
Abstract
Objective:
To evaluate whether tuina is more effective and cost-effective in reducing pain compared to no intervention in patients with chronic neck pain.
Design:
Single-center randomized two-armed controlled trial.
Setting:
University outpatient clinic specialized in Integrative Medicine.
Subjects:
Outpatients with chronic neck pain were randomly allocated to tuina or no intervention.
Intervention:
Six tuina treatments within 3 weeks.
Outcome measures:
The primary outcome was the mean neck pain intensity during the previous 7 days on a visual analogue scale after 4 weeks (VAS, 0–100 mm, 0 = no pain, 100 = worst imaginable pain). Secondary outcomes included Neck Pain and Disability Scale (NPDS), Neck Disability Index (NDI), health-related quality of life (12-item quality-of-life questionnaire [SF-12]), medication intake, and cost-effectiveness after 4 and 12 weeks. Statistical analysis included analysis of covariance adjusted for baseline values and a full economic analysis from a societal perspective.
Results:
Altogether, 92 outpatients were included (46 in both groups, 87% female, mean age 45.4 [standard deviation ±9.7], and mean VAS 57.7 ± 11.5). Tuina treatment led to a clinically meaningful reduction in neck pain intensity (group differences, 4 weeks: −22.8 mm [95% confidence interval, −31.7 to −13.8]; p < 0.001 and 12 weeks: −17.9 mm [−27.1 to −8.8], p < 0.001). No serious adverse events were observed. Total costs as well as quality-adjusted life years (QALYs) did not differ significantly between the groups. When taking group differences into account independently from their statistical significance, costs per QALY gained (incremental cost-effectiveness ratio) would range within a cost-effective area from €7,566 (for costs €10.28 per session) to €39,414 (cost €35 per session).
Conclusion:
An additional treatment with six tuina sessions over 3 weeks was effective, safe and relatively cost-effective for patients with chronic neck pain. A future trial should compare tuina to other best care options.
Introduction
N
Nonspecific neck pain can be treated with medication as well as stretching and strengthening exercises, massages, and heat and cold applications. 4,9 People with chronic pain might benefit from additional pain management programs. 4,9
Tuina therapy is also known as Chinese massage 10 and often used by Chinese patients with neck pain. It is also increasingly popular in the West. As a part of Traditional Chinese Medicine, tuina combines a manual therapeutic approach and anatomical and physiological principles, and emphasizes the meridians and acupoints. 11 Tuina therapy uses mainly two components: soft tissue manipulation and backbone manipulation. The soft tissue techniques include stroking, kneading, and drumming, which are also found in some western massage techniques. The backbone manipulation techniques use manual operation procedures with or without high-velocity low-amplitude thrust manipulation techniques. 11 According to recent reviews high-quality randomized controlled trials (RCTs) are needed to provide evidence about the effectiveness of tuina. 10,11
The aim of our trial was to evaluate whether tuina is more effective and cost-effective than no intervention in reducing neck pain measured on a visual analogue scale (VAS) in patients with chronic neck pain.
Materials and Methods
Design
We performed a two-armed randomized controlled trial comparing tuina treatment with a no-intervention waiting list control. Treatment duration was 3 weeks. The primary outcome was recorded after 4 weeks; a follow-up measurement was performed after 12 weeks.
This study (
Participants and setting
Patients were recruited by the Institute for Social Medicine, Epidemiology, and Health Economics using the institute's website and information materials such as leaflets from August 2013 to March 2014. Patients were informed about the study design and the possibility of being randomly assigned to the no-intervention control group.
After inclusion into the study, participants were randomized into one of two groups (tuina or no-intervention control) in a 1:1 ratio by block randomization with variable block length. The randomization list was generated using SAS/BASE software v9.3 (SAS Institute, Cary, NC) by a statistician who was not further involved in the study.
The list was integrated into a secure Microsoft Office Access 2010 database (Microsoft Corporation, Redmond, WA), where it was implemented in the background, which was not accessible to anyone involved in randomization or treatment. Patients who provided informed consent and fulfilled the eligibility criteria were registered by the therapist in the preface of the database in a consecutive order. After baseline data were obtained, the therapist randomized the patients by pressing a button within this database and provided the results to the patient immediately afterward. Patients could not be changed or deleted in the database, which ensured consecutive order and concealed randomization.
Patients of both gender were eligible for the trial if they fulfilled the following inclusion criteria: age 18–60 years, average pain intensity, during the previous 7 days, more than 40 mm on a VAS (0–100 mm), and clinical diagnosis “chronic neck pain,” with neck pain for at least 12 weeks. If additional back pain was reported, neck pain had to be predominant. Patients had to be mentally and physically able to participate in the study and had to give written informed consent.
Patients were not eligible if they fulfilled any of the following exclusion criteria: neck pain caused by a malignant disease; neck pain caused by trauma; rheumatic disorder; prior spinal column surgery; neurological symptoms, for example, radicular symptoms because of a prolapsed vertebral disc; suspected osteoporosis; obesity with body mass index ≥30 kg/m2; known vascular anomaly such as aneurysm; regular intake of analgesics (>1 × per week) because of additional diseases; intake of centrally acting analgesics; current application for a benefit; pregnancy; severe acute and/or chronic disease that did not allow participation in the therapy; other limitations that did not allow participation in the therapy; alcohol or substance abuse; tuina treatment during the previous 6 months before study entry; participation in another clinical trial during the 6 months before the study or parallel to the study; anticipated new treatments during the study, which have a positive influence on the neck pain such as physiotherapy against neck pain, acupuncture, and massage; and no sufficient German language skills.
Intervention
Patients in the tuina group received tuina in a series of six sessions within 3 weeks with two sessions per week. One treatment session lasted about 30 min. For the treatment, the patient was seated in a chair and treated from distal to proximal. In the first part, meridian points were manipulated and wrist, elbow, and shoulder joints were mobilized. In the following, the neck region was treated with soft tissue massage, local muscle stretching, mobilization and traction of the cervical spine, and manipulation of local pain (trigger) points (see also Supplementary Table S1; Supplementary Data are available online at
Patients in the no-intervention group did not receive a study intervention. After the end of the study, patients of this group could choose to receive a series of six tuina sessions free of charge. However, this intervention was offered to increase motivation, and was not part of the evaluation.
In both groups, new interventions, supposed to have a positive effect on chronic neck pain (e.g., acupuncture therapy, sport therapy, or relaxation), should not be started during the study. All patients could continue their respective prestudy therapy during the study. Concomitant treatments were recorded at 4 and 12 weeks.
Outcome measurements
The primary outcome measure was the average neck pain intensity during the previous 7 days on a visual analogue scale (VAS, 0–100 mm, 0 = no pain and 100 = worst imaginable pain) 13 after 4 weeks.
Secondary outcome measures included the VAS for average neck pain during the previous 7 days at 12 weeks and the following outcomes at 4 and 12 weeks: Neck Pain and Disability Scale (NPDS), 14,15 Neck Disability Index (NDI), 16 –18 12-item quality-of-life questionnaire (SF-12) health-related quality of life, 19 body efficacy expectation, 20 medication intake, and cost-effectiveness. In addition, we evaluated the safety of the interventions. Adverse events associated with the therapy (adverse reactions) and all serious adverse events were recorded at each visit by the therapist. The data were collected by paper-based questionnaires.
Statistical analysis
The study was designed to detect a mean difference of 20 mm on the primary outcome (average VAS during the previous 7 days after 4 weeks) between the tuina group and the no-intervention waiting list group, with a pooled standard deviation of 30 mm (medium effect size according to Cohen's d = 0.67), a t test with a power of 80%, and a two-sided significance-level of 0.05. For this, 37 participants per group were needed (74 in total). Taking 19% potential dropouts into account, 88 participants (44 per group) were planned to be randomized.
The primary analysis population followed an intention-to-treat principle, and included all patients who were randomized and whose data were available for the respective outcome. Missing values were not imputed for the primary analysis. For the primary analysis of the primary endpoint, we used an analysis of covariance (ANCOVA), including the treatment variable (tuina and no-intervention waiting list; fixed effect), and adjusted for baseline-VAS-value (covariate). We used a significance level of 5% (two sided). Results are reported as adjusted group means with 95% confidence intervals and p-values for the group comparison. For a better comparison, Cohen's d was calculated for neck pain intensity after 4 and 12 weeks. All further analyses on the primary outcome and all secondary outcomes are considered explorative. Secondary outcomes were analyzed similar to the primary analysis of the primary outcome, that is, ANCOVA, or logistic or Poisson regression (depending on the scale and distribution of the data), adjusted for the respective baseline value (when available) and additional covariates in case of group imbalances.
A number of sensitivity analyses were performed. A per-protocol analysis with the following population was performed for the primary outcome: six treatments in the first 3 weeks, no missing data for the primary outcome, no new co-intervention for neck pain started during the study, no withdrawal from the study, and no exclusion criterion detected after randomization. Missing data were imputed using multiple imputation techniques based on fully conditional specification, using a Markov Chain Monte Carlo (MCMC) algorithm. For this imputation, the variables VAS after 4 weeks, baseline-VAS, NDPS, NDI, SF-12, body-efficacy expectation, duration of neck pain, age, and sex were used. Furthermore, mixed models for repeated measures were used to compare the groups with respect to changes in the primary outcome over time. The model included terms for treatment and time as fixed main effects, an interaction term for treatment by time, the baseline value as covariate, and the subject as a random effect.
We calculated cost-effectiveness for all randomized patients with complete economic data and utility values from a societal perspective. Since the intervention effects were considered in terms of quality of life changes, the cost-effectiveness assessment was conducted as a cost-utility analysis using quality-adjusted life years (QALYs) as outcome. To calculate QALYs, we converted SF-12 values into health-state utilities using an algorithm published by Brazier and Roberts.
21
Taking into account the individual study duration, QALYs were obtained by using the area under the curve method
22
subsequently. In case of additional QALYs and higher costs compared to control patients, the cost-effectiveness of tuina was calculated as the ratio of group differences in disease-related costs and the group differences in QALYs, the so-called incremental cost-effectiveness ratio (ICER):
The ICER reflects the additional costs of one additional QALY in the intervention group compared to the control patients. In health economic studies, particularly in Western Europe, a threshold of 50,000 Euro per QALY gained is often used to decide whether an intervention is cost-effective or not. An intervention can be seen as cost-effective if the realization of one additional QALY is reachable with less than 50,000 Euros. Thus, the threshold is often described as society's willingness to pay for one extra QALY. We used this threshold to reach a better comparability with international study results. Scenario analyses were realized to evaluate the robustness of the results under varying assumptions. Since tuina is not regularly reimbursed by German statutory health insurance yet, we assumed a hypothetical cost per session ranging from 10.28 € (scenario 1) to 35 € per session (scenario 2). Scenario 1 reflects the mean reimbursement rate for classical massage therapy. 23 Scenario 2 corresponds to the fees recommended by the Federation of German Healing Practitioners. 24
For the analysis, we used SPSS 20.0 or higher (SPSS, Inc., Chicago, IL) and SAS for Windows, Version 9.2 or higher (SAS Institute).
Results
Participants and treatment
From 177 eligible participants screened, 92 were enrolled between September 2013 and January 2014 (Fig. 1) and randomized into the two groups (tuina n = 46 and no intervention control n = 46). The average age was 45.4 ± 9.7 (mean ± standard deviation) years, 87.0% were female, and the mean duration of symptoms was 11.4 ± 10.2 years. At baseline, the average pain intensity on the VAS was 57.7 ± 11.5 mm. 77.2% of participants had already consulted a physician because of neck pain, mostly orthopedic surgeons (57.6%), and 53.3% reported concomitant diseases, most frequently hypothyroidism (13) and hypertension (11). For other baseline characteristics, see Table 1. We did not observe relevant differences between study groups at baseline. Patients in the tuina group received 5.3 ± 1.2 treatments. Three patients in the waiting list group refused further participation after randomization and were consequently lost to follow-up at week 4. Follow-up data after 12 weeks were available for 89 patients (tuina n = 46 and waiting list n = 43, Fig. 1).
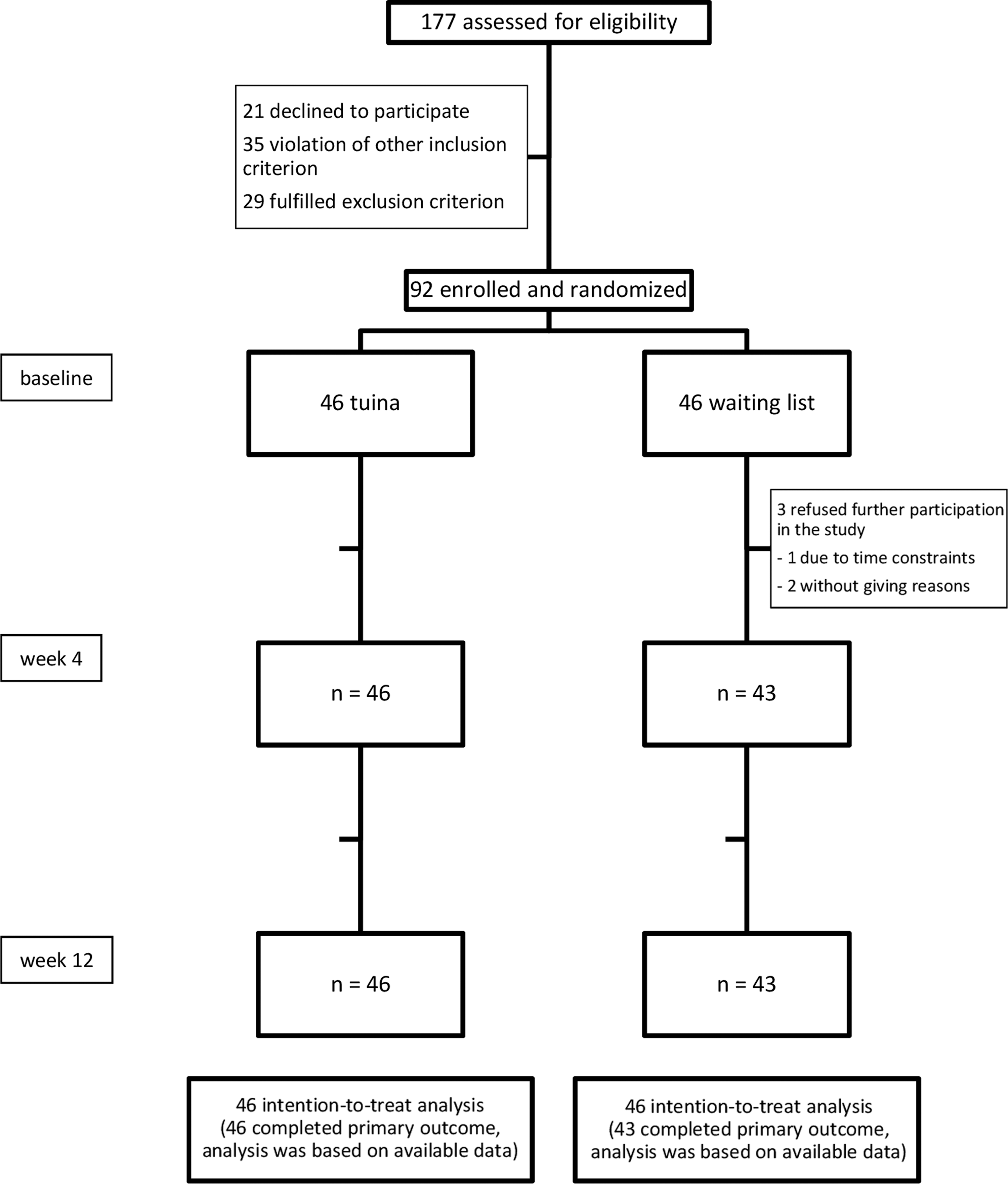
Recruitment, treatment, and follow-up of patients with chronic neck pain.
Lower values indicate better status.
Higher values indicate better status.
BMI, body mass index; NDI, Neck Disability Index; NPDS, Neck Pain Disability Scale; SD, standard deviation; SF-12, 12-item quality-of-life questionnaire; VAS, visual analogue scale for assessing the average low-back pain intensity.
Outcomes
Both groups showed a reduction of pain after 4 and 12 weeks compared to baseline (Table 2). The primary outcome, mean average neck pain intensity (VAS during the previous 7 days) after 4 weeks, was statistically significantly different between both groups (adjusted group difference −22.8 mm [95% confidence interval −31.7 to −13.8]; p < 0.001; Table 2). The average pain intensity after 12 weeks also differed significantly between both groups, although less pronounced than after 4 weeks (Table 2). The effect size (Cohen's d) 25 for the average pain intensity difference between tuina and no-intervention group was large according to Cohen with d = 1.16 after 4 weeks and d = 0.92 after 12 weeks, respectively. Results from the sensitivity analyses confirmed the results (data not shown).
Lower values indicate better status.
Higher values indicate better status.
CI, confidence interval; NDI, Neck Disability Index; NPDI, Neck Pain Disability Index; QALYs, quality-adjusted life years; SF-12, 12-item quality-of-life questionnaire; VAS, visual analogue scale for assessing the average low-back pain intensity.
Furthermore, we observed significant differences in favor of tuina for the physical aspect of quality of life measured by SF-12, neck function (measured by NPDS and NDI) after 4 and 12 weeks, and medication intake after 4 weeks (Table 2). The mental health subscale of SF-12, body efficacy expectation at weeks 4 and 12, and medication intake at week 12 did not show significant differences (Table 2). Accompanying therapies, including concurrent therapies, were not significantly different between both groups.
Safety data
Of the 46 patients in the tuina group, 19 reported mild suspected adverse reactions such as “aching muscles” (11 times), tensions (5), dizziness (4), headache (3), sleepiness (2), mood swings (1), “painful point” (1), difficulties staying asleep (1), slight nausea (1), and “head not movable” (1). None of the patients had to stop the therapy because of adverse reactions. In five patients, self-treatment, but not professional treatment, was necessary. No serious adverse events were observed.
Costs and cost-effectiveness
Tuina and conventional care were comparable in terms of total costs and QALYs during the study duration (Table 2). The observed costs and QALY differences between the groups were not statistically significant. After considering the adjusted group differences independently from their statistical significance, tuina seems to be cost-effective. Depending on the assumed cost-per-tuina session scenarios, the costs per QALY gained (ICER) range within a cost-effective area from 7,566 € (for scenario 1 that had assumed 10.28 € per session) to 39,414 € (for scenario 2 with 35 € per session).
Discussion
We observed that six sessions of tuina led to a clinically relevant 26,27 reduction in mean neck pain intensity and an improved function and physical quality of life compared to the no-intervention control group. Tuina treatment was relatively safe and presumably cost-effective.
The main strengths of this trial are the randomized study design, the relatively large sample size for a single-center interventional trial on tuina, high adherence and follow-up rates, and the broad range of patient-reported outcomes, including pain, function, quality of life, medication intake, and self-efficacy. Furthermore, we performed an economic analysis. We aimed to answer a research question that has relevance for usual care practice and reflects a German setting. Therefore, a German therapist with a background in physiotherapy and additional tuina training applied the therapy.
However, our single-center study setting, the involvement of only one therapist with very specific training, and the high percentage of women in our study population clearly limited the generalizability of our results. The study design had more potential sources of bias: the intervention group received more attention than the control group and the participants were not blinded. The intervention and follow-up time were comparably short, yet chosen to reduce the complexity of the study and ease the recruitment and adherence of patients. The short duration might be one of the reasons for the high adherence and follow-up rates. Although the treatment was safe, when interpreting our safety results, one should take into account that no HVLA (thrust) techniques were applied during the tuina treatment in our study because of safety concerns.
Unfortunately, we did not apply diaries to evaluate pain and function on a daily basis. Diaries would allow the evaluation of the optimal length (dosage) of a tuina cycle, which greatly impacts the cost-effectiveness of tuina. Ideally, tuina should be evaluated within a complex therapy regime that might also include exercise, behavioral change techniques, and medication. 9 Another design option would have been a head-to-head comparison with other best care options. However, in view of scarce evidence for tuina and neck pain in the West, we decided to compare tuina to a no-intervention waiting list control as a first step. A future trial on tuina should include multiple centers, therapists with a different level of training, a comparison with other best care options, a longer follow-up duration, and a more balanced sample regarding gender.
Although numerous studies on tuina can be found, data on the efficacy and effectiveness of tuina for neck pain are still scarce and, to our knowledge, no cost data were available so far.
A recent meta-analysis on Traditional Chinese Medicine for neck pain and low-back pain by Yuan et al. 11 could not include RCTs on tuina due to lack of eligibility and concluded that the efficacy of tuina for neck pain is unknown. Earlier meta-analyses on massage therapy by Kong et al. 28 and by Cheng and Huang 10 included 12 and 14 studies, respectively. While Kong et al. did include three studies on Chinese traditional massage, Cheng and Huang included seven in their meta-analyses. According to them, the effects of massage therapy on neck pain, including tuina, the evidence is sufficient for short-term relief of pain, especially in comparison to inactive therapies such as a self-care book. While there is no sufficient evidence for its effects on dysfunction or follow-up effects after 6 or 12 weeks, in the setting we had chosen, we observed clinically relevant effects on pain and dysfunction after 4 and 12 weeks, as well as effects on medication intake after 4 weeks.
Pain relief due to tuina might be caused by mental components, such as expectation, which lead to a placebo effect, as well as physical components, such as the modulation of local blood circulation, loosing of adherent connective tissue, and improved reuptake of local nociceptive and inflammatory mediators. Both components can modulate central pain perception. 28 –33
To conclude, six sessions of tuina treatment within 3 weeks were beneficial for patients with chronic neck pain, resulting in relevant pain relief. Effects were still maintained after 12 weeks. Total patient-related costs as well as effects in terms of QALYs were comparable and indicate the cost-effectiveness of tuina in our study. A future trial should compare tuina to other best care options.
Footnotes
Acknowledgments
We thank Beatrice Eden and Iris Bartsch for data acquisition, Annette Wagner for coordinating appointments, Jin Li for additional input, Stephanie Roll for statistical advice during the planning of the study, and all patients for their participation in this study. This study was an investigator-initiated trial and had no extra funding.
Authors' Contributions
Conceived and designed the trial: C.M.W., D.P., G.R., M.P., and T.R. Performed the trial: C.M.W., D.P., and M.P. Analyzed and discussed the data: C.M.W., D.P., F.L., K.I., Y.C., B.L., and M.D. Wrote the first draft of the paper: D.P., Y.C., and K.I., revised the paper and approved the final version: C.M.W., D.P., F.L., G.R., K.I., M.P., S.B., Y.C., B.L., T.R., and M.D.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.