softener and enhances the purgative effect of Rhei Rhizoma. 32
As shown in a previous study, daiobotampito was possibly effective at accelerating diverticulitis recovery and preventing recurrence. 6 In this study, participants' diverticulitis pain was reduced after treatment, but it remains unclear whether daiobotampito was effective for diverticulitis. In a subsequent study, we need to prospectively examine the efficacy of daiobotampito in treating incipient diverticulitis, excluding patients who do not have strong diverticulitis pain.
Diverticulitis is sometimes treated with nonabsorbable antibiotics, probiotics, and anti-inflammatory medication by mesalazine (5-amino-salicylic acid). 33,34 The efficacy of nonabsorbable antibiotics and probiotics for diverticulitis is not clear. The efficacy of mesalazine is not clear in acute diverticulitis, but it may reduce symptoms in the chronic phase and recurrence. Daiobotampito also serves as an anti-inflammatory medicine like mesalazine, so it may reduce recurrence of diverticulitis.
Conclusion
Daiobotampito is a safe treatment option for acute, early stage diverticulitis.
Footnotes
Author Disclosure Statement
No competing financial interests exist.